
Abstract
Cryotherapy is the application of a stimulus of a cryotherapeutic temperature below −100 °C in a period of 1–3 min in order to stimulate and use physiological reactions of human body to cold. It can be applied to specific body parts or to a whole body. Whole-body cryotherapy is a treatment method applied in treatment of motor organ issues, nervous system diseases, psychiatry, dermatology and laryngology. The research group consisted of 80 male in the age range of 65–77 suffering from chronic, lasting more than 3 months, lower back pain. The subjects qualified to the research were divided into two groups. Group A consisted of 40 patients who participated in whole-body cryotherapy (WBC) twice a week. Group B also contained 40 patients who participated in WBC whole week. Examinations were conducted twice. The first one was conducted before the commencement of the treatment while the second one after the therapy was over. The results of the research did not show any statistically significant improvement in patients from Group A. However, the results obtained by Group B have proven significant condition improvement and enable the researchers to conclude that WBC is effective in treating patients with lower back pain.
Introduction
Cryotherapy is the application of a stimulus of a cryotherapeutic temperature below −100 °C in a period of 1–3 min in order to stimulate and use physiological reactions of human body to cold. It can be applied to specific body parts or to a whole body.
Whole-body cryotherapy is a treatment method applied in treatment of motor organ issues, nervous system diseases, psychiatry, dermatology and laryngology.
The research group consisted of 80 male in the age range of 65–77 suffering from chronic, lasting more than 3 months, lower back pain. The subjects qualified to the research were divided into two groups. Group A consisted of 40 patients who participated in WBC twice a week. Group B also contained 40 patients who participated in WBC whole week. Examinations were conducted twice. The first one was conducted before the commencement of the treatment while the second one after the therapy was over.
The results of the research did not show any statistically significant improvement in patients from Group A. However, the results obtained by Group B have proven significant condition improvement and enable the researchers to conclude that WBC is effective in treating patients with lower back pain.
An interest in whole-body cryotherapy is becoming greater with each year. Cryotherapy is the application of a stimulus of a cryotherapeutic temperature below −100 °C in a period of 1–3 min in order to stimulate and use physiological reactions of human body to cold [Citation1]. It can be applied to a whole body or to its specific parts.
Systemic cryotherapy is an important treatment method applied in treatment of not only motor organ issues but also nervous system diseases, psychiatry, dermatology and laryngology [Citation2]. Applied in wellness and sports medicine WBC helps maintaining good health condition of healthy people. Clinical results of cryotherapy include: pain relief [Citation3,Citation4] and reflexive congestion of skin and limbs [Citation5], which leads to faster healing of wounds. It has anit-oedematous and anti-inflammatory effect [Citation6,Citation7], reduces muscle tone [Citation8,Citation9], increases muscle strength [Citation10–12], improves mood [Citation13], and additionally has a strong influence on physical capacity [Citation14,Citation15] and the ability to intensify the healing process [Citation1].
The existing knowledge does not explain all the aspects of the effect of low temperatures on human body. Articles presenting the effects of whole-body cryotherapy on the human body are ambiguous and divers. Despite an increasing number of scientific research tackling an issue of the influence of WBC on the human body it needs to be emphasized that their results are very often insufficient and sometimes contradictory [Citation1,Citation16]. Moreover, most of the research is conducted on young subjects.
There are very few research papers in world literature which describe the influence of WBC on elderly people and the results of those treatments applied to specific aliments. Based on a review of the available articles, it can be concluded that WBC is a safe procedure [Citation17]. However, researchers should carefully select patients subject to WBC (especially elderly people) as well as abide the limitations and conduct WBC according to its procedures. Assuming that the WBC treatment in an examined group of patients requires outmost caution in regard to their age the authors tried to determine a dosage of a WBC stimulus which would be the most effective and safe for the examined group of patients.
Unfortunately, there is a big difference in methodology applied by the users of cryotherapeutic chambers which can be reflected in the number of treatments in series, frequency of treatments, duration of a single treatment and applied range of temperatures. Hence, it is necessary to conduct research which would describe a detailed influence of WBC procedures on the human body. Therefore, the researchers tried to determine the frequency of WBC treatments effective in therapy. It was assumed that WBC procedures will have a positive effect in lower back pain treatment.
