
Abstract
A cross-sectional study was conducted to explore the prevalence and severity of health-related complaints perceived by adult males of Hong Kong by using the Hong Kong Traditional Chinese versions of the Aging males’ symptoms (AMS) scale and the 5-dimensional and 3-level European Quality of life (EQ-5D-3L) questionnaire. A total of 825 adult males aged 40 years or above were surveyed, and observed that 80% of the population was living with little-to-mild levels of aging symptoms with mean total scores ranged between 26.02 ± 7.91 and 32.99 ± 7.91 in different age groups. Such symptoms were correlated with age, especially for the somato-vegetative and sexual symptoms. The most severe AMS symptoms were observed in the oldest age group at 70 years or above, with 76%, 34% and 70% living with moderate-to-severe levels of somato-vegetative, psychological and sexual symptoms, respectively. The result was highly correlated with the EQ-5D-3L questionnaire. Secondly, the Hong Kong Aging males’ symptoms (AMS) scale was shown to have good reliability with test–retest coefficient at 0.79 (ranged 0.66–0.87) and Cronbach’s alpha coefficient at 0.88 (ranged 0.70–0.84). In summary, the population of Hong Kong male adults was commonly living with little-to-mild levels of aging symptoms, whereas their severity was correlated with age.
Introduction
The “Aging males” symptoms (AMS) scale’ is an internationally well accepted instrument originally developed in Germany in 1999, for measuring the severity of aging symptoms and their impact on health-related Quality of Life (HRQoL) in males [Citation1]. There are 29 validated versions of different languages available in its official website (www.aging-males-symptoms-scale.info). They were widely used in different national [Citation2] and international [Citation3] male aging surveys to detect symptoms that might suggest testosterone deficiency syndrome. Many researchers measured the AMS in different health conditions, e.g. the Finnish middle aged population with adverse mental symptoms [Citation4], Japanese hospital outpatients with major depressive disorder [Citation5] and Taiwanese psychiatric outpatients [Citation6].
It is reported that Hong Kong has an aging population, where males’ average life expectation has been increased from 72.3 years in 1981 to 81.2 years in 2014. With the increased lifespan, men’s health becomes more and more important nowadays. However, the aging symptoms of males have never been systematically investigated in Hong Kong. Currently, two Chinese versions are available for the AMS scale – the Taiwanese [Citation7] and Chinese [Citation8] versions. Due to the geographical and language differences, the two existing Chinese versions were found unsuitable to be used in Hong Kong where Traditional Chinese characters are used and Cantonese (the dialect of Yue Chinese) is spoken in the City, while Taiwan and Mainland China adopted Mandarin as the sole official language and Simplified Chinese characters are used in Mainland China. Therefore, in the present study, we measured the community-based prevalence of aging symptoms and health-related quality of life in Hong Kong using the “Hong Kong Traditional Chinese AMS” scale and “Hong Kong Traditional Chinese 5D and 3-level European Quality-of-life (EQ-5D-3L)” questionnaire.
Methods
Study design
This is a cross-sectional study to explore the prevalence and severity of health-related complaints perceived by adult males who were aged 40 or above and living in Hong Kong. Secondarily, the Hong Kong Traditional AMS scale was measured in parallel with the EQ-5D-3L (the Hong Kong traditional Chinese version) scale, which is widely used for measuring the health status applicable to various health conditions.
Participants and recruitment
The target population of this study was adult males of Hong Kong. The criteria for inclusion were males aged 40 years or above, and residents of Hong Kong who were staying for longer than 180 days prior to the recruitment. Those who could not understand and speak Cantonese or foreign domestic helpers living in Hong Kong were excluded. In the middle of 2014, there were 1 821 400 males (which accounted for 54.5% of the Hong Kong male population) eligible to participate in this study. Among the 18 districts of Hong Kong, residential areas of 13 districts were surveyed, except the border districts, rural areas and remote islands. During the summer of 2014, between July and August, nine data collectors were allocated to visit at different public parks and recreation facilities located near the residential areas of the sampling districts, at different time slots, that is, 07:00–10:00 h in morning, 14:00–17:00 h in afternoon, and 18:00–21:00 h at night. Each data collector spent 3 h at each allocated spot at each visit, and five to six questionnaires were completed on an average per hour. In case of non-response, next individual was approached and callbacks were not implemented. After confirming the eligibility, the nature and purpose of the study was verbally explained then the individual was invited for completing the set of questionnaires. Completion of the survey was considered as an implied consent of participation. No personal information involving identity was collected in the survey. Ethical approval has been obtained from the University Human Ethics Sub-committee of the Hong Kong Polytechnic University.
