Abstract
Background: Disease management programmes (DMPs) improve quality of care for patients with heart failure (HF). However, only a limited number of trials have studied the efficacy of such programmes for patients with heart failure with preserved ejection fraction (HFPEF). Objective: To estimate the impact of a structured, nurse-led patient education programme and care plan in general practice on outcome parameters and events in patients with HFPEF. Methods: Single blinded randomized clinical trial with an intervention over six months and a follow-up during 12 additional months. In the control group, the patients (n = 41) were managed according to Russian national guidelines. Patients in the intervention group (n = 44) received education on individual lifestyle changes and modifications of cardiovascular disease (CVD) risk factors, home-based exercise training and weekly nurse consultations in addition to usual care. Results: Six months after their inclusion, patients in the intervention group significantly improved body mass index, waist circumference, six-min walk test distance, total cholesterol, low-density lipoprotein, left ventricular end-diastolic volume index, quality of life and level of anxiety. After 18 months, there were 11 deaths (25%) or hospitalizations in the intervention group and 12 (29%) in the control group (P = 0.134). Cardiovascular mortality and readmission rate were not reduced significantly after six months of follow-up: the hazard ratio was 0.47 (95% CI: 0.17–1.28; P = 0.197). After 18 months, this was 0.85 (0.42–1.73; P = 0.658).
Conclusion: This primary care based DMP for patients with HFPEF improved the patients’ emotional status and quality of life, positively influenced body weight, functional capacity and lipid profile, and attenuated heart remodelling.
Introduction
According to the ‘EPOCH–A–CHF’ epidemiological study, 5.5% of the population in Russia, or about eight million people, suffer from chronic heart failure (CHF) (Citation1). Despite major advances in the treatment of CHF, mortality and morbidity remain unacceptably high (Citation2). One of the suggested approaches to patient care is the implementation of disease management programmes (DMPs), which are designed to improve the effectiveness and efficiency of care and can be defined as a class of interventions to improve the management of vulnerable patients with a chronic condition (Citation3). A systematic evaluation of the efficacy of DMPs for patients with CHF showed a decrease of 30% in readmission for decompensated heart failure (HF) or other cardiovascular causes. This was associated with a decrease in cost of care and a trend towards a lower mortality rate. Most trials were conducted with specially trained nurses (Citation4). The Russian SHANS multi-centre trial found a decrease of 20.5% in re-admission for decompensated HF in the intervention group compared with patients in the control group and a decrease in cardiovascular mortality from 13% to 8.3% in the intervention group (Citation5). In this study, the patient education was organized during the course of hospitalization.
However, most patients with CHF are managed in primary care. These patients are mainly elderly women with a history of arterial hypertension and diabetes (Citation6) and a diagnosis of HF with preserved ejection fraction (HFPEF) (Citation7). In the EPOCH–A–CHF study, 57% of patients with clinical signs of CHF had preserved left ventricular ejection fraction (LVEF > 50%). HFPEF has a poor prognosis comparable with that of HF with reduced ejection fraction with five-year mortality rates of almost 60% (Citation8). Moreover, in the last 15 years, survival has improved for patients with HF with reduced ejection fraction but not for patients with preserved ejection fraction (Citation9). Over the last two decades, some 50 variables have been shown to be predictors of mortality in patients with CHF (Citation10). Most of the predictors of death in patients with HFPEF are similar to those for patients with reduced ejection fraction (Citation8). However, limited data are available on how DMPs influence the prognosis of patients suffering from HFPEF.
Therefore, we designed and organized a randomized clinical trial in primary care to evaluate the impact of a structured nurse-led patient education programme and care plan on the prognosis, quality of life and cardiac function of patients with HFPEF.
Methods
Study design
The study was a randomized clinical trial with a single blinded intervention over six months comparing the efficacy of a structured nurse-led patient education programme and care plan with usual care, monitoring heart failure patients in the context of a primary care practice (). The local ethics committee of St Petersburg Medical Academy of Postgraduate Study approved the study.
Figure 1. Enrollment of patients in the study.
(Date decision letter: 11/5/2007). The study started 1/9/2006 and the end of the follow-up period was 30/8/2009.