Materials and methods
The research group consisted of 80 male in the age range of 65–77 (mean 70.1) suffering from chronic, lasting more than 3 months, lower back pain. The subjects were chosen on the basis of interviews which enabled researchers to determine the characteristics of the pain and its duration. The cause of pain was established on the basis of an objective tests results of X-ray and MRI.
The patients excluded from the research suffered from an acute pain ailments, damage to nerve roots (Laseqeu’s sign of sensory disturbance, paresis) or different diseases, such as irregular hypertension, osteoporosis or circulatory failure. There were also patients who were unable to participate in the whole-body cryotherapy due to health conditions. The current knowledge enables us to determine the following limitations: claustrophobia, cold intolerance, Raynaud’s disease, hypothyroidism, acute respiratory disease, cancer, cardiovascular diseases (unstable angina pectoris, aortic valve stenosis or venous stenosis of the left mouth, circulatory failure, dangerous arrhythmias) gangrenous skin lesions, sympathetic neuropathies, local circulatory disorders, emaciation and hypothermia [Citation1,Citation18].
The subjects qualified to the research were randomly divided into two separate groups.
Group A consisted of 40 patients who participated in WBC twice a week on Tuesdays and Fridays. Group B also contained 40 patients who participated in WBC whole week from Monday to Friday. Examinations were conducted twice. The first examination was conducted before the commencement of the therapy (Examination 1) while the second (Examination 2) was a day after the 3-week course. The whole-body cryotherapy treatments were conducted in a Cryogenic chamber type CR 2002, which consisted of a vestibule and main chamber (). with treatment lasting 3 min. When a subject entered the vestibule, they spent there approximately 30 s at a temperature of −60 °C to adapt to the cold. Next, the subject moved to the main chamber. At a temperature −120 °C they spent another 3 min, during which they were subject to the proper whole-body cryotherapy. After the procedure, the subjects left the chamber and went to a gym. The subjects performed the same therapeutic exercises 5 d a week, 45 min a day for a period of 3 weeks, with all exercises being supervised by a qualified physiotherapist. During the research, none of the patients used other physical therapy or applied pharmacological treatment.
Figure 1. Cryo chamber.

All measurements (mobility measurements and EMG recordings) were taken by the same person and at the same time of day. Also, the overall testing conditions (humidity, lighting and temperature) were kept constant for all measurements.
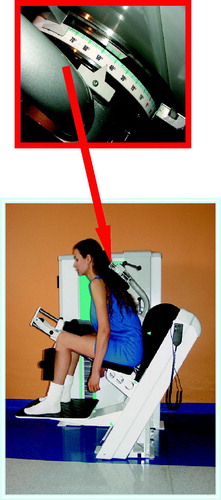
The research evaluated the lumbar spine mobility. The measurements of: active flexion and extension, rotation to the right and left, and lateral flexion to the right and left were taken. Spine mobility was measured by the use of devices applied in a DBC method devices are used in functional diagnostics and therapy. Their construction enables the performance of a movement of a selected part of the spine. Each device equipped in a build-in supporter enabled complete lower limb stabilization and facilitated precise performance of a movement. An angle scale embedded in each device made it possible to measure the mobility of the spine. In order to maintain constant measurement conditions, the settings of the devices were recorded on a magnetic card owned by each subject (height of a seat, feet supporting platform, etc.) [Citation19].
Measurement of active flexion and extension of the lumbo-thoracic spine [19]
The measurement of a movement in the sagittal plane was conducted by the use of the device with the symbol LTE (). During that measurements, the subject remained in a sitting position and their feet were placed on a platform. In order to eliminate compensatory movements, researchers adjusted the height of the platform for each subject. They used the mechanism to stabilize hip joint inflexion. Thighs and pelvis were supported by cushions preventing those body parts from rotating. The range of movement was measured by the measurement system set at the height of the spine at the scapula. Upon a signal, the subject performed maximum flexion until reaching the first sensation of pain, then maximum extension to the same extent. Angle values were taken from a scale attached to the device.