The instruments
The questionnaire used in this survey was established by combining the two internationally well-accepted scales, namely, the Hong Kong Traditional AMS scale and the Hong Kong traditional Chinese version of EQ-5D-3L.
The Hong Kong Traditional Chinese AMS scale was translated from the English version of the AMS scale (as obtained from the official website http://www.aging-males-symptoms-scale.info/documents/AMS_English.pdf) through the translation and back-translation process conducted by a expert panel of medical professionals and two independent bilingual translators. The instrument consists of 17 items to measure the male symptoms/complaints associated with aging in three dimensions, namely, the somato-vegetative, the psychological and the sexual factors. The scoring scheme is based on the 5-point Likert scale (from 1 to 5) of “severity” for each of the items reflecting the personal perception of the respondent. The composite score ranged between 17 and 85, is calculated by summing up the scores of all 17 items. While the dimension scores of the subscales are calculated by summing up the scores of corresponding items, i.e. somato-vegetative dimension score ranged between 7 and 35 (items 1, 2, 3, 4, 5, 9 and 10), psychological dimension score raged between 5 and 25 (items 6, 7, 8, 11 and 13) and sexual dimension score ranged between 5 and 25 (items 12, 14, 15, 16 and 17). To determine the test–retest reliability, 24 age-matched adult males were recruited in the Urology Clinic of Prince of Wales Hospital. The 14-day test–retest coefficient was found to be 0.79 for the 17-item AMS scale, and ranged between 0.66 for somato-vegetative subscale, 0.69 for psychological subscale and 0.87 for sexual subscale, which were acceptable. Furthermore, Cronbach’s α reliability analysis on the data collected from the sampled population (n = 825), the Hong Kong Traditional Chinese AMS scale was found to be highly reliable with α = 0.88 for all 17 items and the α values for somato-vegetative, psychological and sexual subscales were 0.85, 0.70 and 0.80, respectively.
The Hong Kong traditional Chinese version of EQ-5D-3L was obtained from the EuroQol Research Foundation after completing the registration process at the official website (Appendix 1). This instrument consists of five dimensions, namely, mobility, and self-care, usual activities, pain/diskomfort, and anxiety/depression. The respondent was asked to indicate one of the three levels (no problem, some problems and extreme problems). In addition, the EQ-5D-3L also includes the EQ visual analog scale (VAS) that records the respondent’s self-rated imaginable health state from 0 (the worst) to 100 (the best).
Data processing and statistical analysis
Data collected from the survey were analyzed using IBM SPSS version 21.0 (Armonk, NY) and GraphPad Prism version 3.02 (San Diego, CA). Descriptive statistics (frequency and percentages) were used to describe the demographics, medical conditions, severity of aging symptoms of males and levels of quality of life domains. Chi-squared test and one-way ANOVA test were used to compare nominal variables and mean values among multiple groups, respectively. Linear correlation between two variables was assessed using the Pearson’s correlation analysis.
Results
Aging males’ symptoms among the Hong Kong male adults
During the data collection period from July to August 2014, a total of 825 adult males who were eligible for inclusion in the study completed the survey. The response rate was ∼36%. The studied population had a mean age of 58.97 ± 11.09 years ranged between 40 and 96 years. Demographic data and common medical conditions associated with the population are summarized in . Subjects of the sampled population were fairly evenly distributed among all age groups. Parameters on smoking and drinking habits, self-perceived obesity, self-reported metabolic syndromes including hypertension (HT), diabetes mellitus (DM) and their comorbidity, and self-reported urological disorders were significantly associated with the age of adult males. HT and DM were shown to be the common metabolic disorders associated with age, clear upward trends were observed for both illnesses affecting 40% and 20% of the sampled population, respectively. The same trend was observed on the comorbidity of HT and DM, whereas those suffering from DM were shown to have higher chance (ranged 75–94%) to develop into comorbidity with HT with age. The prevalence rates of HT, DM and their comorbidity were particular highest in the age group of 70 years or above at 63%, 34% and 32%, respectively. Various urological disorders including benign prostatic hyperplasia (BPH), prostatic cancer and testicular problem were uncommon at age groups under 60 years; however, their prevalence rates were dramatically increased to 11% and 23% at age groups 60–69 years and 70 years or above, respectively. Cancer therapies and hormonal therapies were rare in the sampled population.
Table 1. Demographic data and common illnesses of the adult male population of Hong Kong.