Sample size estimation
Other researchers reported previously that the overall mortality and readmission rates for HFPEF were nearly 60% during 6 months (Citation11), and the average effect of DMPs concerning re-admission rate was nearly 50% (Citation2). Therefore, we projected that our intervention would decrease the combined number of deaths and hospitalizations for a CV event from 60% to 30%. A sample size of 78 persons (39 in each group) was calculated to be able to detect a 50% difference between groups in the combined endpoints with 80% power and a 5% significance level. Based on experience of other researchers, we expected a 70% response rate (Citation12). Therefore, we decided to recruit 50 patients in each group.
Selection of study participants
The study was conducted in the office of General Practice of the Municipal Medical Centre of Vyborg (St Petersburg region). The centre has 13 000 patients (adults and children) on its list. The medical staff includes 8 general practitioners (GPs), 2 doctor's assistants (nurse practitioners) and 8 nurses.
Before the start of the intervention (the inclusion period was six months), GPs selected patients during outpatient reception hours. Included were all patients of 50 years or older with an established diagnosis of HFPEF in a stable condition (see ). GPs diagnosed HFPEF based on symptoms (dyspnoea at rest or during exercise, fatigue, tiredness, ankle swelling) or signs (tachycardia, tachypnea, raised jugular venous pressure, oedema) of congestive HF plus the results of an echocardiographic examination by a cardiologist: presence of a normal LV systolic function (LVEF 50%), and evidence of abnormal LV relaxation, diastolic distensibility or diastolic stiffness (Citation13). Exclusion criteria were: a history of an acute coronary syndrome within the last 6 months, a haemodynamically significant valvular stenosis (Citation14), the presence of physical conditions that limited participation in a rehabilitation programme, insulin-dependent diabetes mellitus or confirmed chronic obstructive pulmonary disease i.e. an FEV1/FVC <70, a negative reversibility test and a history of chronic cough, sputum production and dyspnoea.
Box 1. Criteria used to define a stable condition of HFPEF.
Randomization and informed consent
Every eligible patient was included in our study. All eligible patients signed an informed consent form. Selected patients were stratified by sex and randomized with the ‘randomization by envelopes’ method into two equal groups: a control group (usual care group) and an intervention group (usual care + nursing intervention group). An external collaborator that did not know the patients performed this procedure. After randomization but before the start of the intervention, 6 patients in the intervention group and nine in the control group refused to continue (see ).
Usual care
The usual care treatment and monitoring was organized in concordance with the Russian national guidelines (Citation15). Usual care included the prescription of medication as well as non-pharmacological measures. The basic medications are angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), b-blockers, aldosterone antagonists, diuretics and digoxin if needed. Non-pharmacological measures included recommendations concerning diet, alcohol intake, weight reduction, smoking cessation, activity and exercise training, given by the GP during consultation. The frequency of visits to the GP depended on the patient's feelings and the presence of complaints and special needs.
Intervention
The nursing intervention programme consisted of three parts. The first was an educational programme consisting of four weekly educational group sessions, targeting individual lifestyle changes and modifications of cardiovascular risk factors (month one). Each session lasted about 90 min and included a lecture and a practical skills session. The main topics of the sessions were disease information, lifestyle changes and information on treatment. In each group, 5 or 6 people participated. The teachers were nurses with a special degree in patient education obtained in a joint course.
The second part of the intervention was exercise training (see ). In the first month, the patients attended four weekly introductory sessions of 30 min each, under the supervision of a physiotherapist who had been trained in the study protocol. The personal intensity level, frequency and duration of training were determined and an individualized programme was recommended for further practice at home during the next five months (months two-to-six).
Box 2. Short overview of the exercise-training programme.
The third part was proactive and supportive nursing care. This care included weekly 15–30 min consultations in the health centre or by phone over five months (months two-to-six). During the consultations, the nurse discussed successes and difficulties encountered by the patient in making lifestyle changes, checked medication compliance and elicited information about any changes in the condition of the patient. The specially trained nurses, who were teachers in the educational programme, did the consultations. All observations were registered on a form in the medical record.