Figure 2. Device LTE for applied in the research.
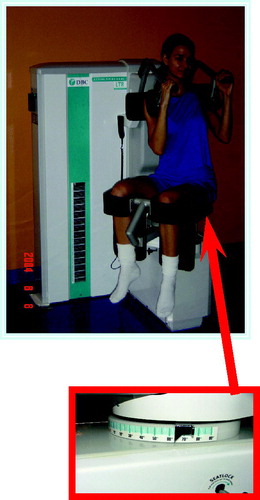
Measurement of an active rotation of the lumbo-thoracic spine [19]
The measurement of a movement in the transverse plane was conducted by the use of the device with the symbol LTR (). During that measurements, the subject remained in a sitting position. The angle between the thighs and trunk was 90°. This position was stabilized by the mechanism. The shoulders of the subject were stabilized by pads which prevented the subject from moving the upper part of the thoracic spine. Upon a signal the subject performed a maximum rotation to the right and then to the left until the first sensation of pain. Angle values were taken from a scale attached to the device.
Figure 3. Device LTR for applied in the research.
Measurement of an active side bend of the lumbo-thoracic spine
The measurement of movement in the frontal plane was conducted by the use of the device with the symbol LTL [Citation19] (). During that measurements, the subject remained in a sitting position. The angle between the trunk, thighs and lower leg was 90° and the feet rested on a platform. The feet rested on the platform. The seat was adjusted to each subject, so the rotation axis for all was within the area of the L2 vertebra. The subject was stabilized in that position by a suitable mechanism, an applicator at the height of shoulders. Upon a signal the subject performed a maximum rotation to the right and then to the left until the first sensation of pain. Angle values were taken from a scale attached to the device.
Figure 4. Device LTL for applied in the research.

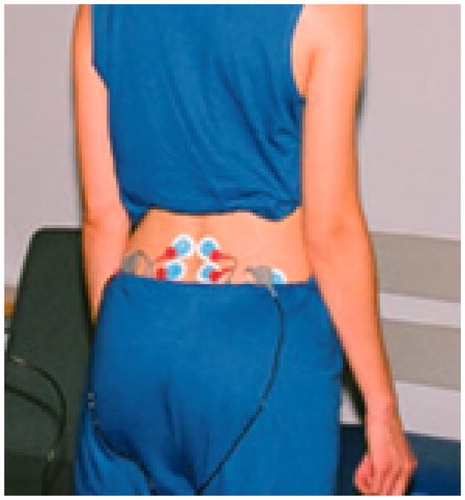
EMG measurement of erector spinae in the lumbar part of the spine performed at rest and in flexion. The area to be examined was shaved and cleaned with an abrasive paste and alcohol in order to decrease skin resistance. During the placement of electrodes, the patient’s body was slightly leaned forward which facilitated optimum placement of electrodes on the skin for the examination. Electrodes were places symmetrically on both sides of the lumbar spine. The first set of the electrodes was attached at the level of L4 and L5 vertebra, while the second was placed at a greater distance from the spine at the level of L5 and S1 (). In order to obtain a comparable EMG signal, researchers used the same conditions for both sets of electrodes (the same resistance between electrodes and signal amplification, and constant distance between electrodes).
Figure 5. The placement of EMG electrodes.
Static EMG examined the lumbar erector spinae muscles separately on the right and on the left side. The research was conducted in a free-standing position and at maximum flexion and maximum extension. The researchers used a questionnaire which helped them take into account subjective parameters such as: a pain scale by the use of Visual Analogue Scale (VAS) and functional limitations determined by ADL (Activities of Daily Living). Since we are aware about the influence of fatigue on EMG time and domain analysis parameters, we controlled the measurements procedures to avoid an occurrence the fatigue. The static EMG recordings were taken during non-fatigue 5-s periods, divided by 5-minute breaks that did not cause any fatigue in tested subjects. All EMG recordings were conducted when the subject felt relaxed without any prior experienced physical exercises. The EMG recordings were performed using the DBC surface EMG hardware and software. The stable static 5-s recordings were collected for each condition (standing, flexion and extension) after the required subject’s position was correctly set. The DBC EMG software performed automatic calculation of the EMG amplitude, as the RMS (root mean square) from these 5-s periods. The estimation of EMG amplitude (RMS) is appropriate parameter to reveal any neurophysiologic changes related to muscle tone alterations in the context of diagnosis and monitoring of therapy effectiveness. Researcher performing the EMG recordings controlled strictly the stability of the testing conditions, e.g. when the EMG recording was performed during the trial with inaccurate body position or with body movement, that trial was discarded and performed once again. Taking into account the literature data with EMG amplitude analysis using RMS parameter, these 5-s periods are enough time frames to obtain reliable estimate of the EMG amplitude. In many studies, authors use 1-s periods and it gives reliable EMG results.