Male adults of Hong Kong were commonly living with little-to-mild levels of AMS ( and ). The severity of AMS was significantly (p < 0.001) increased with age in all domains (). Overall, >80% of the studied population had little to mild levels of AMS with the mean composite score of 29.4 out of 85, whereas only 2% of the adult males were affected by severe level of AMS. The prevalence of moderate-to-severe levels of AMS was proportionally increased in every 10 years age range, from 9.4% in 40–49 years group, 13.7% in 50–59 years group, 21.0% in 60–69 years groups to 31.9% in 70 or above years group (). Hence, the severity levels of AMS were significantly correlated (r = 0.30; p < 0.001) with age, particularly half and 30% of older adults at age 70 years or above were reported to have mild level and moderate-to-severe level of symptoms, respectively (). The prevalence rates of moderate-to-severe levels of all three AMS domains were all highly correlated with age (). Overall, almost 80% of the studied population was suffered from mild-to-moderate levels of somato-vegetative symptoms.
Table 2. AMS findings according to the age groups as obtained from the Hong Kong male population.
Table 3. Distribution of the responses in the Hong Kong traditional Chinese AMS scale.
The severity of somato-vegetative symptoms was increased with age, whereas the percentage of severe symptoms was the lowest as 6.7% at age 40–49 years and the highest as 30.2% at age 70 years or above (). There were more concerns caused by somato-vegetative symptoms with the mean dimension score of 13.8 out of 35 and sexual symptoms with the mean dimension score of 8.4 out of 25, both were within the ranges of moderate severity level. The prevalence rates of moderate-to-severe levels of somato-vegetative symptoms and sexual symptoms were found to be the highest at 76.4% and 70.3%, respectively, at age 70 years or above. The common somato-vegetative complaints reported by the adult males were having declined feeling of general well-being due to joint and muscular pains, decreased in muscular strength as well as physical exhaustion and lacking vitality (). On the other hand, half of the male adults were suffered from moderate-to-severe levels of sexual symptoms. Particularly, the severe symptoms were dramatically increased by 15% from the age group of 40–49 years to any age at above 49 years, while the moderate symptoms were gradually increased with age (). More than half of the respondents reported they felt they have passed their peak, followed by other sexual symptoms, except decrease in beard growth ().
For the psychological domain, ∼20% of the respondents had moderate-to-severe symptoms, of which the prevalence was increased with age (). Among the five items of the psychological subscale, the complaints about feeling burnt out and having hit rock-bottom were dominated (). Dimension scales of all AMS domains were observed to have good correlation (0.77 for sexual; 0.81 for psychological and 0.89 for somato-vegetative) with the AMS composite (total-sum) score.
Aging males’ symptoms were highly inter-correlated with the EQ-5D-3L indexes
The mean self-perceived health state score was found to be 73 out of 100, whereas the score was negatively correlated (r = 0.27; p < 0.001) with age (). Similar significant trends were observed in all five dimensions measured at the three levels using the EQ-5D-3L questionnaire. More than one-fifth of the male adults were affected by moderate level of pain or diskomfort while the frequency was clearly increased with age, and only two respondents who aged >70 years were reported suffering from extreme pain or diskomfort (). There was 5%–11% of the studied population who had encountered some problems with the remaining QoL dimensions, and all shared a similar increasing trend with age (). Furthermore, severity levels, composite score and domain scores obtained with the Hong Kong Traditional Chinese AMS scale were significantly (p < 0.001) different between the “with problems” and “No problems” subpopulations of the five QoL dimensions (). Results of the AMS were inter-correlated with the EQ-5D-3L findings, particularly the self-perceived health state scores reported in the EQ-5D-3L were significantly (p < 0.001) correlated negatively with the composite score and the domain scores of the AMS, as shown in .
Figure 1. Linear regression analysis between the AMS scores and EQ VAS scores.
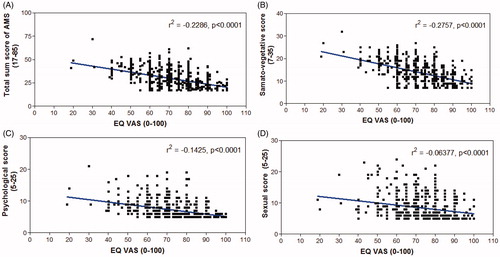
Table 4. Findings of EQ-5D-3L according to the age groups as obtained from the Hong Kong male population.
Table 5. Correlational analysis and comparison of the AMS symptoms between the “with problem” and “no problem” subpopulations identified by the EQ-5D-3L questionnaire.