Outcome parameters
Variables. The subjects were tested at baseline (T0, before randomization) and after six months (T6) by nurses and physicians, who did not know whether the patient belonged to the intervention or the control group (single blinded). Outcome parameters were New York Heart Association (NYHA) Class of CHF, body mass index (BMI), waist circumference (WC), 6-min walking test (6MWT) and biochemical parameters of blood plasma levels of fasting blood glucose, total cholesterol, low-density lipoprotein (LDL), C-reactive protein (CRP, high sensitivity method) and N-terminal pro-brain natriuretic peptide (NT-proBNP) (Biomedica Gruppe Austria). We measured emotional status with the hospital anxiety and depression scale (HADS) (Citation16) and quality of life with the Minnesota living with heart failure questionnaire (MLHFQ) (Citation17). The following echocardiographic parameters were evaluated for cardiac function assessment: left atrial size index (LASI), LV end-diastolic volume index (LVEDVI), LV mass index (LVMI) and ratio of early (E) to late (A) mitral valve flow velocity (E/A ratio).
Change. To study the evolution of individual patients, the change in the outcome parameters between T0 and T6 was determined. For continuous variables, the Edwards–Nunally index was used to determine a relevant improvement or decline. This index calculates the significance of individual changes based on the reliability of the measuring instrument, the confidence interval and the population mean (Citation18). For the other variables (NYHA class, BMI, WC, 6MWT and the biochemical and echocardiographic parameters), a positive or negative change was defined in relation to the criteria described in (supplementary material).
Table I. Criteria for changes in the outcome parameters of a physical state.
Since a cut-off value of >7 points on the HADS identifies anxiety or depression, the change in emotional status was estimated as positive if the level of anxiety or depression decreased to 7 points on the HADS, and as negative if the level of anxiety or depression increased to >7 points on the HADS (Citation16).
Events. The number of deaths and hospitalizations for a cardiovascular event (after six (T6) and 18 months (T18) after the start of the intervention, respectively) were used as a combined endpoint. At the end of the follow-up period, a retrospective analysis of the medical analysis of the medical records was carried out to collect all events by the principal investigator.
Statistical analysis
We used STATISTICA 5.5 (StatSoft Inc 1999) for all calculations. Nonparametric methods were used for variables with a non-normal distribution. Data were described using median values and inter quartile ranges (IQR) and groups were compared using the Mann–Whitney U test or the Chi-square test (method of maximum likelihood or Yates corrected if any observed frequency was <10). The numbers of events in the intervention group compared with the control group were expressed as hazard ratios. A two-sided P-value of <0.05 was considered as statistically significant.
Results
Baseline characteristics (n = 85)
At baseline, 85 study participants (26 men, 59 women) with a mean age of 67 years (range: 59–71) were included and evaluated. Overall, 17% of patients were in NYHA class I, 35% in NYHA class II and 48% in NYHA class III. demonstrates that before inclusion in the study, no significant differences were observed between the control and intervention groups in age, sex, NYHA class or number of prescribed medications. In addition, there were no significant differences regarding the outcome parameters between both groups, only the LVMI was significantly higher in the intervention group.
Table II. Comparison of the control and intervention groups by age, sex, severity of disease and treatment protocol before start of the interventiona.
Physical and psychosocial parameters at six months (n = 75)
shows the quantitative indices of the outcome parameters in both study groups before the start of the intervention and after six months. After six months, 75 patients were tested, because 1 had died in the intervention group and 2 had died in the control group; 3 patients in the intervention group and 4 in the control group refused to continue the study. The reasons for refusing were change in location of residence, work pressure and shortage of time. shows the difference between the control group and the intervention group in the number of patients with positive and negative changes of the outcome parameters. A greater number of patients in the intervention group than in the control group improved on outcome parameters of physical state such as BMI, WC, 6MWT, total cholesterol, LDL, LVEDVI and on scores in the MLHFQ and the HADS.
Table III. Physical and psychosocial outcome parameters in both study groups before the start of the intervention and after 6 months (median, IQR).
Table IV. Number of patients in the control and intervention groups with positive and negative changes in physical and psychosocial outcome parameters, 6 months after inclusion.