The evaluation of patient response was based on the evaluation of actual pain measured at the beginning and end of the research. Pain was evaluated on the basis of VAS from 0 to 100 mm. Patient’s task was to evaluate the intensity of the pain regardless of the level of physical fitness. The patient had to put an “x” on the scale where the left extreme meant “no pain” while the right “the strongest pain”. At the beginning and end of research, researchers evaluated patients’ functional limitations (ADL). To accomplish this, they used a scale from 0 to 3 points: 0 stood for “I don’t have any problems with that activity” while 3 meant “I can’t do it”. A subject selected the number which corresponded to their ability to perform each activity listed on the questionnaire.
Statistical analysis was performed by the use of Statistica 9 PL software (StatSoft, Inc., Tulsa, OK). Both Shapiro–Wilk and Levene’s tests were applied to check normal distribution and homogeneity of variance. Since the obtained results revealed abnormal distribution the Mann–Whitney U test was used to compare the results obtained for both groups. The Wilcoxon signed-rank test evaluated the efficacy results of the therapy for each group. Statistical significance observed was p < 0.05.
Results
present statistical analysis of the results obtained in the research. Values presented in taken for both groups before the beginning of a treatment show no significant differences between the mean values of the examined active parameters of the lumbar spine, values of active potentials of erector spinae in the lumbar part of the spine and subjective pain parameters. This suggests that the function of the spine, subjective feeling of pain and the level of functional difficulties were at the same level.
Table 1. Mean values of the analyzed parameters and differences observed between the analyzed groups – examination 1.
Table 2. Mean values of the analyzed parameters and differences observed between the analyzed groups – examination 2.
Table 3. The efficacy of the therapy for the examined groups.
The results obtained in the second examination after the cycle of therapeutic treatment are presented in . The analysis of these parameters reveals statistically significant differences between the examined groups in all the parameters but the level of functional difficulty. The patients who exercised and participated in whole-body cryotherapy five times a week showed significantly lower values of active potentials of erector spinae muscles in the lumbar part of the spine and a significant increase in the range of the lumbar spine mobility. The level of pain was also significantly decreased. However, the researchers did not observe any changes at the level of functional difficulty caused by pain.
contains the results of the comparative analysis of therapy efficacy for both groups. The analysis of the results of the examinations conducted at the beginning and at the end of the therapy did not reveal any significant differences in Group A. However, statistically significant differences observed in Group B enable the researchers to conclude that only systematic WBC is effective in treating patients with lower back pain.
Discussion
This research aimed to determine the frequency of WBC treatments, which along with exercise, have positive influence on the improvement of the functional condition of elderly men suffering from lower back pain. The simple measurement methods applied in the study enabled the determination of lumbar spine activity and patients’ sensations. The methods can easily be used in any therapeutic facility.