Discussion
This study revealed that the majority of the Hong Kong adult male population aged 40 years or above was bothered by aging symptoms at little-to-mild levels, while their somato-vegetative and sexual symptoms were at mild-to-moderate levels. The severity of AMS and all subscale symptoms were highly correlated with age. For older males at age 70 years or above, majority was suffered from moderate-to-severe levels of somato-vegetative and sexual symptoms while mild-to-moderate level of psychological symptoms, which were more severe than all other age groups. Results herein also indicated the Hong Kong Traditional Chinese AMS scale has acceptable reliability, in terms of test–retest reliability and Cronbach’s alpha international consistency. Outcomes measured by the Hong Kong Traditional Chinese AMS scale were highly correlated with those measured by EQ-5D-3L questionnaire. Therefore, the Hong Kong Traditional Chinese AMS scale is a reliable instrument being used for measuring the severity of aging symptoms and their impacts on HRQoL, in adult males of Hong Kong.
Different versions of AMS scale have been compared with several generic quality of life (QoL) and HRQoL questionnaires such as SF12 (physical and menatal health components), SF36, Rapid Disability Rating Scale (RDRS), and Hospital Anxiety and Depression Scale (HADS) [Citation6,9–11]. However, to our best knowledge, it was the first-time that an AMS scale version was used in parallel with EQ-5D-3L and revealed the high inter-correlation. Similar to other countries [Citation9], the correlations between the domain scores and composite score were high (ranged 0.77–0.89) but lower among the subscales (ranged 0.44–0.66), which suggested that the subscales are not fully independent. Furthermore, the coefficients for test–retest coefficients and Cronbach’s alpha internal consistency obtained with the Hong Kong Traditional Chinese AMS scale were comparable to the values obtained in most countries in Asia [Citation9]. When compared with the worldwide values, the test–retest coefficients were shown to be intermediate between the countries with the highest and lowest values, e.g. the lowest 0.74 at Portugal and highest at Korea 0.90 for the composite score [Citation9]. Portugal and Spain have reported the lowest test–retest coefficients for all subscale scores among all countries, while the highest coefficients were independently reported by Korea for psychological score (0.85), Sweden for somatic score (0.94) and Italy for sexual score (0.98) [Citation9].
According to the results of the International web survey using the AMS scale, the severity of AMS in Hong Kong was less severe than the US and UK populations [Citation3]. The total AMS score and subscale scores obtained with the Hong Kong adult males were almost the same as reported with the Japanese males aged 40 years or above [Citation12]. However, the AMS situation of Hong Kong was different from what was reported in China, where the total AMS severity was reported to be at little-to-mild level among all age groups >40 years, the moderate-to-severe level was steadily ranged at 24–34% at all ages with the highest prevalence between 50 and 69 years and was only reported as 25% even for those aged 70 years or above, which was much lower than the 32% reported in this study [Citation8]. The aging populations and their health impacts are varied due to multiple cultural and economic factors in different geographical locations [Citation13]. This may explain at least partially why the two Chinese populations (i.e. Hong Kong and China) displayed very different AMS morbidities. In fact, the Hong Kong population has a similar living style to the Japanese population that both have high living standards than the population of a small city of China where the above study was conducted [Citation8]. More in-depth investigation of those factors is required.
As shown in the results, the adult males of Hong Kong were bothered by the somatic and sexual symptoms. Particularly, as agreed between the AMS scale and EQ-5D-3L questionnaire, older males of Hong Kong were demonstrated to have more problems with the musculoskeletal strength and pain. It is assumed that androgen production is progressively declined with age in males. Studies have associated the age-related changes in bone health and muscle strength with hypodonadism that affects the musculosckeletal function [Citation11,Citation14,Citation15]. Furthermore, numerous reports [Citation16–21] have demonstrated the association between testosterone levels and metabolic syndromes, which seemed to be consistent with the high prevalence of HT, DM and their comorbidity reported in the adult males. However, excessive sweating – one of the remarkable sign of AMS symptoms was lacking in the studied population, as only reported by 26% at mild to severe levels, and the most majority (21% of the 26%) was at mild level only. The frequencies of various types of sweating in males are similar to those happened in females during the course of aging, due to the hormonal changes specifically androgen in males. In fact, the associations between AMS and androgen levels were often reported in males with certain health conditions, e.g. adverse mental symptoms [Citation4]. The AMS total and domain scores were not correlated with androgen levels in 161 ambulatory elderly men aged 74–89 years [Citation10]. In fact, the AMS scale is known to be primarily an health-related quality of life scale (also supported by the current findings on good correlation with EQ-5D-3L)), but may not be the best tool for diagnostic purpose. The International Society for the Study of the Aging Male (ISSAM) has recently recommended the most up-to-date diagnostic method for AMS [Citation22].