Events: mortality and hospitalization at six and 18 months (n = 85)
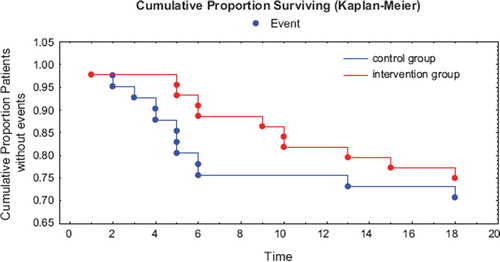
The total number of events in the intervention group (n = 44) after six months were 5: 1 patient died and 4 patients were hospitalized for a cardiovascular event. In the control group (n = 41), 2 patients died and 8 patients were hospitalized (total number of events: 10). After 18 months, 1 more patient had died in the intervention group. 5 more and 2 more patients respectively were hospitalized in the intervention and control groups. In summary, after six months 11% (5/44) reached the combined endpoint in the intervention group and 24% (10/41) in the control group. After 18 months the figures were 25% (11/44) and 29% (12/41), respectively. However, the intervention did not reduce the risk of cardiovascular events after six and 18 months significantly: the hazard ratios were 0.47 (95% CI: 0.17–1.28; P = 0.197) and 0.85 (0.42–1.73; P = 0.658), respectively. shows the cumulative proportions of patients without combined events over the 18 months observation period.
Figure 2. Survival analysis of patients in the intervention (n = 44) and control (I = 41) group: Kaplan–Meier curves for combined events (mortality and hospitalization) (P = 0.281, Cox's F-Test). Time is expressed in months.
Discussion
Main findings
This six-month intervention trial in a Russian general practice showed a positive effect on multiple outcome parameters for a structured nurse-led patient education programme and care plan in patients with HFPEF. We observed positive effects on BMI and WC, the 6MWT, levels of total cholesterol and LDL fraction, LVEDVI, emotional state and quality of life. However, no significant difference was observed between groups in the number of combined cardiovascular events, i.e. mortality and hospital admissions.
Other studies
Most previous trials studied the efficacy of a DMP for patients with CHF and reduced ejection fraction. Trials that study the impact of a DMP for HFPEF patients are scarce. We found two trials addressing this problem. One trial studied the effect of a home-based exercise programme in addition to patient education on quality of life and functional capacity in 32 women with HFPEF (Citation19). The intervention group significantly improved in quality of life and depression scores and functional capacity estimated by the 6MWT. However, this study included only women.
Another trial studied the effect of a DMP on all-cause mortality, functional class of HF, quality of life and total health care costs in a subgroup of 317 HFPEF patients (Citation12,Citation20). Nurses provided a DMP for 18 months. This trial found no effects on mortality, functional class and health care costs, but a positive effect on quality of life estimated by the SF-36 questionnaire at six and 12 months. Our results are in line with the results of these studies.
Strengths and limitations
Unlike previous trials, our study population was representative in age and sex for a population of patients with HFPEF as described in epidemiological studies (Citation1,Citation21). Moreover, our study is unique in the intensity and individualized approach of the care programme: nurses contacted patients weekly for six months and the exercise training level was individually adjusted. It is well known that a more intensive follow-up results in a greater long-term benefit (Citation22). Furthermore, our study estimated the effect of a DMP on a broad spectrum of outcome parameters in patients with HFPEF.
There are several limitations of the present study. First, only 85 patients were included. However, specific inclusion and exclusion criteria were used and our sample proved to be a representative selection of patients with HFPEF. Second, the intervention period was only six months. Therefore, we cannot answer the question whether and how intensively the intervention should be continued. Third, we did not investigate compliance with treatment, although this could be an important exsplanation of our study results.
Implications
To date, no specific treatment has been convincingly shown to reduce morbidity and mortality in patients with HFPEF. Guidelines recommend that management of HFPEF should be aimed at the causes of diastolic dysfunction such as myocardial infarction, hypertension and diabetes and precipitating factors like atrial fibrillation (Citation22). In this study, patients were treated in accordance with the Russian national guidelines (Citation15). All patients received an angiotensin-converting enzyme inhibitor and 64% received a -blocker. The observed positive effect of our intervention may be explained by the improvement in patient compliance. Previous research has shown that a nurse-led intervention with emphasis on education and counselling during hospitalization, at home and by telephone was effective in the improvement of medication compliance and patient self-control (Citation24). In addition, evidence exists that exercise training improves functional capacity and health-related quality of life and induces favourable heart remodelling (Citation19,Citation25).