Approximately 50% of adults suffer from lower back pain [Citation20]. It is a long-lasting ailment causing significant movement limitation, including that related to performing sports. It is especially significant in the case of elderly men. On one hand, involutionary processes occurring with age deteriorate the functional capabilities of the human body and lead to an increase in the percentage of people with limitation of movement. On the other hand, the limitations caused by lumbar spine ailments limit the abilities of people suffering from lower back pain. The limitations of physical activity which accompany these disorders, especially in old age, may be related to many health issues associated with motor organs and other important human systems. Impaired function of the cardiovascular and respiratory systems and those related to changes in motor organs [Citation21] have a negative influence on the impairment on many activities necessary to independent functioning in everyday life [Citation22]. They also lead to a decrease in physical performance [Citation21]. Long-lasting pain may also lead to depression [Citation23]. Pain related to this problem [Citation23] causes significant limitations to the movement possibilities of patients. Many patients with chronic lumbar pain suffer from so-called deconditioning and have a tendency to avoid movement. Evading movement is caused by the fear of an increase in pain. The decrease in daily physical activity related to age and chronic lumbar pain leads to an impairment of physical abilities, decrease in the range of movement, loss of muscle strength and deterioration of motor coordination [Citation24,Citation25].
Thus, researchers keep searching for new, effective measures which will decrease existing ailments and limit their recurrence. They also hope to increase the physical activity of people. Physiotherapy programs not only decrease lower back pain but are also a form of physical activity. The authors of this research hope that the therapeutic effect of the performed exercises will also encourage the patients to stay physically active.
One of the barriers which has existed for many years and is a named form of limitation in the improvement process of elderly people is the fear of pain associated with motor organs [Citation25,Citation26]. Studies conducted for many years revealed the efficiency of physical exercise improving patients suffering from sub-acute and chronic pain [Citation27–29]. It is commonly known that physical exercise brings excellent results in pain treatment related to motor organs [Citation29]. It enables an increase in: the range of joint movement, muscle strength and physical fitness. Regular physical effort extends the period of independence and improves the lifestyles of elderly people [Citation26,Citation30].
Due to the application of physical therapy, especially those with analgesic, anti-inflammatory and relaxing properties, it is possible to intensify kinesitherapy. WBC is a treatment which, thanks to its analgesic and anti-inflammatory properties [Citation6,Citation7], can be classified as a treatment supporting lumbar pain therapy.
The analgesic and anti-inflammatory effects of WBC have been described in many research papers. Lange et al. [Citation6] and Algafly et al. [Citation7] have proven the anti-inflammatory and analgesic activity of these treatments. The anti-inflammatory effect of WBC may result from the influence of low temperatures on the production of inflammatory mediators, as well as pro-oxidant–anti-oxidant balance. It is important in the treatment of nociceptive pain which is observed in spinal pain syndrome [Citation31–33].
The efficacy of WBC applied in the treatment of a range of diseases has been presented in many papers. The examples presented herein confirm the results obtained by those authors for Group B. Hirvemen et al. [Citation34] and Metzger et al. [Citation35] used cryotherapy treatment on patients with rheumatoid diseases and observed a significant decrease of pain in those patients. Offenbacha et al. [Citation36] and Bettoni et al. [Citation37] have established an analgesic influence of WBC on patients suffering from fibromyalgia.
The improvement of spine mobility observed by the authors may be related to a decrease in pain, the values of active potentials of erector spinae muscles in the lumbar part of the spine or the positive influence of WBC treatments on inflammation reduction. These factors enabled the patients from Group B (five treatments) to intensify the process of improvement through the increase of work load during exercises and improvement of their range of movement, resulting in better final results. A study performed by Stanek et al. [Citation18] on AS patients treated with whole-body cryotherapy showed improved spinal movement and muscle relaxation. Moreover, results obtained by Rymaszewska et al. [Citation13] proved the positive influence of WBC in treatment of patients suffering from depression. Excessive and long-lasting pain observed in patients with lumbar spine ailments [Citation38] may lead to depression [Citation23]. So, the anti-depressant properties described by Rymaszewska and an increase in the level of β-endorphin after WBC reported by Zagrobelny [Citation1] may potentially improve a patients’ willingness to perform physical exercises and to have an influence on better treatment results.
The current research conducted by Bettoni et al. [Citation37] uses a standardized questionnaire to confirm the improvement in quality of life of patients with fibromyalgia using WBC as a treatment. In this research, the authors did not observe any improvement in the ADL parameter. This may have been caused by the short treatment period. Spine ailments are chronic. All abnormalities caused by long-lasting ailments become permanent for the time of the disease and may be difficult to alter in a 3-week therapy period.