In conclusion, the population of Hong Kong male adults was living with little to mild levels of aging symptoms. The severity of aging symptoms was correlated with age, especially for the somato-vegetative and sexual symptoms. Such symptoms were also seemed to be associated with metabolic syndromes particularly hypertension and diabetes mellitus that commonly associated with age. The Hong Kong traditional Chinese AMS scale was shown to have high reliability in terms of both test–retest and Cronbach’s alpha internal consistency analyzes. The scale was also found to have good correlation with the EQ-5D-3L questionnaire that used for measuring the health-related quality of life.
Acknowledgements
The authors would like to thank the two independent translators and the nine data collectors who have volunteered to help in this study. Special thanks to Ms Sara Fung who had proof read the article, and Mr Jacky Tam who had coordinated the data collection schedule with the data collectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Heinemann LAJ, Zimmermann T, Vermeulen A, et al. A new ‘Aging male’s symptoms’ rating scale. Aging Male 1999;2:105–14
- Reyes JA III, Tan DA, Quimpo JA, et al. The Philippine male aging survey. Aging Male 2004;7:227–35
- Trinick TR, Feneley MR, Welford H, Carruthers M. International web survey shows high prevalence of symptomatic testosterone deficiency in men. Aging Male 2011;14:10–15
- Hintikka J, Niskanen L, Koivumaa-Honkanen H, et al. Hypogonadism, decreased sexual desire, and long-term depression in middle-aged men. J Sex Med 2009;6:2049–57
- Yoshida N, Kumano H, Kuboki T. Does the Aging Males’ Symptoms scale assess major depressive disorder? A pilot study. Maturitas 2006;53:171–5
- Lee CP, Jiang JR, Chen Y, et al. The Aging Males’ Symptoms (AMS) Scale assesses depression and anxiety. Aging Male 2013;16:97–101
- Chen CY, Wang WS, Liu CY, Lee SH. Reliability and validation of a Chinese version of the Aging Males’ Symptoms scale. Psychol Rep 2007;101:27–38
- Kong XB, Guan HT, Li HG, et al. The ageing males’ symptoms scale for Chinese men: reliability, validation and applicability of the Chinese version. Andrology 2014;2:856–61
- Daig I, Heinemann LA, Kim S, et al. The Aging Males’ Symptoms (AMS) scale: review of its methodological characteristics. Health Qual Life Outcomes 2003;1:77
- T’Sjoen G, Goemaere S, De MM, Kaufman JM. Perception of males’ aging symptoms, health and well-being in elderly community-dwelling men is not related to circulating androgen levels. Psychoneuroendocrinology 2004;29:201–14
- Hall SA, Chiu GR, Williams RE, et al. Physical function and health-related quality-of-life in a population-based sample. Aging Male 2011;14:119–26
- Kobayashi K, Hashimoto K, Kato R, et al. The aging males’ symptoms scale for Japanese men: reliability and applicability of the Japanese version. Int J Impot Res 2008;20:544–8
- Goh VH. Aging in Asia: a cultural, socio-economical and historical perspective. Aging Male 2005;8:90–6
- Chin KY, Soelaiman IN, Naina M,I, et al. Testosterone is associated with age-related changes in bone health status, muscle strength and body composition in men. Aging Male 2012;15:240–5
- Nolan M, Nitz J, Choy NL, Illing S. Age-related changes in musculoskeletal function, balance and mobility measures in men aged 30-80 years. Aging Male 2010;13:194–201
- Mazza AD, Morley JE. Metabolic syndrome and the older male population. Aging Male 2007;10:3–8
- Schipf S, Haring R, Friedrich N, et al. Low total testosterone is associated with increased risk of incident type 2 diabetes mellitus in men: results from the Study of Health in Pomerania (SHIP). Aging Male 2011;14:168–75
- Liao CH, Huang CY, Li HY, et al. Testosterone and sex hormone-binding globulin have significant association with metabolic syndrome in Taiwanese men. Aging Male 2012;15:1–6
- Mazur A, Westerman R, Werdecker A, Mueller U. Testosterone and type 2 diabetes in men. Aging Male 2014;17:18–24
- Cao J, Li J, Hao W, et al. Correlation of sex hormone and androgen receptor with diabetes mellitus in elderly men. Aging Male 2011;14:162–7
- Torkler S, Wallaschofski H, Baumeister SE, et al. Inverse association between total testosterone concentrations, incident hypertension and blood pressure. Aging Male 2011;14:176–82
- Lunenfeld B, Mskhalaya G, Zitzmann M, et al. Recommendations on the diagnosis, treatment and monitoring of hypogonadism in men. Aging Male 2015;18:5–15