However, our intervention did not demonstrate additional benefits on the combined endpoint. There was only a trend towards decreasing numbers of events in the intervention group during nursing activities. It has been reported that a longer follow-up may enhance the effects of patient education and support (Citation22).
A nurse-led patient education programme and tailoring of an individualized care plan for each patient seemed to be effective and could be recommended for patients with HFPEF in general practice. Education of the patient and his/her family is an important component of managing HFPEF. Nurses find themselves in a unique position and can take shared responsibility with the GP for patient education, support provision and improvement in quality of life. However, more randomized clinical trials are needed to substantiate the limited existing evidence.
Conclusion
A structured nurse-led education programme and care plan, including exercise and frequent consultations, for patients with HFPEF organized in a primary care setting improved the patients’ emotional status and quality of life, had a positive influence on body weight, functional capacity and lipid profile, and attenuated heart remodelling.
Funding
This research was run without any external funding.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Mareev VIu, Danielyan MO, Belenkov IuN. Comparative characteristics of patients with CHF in relation to the value of injection fraction by data from the Russian multicenter study EPOCH-A-CHF: Once more about the problem of CHF with preserved left ventricular systolic function. J Heart Fail. 2006;4:164–71.
- Gustafsson F, Malcolm J, Arnold O. Heart failure clinics and outpatient management: review of the evidence and call for quality assurance. Eur Heart J. 2004;25:1596–604.
- Rumsfeld JS, Masoudi FA. Heart failure disease management works, but will it succeed? Eur Heart J. 2004;25:1565–7.
- Gonseth J, Guallar-Castillon P, Banegas JR, Rodriguez-Artalejo F. The effectiveness of disease management programmes in reducing hospital re-admission in older patients with heart failure: A systematic review and meta-analysis of published reports. Eur Heart J. 2004;25:1570–95.
- Ageev FT, Mareev VIu, Seredenina EM, Belenkov IuN. Prospects of introduction of specialised forms of active outpatient conducting patients with heart failure: A structure, a technique and preliminary results of the Russian program ‘SHANS.’ J Heart Fail. 2004;5:268–71.
- Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart 2007;93:1137–46.
- Aurigemma GP, Gaasch WH. Diastolic heart failure. N Engl J Med. 2004;351:1097–105.
- Tribouilloy Ch, Rusinaru D, Mahjoub H, Soulière V, Lévy F, Peltier M, . Prognosis of heart failure with preserved ejection fraction: A five-year prospective population-based study. Eur Heart J. 2008;29:339–47.
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006; 355:251–9.
- Eichhorn EJ. Prognosis determination in heart failure. Am J Med. 2001;110(Suppl. 7A):14S–36S.
- Smith GL, Masoudi FA, Vaccarino V, Radford MJ, Krumholz HM. Outcomes in heart failure patients with preserved ejection fraction: Mortality, readmission, and functional decline. Am Coll Cardiol. 2003;41:1510–8.
- Smith B, Forkner E, Zaslow B, Krasuski RA, Stajduhar K, Kwan M, . Disease management produces limited quality of life improvements in patients with congestive heart failure: Evidence from a randomized trial in community-dwelling patients. Am J Manag Care 2005;11:701–13.
- Guidelinesfor the diagnosis and treatment of chronic heart failure: Executive summary (update 2005). The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26: 1115–40.
- Bonow RO, Carabello B, de Leon AC Jr, Edmunds LH Jr, Fedderly BJ, Freed MD, . Guidelines for the management of patients with valvular heart disease: Executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients with Valvular Heart Disease). Circulation 1998;98:1949–84.
- National Recommendations of Russian Academic Society of Cardiology and the Society of Specialists in Heart Failure regarding diagnosis and treatment of congestive HF— Second Review. J Heart Fail. 2006;8:1–35.