The effectiveness of WBC therapy has been described many times. Those treatments have also proven effective in the treatment of lumbar pain in elderly people [Citation38,Citation39]. It is commonly known that a stimulus of extremely low temperature has a strong impact on the human body. Even a single treatment may disturb some functions of the human organism. Evaluation of healthy young people conducted by Giemza et al. after a single WBC treatment [Citation40] showed the imbalance. Lubkowska [Citation41] in her research on youth observed an increase in the systolic blood pressure right after the first day of WBC treatment. In her next paper [Citation42], she proved an increase of ISO-P-8 – marker of oxidative stress after the first WBC session. Smolander [Citation43] made observations about the decrease of FEV1 in young males, which had been subject to WBC treatments. Bearing in mind that WBC procedures may be used to treat elderly patients, one should consider the analysis of these results and pose the question whether a decrease of the number of treatments from five to two per week will bring the same results and be equally effective [Citation39].
An analysis of the results obtained from Group B, which consisted of patients who participated in the WBC treatment regularly five times a week, showed a significant improvement in almost all analyzed parameters. Such improvements were not observed in the group of patients who attended WBC sessions only twice per week. It was probably caused by the lack of positive body response to cryogenic temperatures. Anti-inflammatory properties of WBC treatments result from an influence of extreme cold on concentration of inflammatory markers and pro-anti-oxidant balance. These properties decrease a nociceptive pain occurring in degenerative joint diseases and spinal pain syndromes [Citation30–32]. WBC leads to muscle relaxation and increases pain tolerance, which enable to increase range of movements [Citation18].
Analgesic and anti-inflammatory effect, decrease in an excessive muscle tension and increase in a range of movements enabled subjects from Group B to increase a workload and intensity of the performed exercises. On the other hand, willingness to perform physical activities observed in that group might have been caused by an increase at the level of β-endorphins after the WBC treatments (Zagrobelny). All that could have led to obtaining better effects of the back pain treatment therapy observed in the results of Group B in comparison to those of Group A. An important part may have been played by the anti-depressant properties of WBC described by Rymaszewska et al. [Citation13] since chronic back pain may cause depressive states. The lack of improvement in patients from Group A may result from the fact that they failed to obtain a desirable result of WBC treatment due to its rare use. Hence, positive effects of this treatment did not overlap and did not bring positive effects at the end of the therapy.
Equally significant is a fact that only repetitive WBC treatments activate adaptive mechanisms which increase anti-oxidant capacity of organism and decreases oxidative stress. Lubkowska’s [Citation43] research has shown that a single WBC treatment causes changes in total and anti-oxidant plasma capacity.
Intensification of free-radical reactions caused by extreme cold leads to short and temporary pro-anti-oxidant imbalance. However, repetitiveness of the treatments activated adaptive mechanisms increasing anti-oxidant capacity of organism and readiness of protective mechanisms against oxidative damage [Citation44].
The presented results prove that only the regular application of WBC treatments is effective. It is common knowledge in physiotherapy that only treatments which are performed systematically within a certain period of time bring intended results. Due to that, the treatments performed one after another overlap and give positive effects. When the period between treatments is too long, positive results disappear and the procedures which occur next do not have a positive influence on a patient because they do not add up. The results presented in this research support this notion.
In recent years, there have been a number of studies dealing with the impact of WBC on the human body. Despite the large amount of research, the results are still ambiguous and incomplete [Citation39]. However, unequivocal criteria which would enable the classification of patients able to utilize WBC procedures have not been created yet. Also, there are no criteria which would determine the application of WBC treatments to patients of different ages. Thus, cryotherapy treatments applied to elderly people should be selected very cautiously and adjusted to their individual needs depending on the anticipated result. Staff performing the procedure should be well qualified and follow the procedures of such treatments.
In summary, it can be stated that systematic whole-body cryotherapy treatments are effective in treating people suffering from lower back pain. It is also safe for elderly people. Existing textbooks on WBC treat the age of 65 as the borderline for relative contradiction to using whole-body cryotherapy. However, this was written in the 1980s when whole-body cryotherapy was introduced to physiotherapy as a form of treatment. Its creators probably had in mind the safety of patients and the lack of research on that matter which could not influence their opinion.
The authors of this research are aware that the study does not contain information of the durability of positive effects of WBC treatments. But this matter is still under research and the obtained results will be presented after its completion.
Declaration of interest
The authors declare no conflicts of interests. The authors alone are responsible for the content and writing of this article.
References
- Zagrobelny Z. Local and whole body cryotherapy. Wydawnictwo Medyczne Urban Partner 2003;2:1–3
- Łuszczak J, Michalik J. Influence of extremely low temperatures on selected human motor activities. Fizjoterapia Polska 2006;6:206–11
- Sieroń A, Pasek J, Mucha R. Cryotherapy in rehabilitation. Rehabilitacja w Praktyce 2007;3:34–6
- Airaksinen OV, Kyrklund N, Latvala K, et al. Efficacy of cold gel for soft tissue injuries: a prospective randomized double-blinded trial. Am J Sport Med 2003;31:680–4
- Skrzek A, Anwajler J, Dudek K, et al. Thermovision examinations of body temperature distribution after systemic cryotherapy application. Acta Bio-Optica et Informatica Medica 2007;2:141–6
- Lange U, Uhlemann C, Müller-Ladner U. Serial whole-body cryotherapy in the criostream for inflammatory rheumatic diseases. Med Klin [Munich] 2008;103:383–8
- Algafly AA, George KP. The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance. Br J Sports Med 2007;41:365–9
- Mead S, Knott M. Topical cryotherapy. Use for relief of pain and spasticity. California Med 1996;105:179–81
- Kwolek A, Pabis M. Influence of extremely low temperatures on selected human motor activities. Fizjoterapia Polska 1998;6:17–19
- Evans T, Ingersoll C, Knight KL, Worrell T. Agility following the application of cold therapy. J Athletic Train 1995;30:231–4
- Ruiz DH, Myrer JW, Durrant E, Fellingham GW. Cryotherapy and sequential exercise bouts following cryotherapy on concentric and eccentric strength in the quadriceps. J Athletic Train 1993;28:320–3
- Skrzek A, Woźniewski M, Zagrobelny Z, Lisowska M. Changes of speed force parameters of muscles under the influence of whole body cryotherapy. Fizjoterapia 2001;9:12–17
- Rymaszewska J, Ramsey D. Whole body cryotherapy as a novel adjuvant therapy for depression and anxiety. Arch Psychiatr Psychotherap 2008;2:49–57
- Chwalbińska-Moneta J. Influence of whole-body cryotherapy on selected reactions to physical effort in athletes. Sport Wyczynowy 2003;5–6:50–4
- Zimmer K. Whole-body cryotherapy in sport medicine. Sport Wyczynowy 2003;5–6:43–9
- Korzonek-Szlacheta I, Wielkoszyński T, Stanek A, Świętochowska E. Influence of whole body cryotherapy on the levels of some hormones in professional footballers. Pol J Endocrinol 2007;1:27–32
- Bonomi FG, De Nardi M, Fappani A. Impact of different treatment of whole body-crytherapy on circulatory parameters. Arch Immunol Ther Exp 2012;60:145–50
- Stanek A, Cieślar G, Matyszkiewicz B, et al. Subjective estimation of therapeutic efficacy of whole-body cryotherapy in patients with ankylosing spondylitis. Balneologia Polska 2005;1–2:s.24–32
- Giemza C, Kabala T. DBC – a system of active therapy of the spine. Fizjoterapia 2007;15:1,55–66
- Deyo RA. Fads in the treatment of low back pain. New Engl J Med 1991;325:1039–40
- Allen C, Glasziou P, Del Marc C. Bed Rest: a potentially harmful treatment needing more careful evaluation. Lancet 1999;354:1229–33
- Greenleaf JE. Some evils of prolonged bed-rest deconditioning. Medicina Sportiva 2001;5:E77–95
- Sipko T, Kuczyński M. Intensity of chronic pain modifies postural control in low back patients. Eur J Pain 2013;17:612–20