- Kubzansky LD, Kawachi I, Weiss ST, Sparrow D. Anxiety and coronary heart disease: A synthesis of epidemiological, psychological, and experimental evidence. Ann Behav Med. 1998;20:47–58.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–70.
- Riegel B, Moser DK, Glaser D, Carlson B, Deaton C, Armola R, . The Minnesota living with heart failure questionnaire: Sensitivity to differences and responsiveness to intervention intensity in a clinical population. Nursing Res. 2002;51:209–18.
- Speer DC, Greenbaum PE. Five methods for computing significant individual client change and improvement rates: Support for an individual growth curve approach. J Consult Clin Psychol. 1995;63:1044–8.
- Gary RA, Sueta CA, Dougherty M, Rosenberg B, Cheek D, Preisser J, . Home-based exercise improves functional performance and quality of life in women with diastolic heart failure. Heart Lung 2004;33:210–8.
- Galbreath AD, Krasuski RA, Smith B, Stajduhar K, Kwan M, Ellis R, . Long-term healthcare and cost outcomes of disease management in a large, randomized, community-based population with heart failure. Circulation 2004;110: 3518–26.
- Bruggink-Andre de la Porte PWF, Lok DJA, van Veldhuisen DJ, van Wijngaarden J, Cornel JH, Zuithoff NPA, . Added value of a physician-and-nurse-directed heart failure clinic: Results from the Deventer-Alkmaar heart failure study. Heart 2007;93:819–25.
- Lenzen MJ, Scholte op Reimer WJ, Boersma E, Vantrimpont PJ, Follath F, Swedberg K, . Differences between patients with a preserved and a depressed left ventricular function: A report from the EuroHeart Failure Survey. Eur Heart J. 2004;25:1214–20.
- Wal van der MH, Jaarsma T, van Veldhuisen DJ. Non-compliance in patients with heart failure; how can we manage it? Eur J Heart Fail. 2005;7:5–17.
- Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, Komajda M, . Guidelines for the diagnosis and treatment of chronic heart failure: executive summary: The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26: 1115–30.
- Giallauria F, Cirillo P, Lucci R, Pacileo M, De Lorenzo A, D'Agostino M, . Left ventricular remodelling in patients with moderate systolic dysfunction after myocardial infarction: Favourable effects of exercise training and predictive role of N-terminal pro-brain natriuretic peptide. Eur J Cardiovasc Prev Rehabil. 2008;15:113–8.
- Reisfield GM, Wilson GR. Prognostication in heart failure. J Palliat Med. 2007;10:245–6.
- Graham I, Atar D, Borch-Johnsen K, Boysen G, Burrel G, Ciffkova R . European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur Heart J. 2007;28:2375–414.
- Crapo RO, Casaburi R, Coates AL, Enright PL, MacIntyre NR, McKay RT, . ATS Statement: Guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002; 166:1111–7.
- Pearson TA, Mensah GA, Wayne AR, Anderson JL, Cannon RO, Criqui M, . Markers of inflammation and cardiovascular disease: Application to clinical and public health practice. A statement for healthcare professionals from the Centers for Disease Control and Prevention and American Heart Association. Circulation 2003;107:499–511.
- Bruch C, Fischer C, Sindermann J, Stypmann J, Breithardt G, Gradaus R. Comparison of the prognostic usefulness of N-terminal pro-brain natriuretic peptide in patients with heart failure with versus without chronic kidney disease. Am J Cardiol. 2008;102:469–74.
- Vazquez R, Bayes-Genis A, Cygankiewicz I, Pascual-Figal D, Grigorian-Shamagian L, Pavon R, . The MUSIC Risk score: A simple method for predicting mortality in ambulatory patients with chronic heart failure. Eur Heart J. 2009;30: 1088–96.
- Grayburn PA, Appleton CP, DeMaria AN, Greenberg B, Lowes B, Oh J, . Echocardiographic predictors of morbidity and mortality in patients with advanced heart failure: The Beta-blocker Evaluation of Survival Trial (BEST). J Am Coll Cardiol. 2005;45:1064–71.
- Khouri SJ, Maly GT, Suh DD, Walsh TE. A practical approach to the echocardiographic evaluation of diastolic function. J Am Soc Echocardiogr. 2004;17:290–7.