- Leboeuf-Yde C, Klougart N, Lauritzen T. How common is low back pain in the Nordic population? Data from a recent study on a middle-aged genera Danish population and four surveys previously conducted in the Nordic countries. Spine 1997;22:877–81
- Cooper RG, St Clair Forbes W, Jayson MI. Radiographic demonstration of paraspinal muscle wasting in patients with chronic low back pain. Br J Rheumatol 1992;31:389–94
- Coleman EA, Buchner DM, Cress ME, et al. The relationship of joint symptoms with exercise performance in older adults. J Am Geriatric Soc 1996;44:14–21
- Hansen FR, Bendix T, Skov P, et al. Intensive, dynamic back-muscle exercises, conventional physiotherapy, or placebo-control treatment of low back-pain. A randomized, observer-blind trial. Spine 1993;18:98–108
- Manniche C, Hesselsoe G, Bentzen L, et al. Clinical trial of intensive muscle training for chronic low back pain. Lancet 1988;2:1473–6
- Mannion AF, Muntener M, Taimela S, Dvorak J. A randomized clinical trial of three active therapies for chronic low back pain. Spine 1999;24:2435–48
- Kostka T. Rola aktywności ruchowej w promocji zdrowia u osób starszych. Medicina Sportiva 2001;5:147–50
- Lubkowska A, Dołęgowska B, Szyguła Z. Whole-body cryostimulation-potential beneficial treatment for improving antioxidant capacity inhealthy men-significance of the number of sessions. PLoS One 2012;7:e46352
- Lubkowska A, Szyguła Z, Chlubek D, Banfi G. The effect of prolonged whole-body cryostimulation treatment with different amounts of sessions on chosen pro- and anti-inflammatory cytokines levels in healthy men. Scand J Clin Lab Invest 2011;71:419–25
- Banfi G, Melegati G, Barassi A, et al. Effects of whole-body cryotherapy on serum mediators of inflammation and serum muscle enzymes in athletes. J Thermal Biol 2009;34:55–9
- Hirvonen H, Mikkelsson M, Kautiainen H, et al. Effectiveness of different cryothepies on pain and disease activity in active rheumatoid arthritis. A randomized single blinded controlled trial. Clin Exp Rheumathol 2006;24:295–301
- Metzger D, Zwingmann C, Protz W, Jäckel WH. Whole-body cryotherapy in rehabilitation of patients with rheumaticdiseases – pilot study. Rehabilitation 2000;39:93–100
- Offenbächer M, Stucki G. Physical therapy in the treatment of fibromyalgia. Scand J Rheumatol 2000;113:78–85
- Bettoni L, Bonomi FG, Zani V, et al. Effects of 15 consecutive cryotherapy session no the clinical output fibromyalgic patients. Clin Rheumatol 2013;32:1337–45
- Ellegaard H, Pedersen BD. Stress is dominant in patients with depression and chronic low back pain. A qualitative study of psychotherapeutic interventions for patients with non-specific low back pain of 3–12 months. BMC Musculoskelet Disord 2012;13:166
- Giemza C, Matczak-Giemza M, Ostrowska B, et al. Aging Male 2013;Dec 5. [Epub ahead of print]
- Giemza C, Czech P, Paluszak A, et al. Acute effects of cryotherapy on postural control. Neurosci Lett 2013;536:6–9
- Lubkowska A, Szyguła Z. Changes in blond pressure with compensatory hart rate decrease and in the level of aerobic capacity in response to repeated whole-body cryostimulation in normotensive, young and physically active men. Int J Occup Med Environ Health 2010;23:367–75
- Lubkowska A, Dołęgowska B, Szyguła Z. Potential beneficial treatment for improving antioxidant capacity in healthy men – significance of the number of sessions. PLoS One 2012;7:e46352
- Lubkowska A, Chudecka M, Klimek A, et al. Acute effect of a single whole-body cryostimulation on prooxidant-antioxidant balance in blood of healfy, young men. J Therm Biol 2008;33:464–67
- Woźniak A, Woźniak B, Drewa G, Mila-Kierzenkowska C. The effect of cryostimulation on the prooxidant-antioxidant balance in blood of elite kayakers after training. Eur J Appl Physiol 2007;101:533–7