Abstract
This is the first article in a Series on collaborative projects between European countries, relevant for general practice/family medicine and primary healthcare.
Telemedicine, in particular the use of the Internet, videoconferencing and handheld devices such as smartphones, holds the potential for further strides in the application of technology for the delivery of healthcare, particularly to communities in rural and remote areas within and without the European Union where this study is taking place. The Northern Periphery Programme has funded the ‘Implementing Transnational Telemedicine Solutions’ (ITTS) project from September 2011 to December 2013, led by the Centre for Rural Health in Inverness, Scotland. Ten sustainable projects based on videoconsultation (speech therapy, renal services, emergency psychiatry, diabetes), mobile patient self-management (physical activity, diabetes, inflammatory bowel disease) and home-based health services (medical and social care emergencies, rehabilitation, multi-morbidity) are being implemented by the six partner countries: Scotland, Finland, Ireland, Northern Ireland, Norway and Sweden. In addition, an International Telemedicine Advisory Service, created for the project, provides business expertise and advice. Community panels contribute feedback on the design and implementation of services and ensure ‘user friendliness’. The project goals are to improve accessibility of healthcare in rural and remote communities, reducing unnecessary hospital visits and travel in a sustainable way. Opportunities will be provided for comparative research studies. This article provides an introduction to the ITTS project and how it aims to fulfil these needs. The ITTS team encourage all healthcare providers to at least explore possible technological solutions within their own context.
KEY MESSAGE
The goal of the ITTS team is sustainable leading edge eHealth delivery via new technologies.
Telemedicine has immense potential in improving healthcare delivery for communities everywhere in a cost-effective way.
We encourage all healthcare providers to at least explore possible technological solutions within their own context.
INTRODUCTION
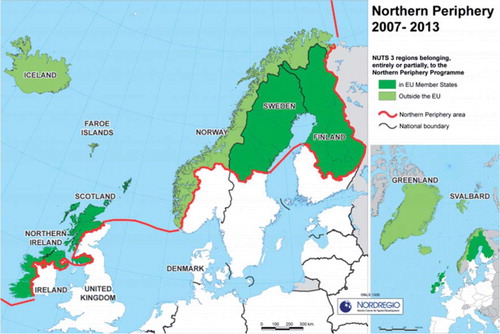
The countries included in the Northern Periphery Programme (NPP)—Greenland, Iceland, Faroe Islands, Ireland, Northern Ireland, Scotland, Norway, Sweden, and Finland—are distinctive; however, they have common features of dispersed populations living in remote areas subject to harsh weather conditions (see )(Citation1). The current project, ‘Implementing Transnational Telemedicine Solutions’ (ITTS) aims to implement transnational telemedicine solutions, at scale, and in a sustainable manner, into everyday medical practice across the Northern Periphery. It is based on the previous Competitive Health project funded by the European Union. Box 1 provides a summary of the partner countries (Ireland, Northern Ireland, Scotland, Norway, Sweden, Finland) and team members. In addition, Greenland and the Faroe Islands are acting as observer countries with a view to future involvement in telemedicine projects.
Figure 1. Northern periphery programme area and partner countries.
Box 1. The ITTS project: partner countries and team members.
ITTS—Implementing Transnational Telemedicine Solutions
International collaboration between six Northern Periphery countries to provide sustainable health care to rural areas and homes through the use of the Internet, smartphones and videoconferencing units. The budget of €2.3 million is partially funded by the European Union Northern Periphery Programme for 10 demonstrator projects to be implemented between Sept. 2011 and Dec. 2013.
Scotland (Lead): aDavid Heaney, Lee Dowie, Gillian Galloway, Emma Coats, Emily Duncan, Gerry King, Leila Eadie. Centre for Rural Health, University of Aberdeen (http://www.abdn.ac.uk/crh/).
Finland: aMatti Matero, Ritva Leinonen, Tiina Vuononvirta, Teemu Strengell. Oulu Arc Subregion (http://www.oulunkaari.com).
Ireland: aLiam Glynn, Gearóid ÓLaighin, Andrew Murphy, Monica Casey, Patrick Hayes, Breda Kelleher. National University of Ireland, Galway (http://www.nuigalway.ie/general_practice/).
Northern Ireland: aEddie Ritson, Soo Hun, Penny Hobson, Roy Harper. Centre for Connected Health & Social Care (http://www.eu-cch.org).
Norway: aSiri Bjørvig, Undine Knarvik, Line Linstad, Frank Larsen, Stig Karoliussen, Randi Laukli, Heidi Åsheim-Olsen. Norwegian Centre for Integrated Care and Telemedicine (NST) (http://www.telemed.no/).
Sweden: aKate Alrutz, Brith Granstrőm, Anders Asplund, Simon Lindgren, Nils Sandberg. County Council of Västerbotten (http://www.vll.se).
International Telemedicine Advisory Service (ITAS): Frances Mair (Scotland), Seppo Heikkila (Finland), Paddy Gillespie (Ireland), Michael McCormick (Northern Ireland), Trine Bergmo (Norway), Thomas Molen (Sweden).
aPartner country leads.
The ITTS project is based around three themes:
videoconferencing consultations using various forms of readily available technology, saving on unnecessary travel and providing care to remote areas not receiving comparable care to urban areas;
smartphone and internet-based mobile self- management for a range of health issues, which due to the penetration of these technologies is an inexpensive method to implement this service to large numbers of people familiar with these communication methods; and
home-based health services to provide care for patients with multiple and complex health and social care issues who are restricted in their ability to travel.
Previous international experience yielded valuable information and techniques to find innovative healthcare solutions for these remote areas of the northern periphery. International collaboration allows this information to be gleaned through knowledge exchange and increases the potential of discovering solutions, which will be applicable across the peripheral countries. The ITTS project shares knowledge, experience and expertise by exporting projects from countries that have successfully implemented them to countries that will import and use the applications for the first time. shows a map for one of the projects, illustrating these interactions.
Figure 2. Example of one ITTS project.

Sustainability is improved by the group working together in a consistent international approach to establish workable projects with associated business plans and then design training materials to disseminate. In order for clinicians to be enthusiastic about the implementation of telemedicine, they must have a clear understanding of the processes involved, access to transnational best practice and thorough training information, as well as patient information in an easily understood format.
Through normalization of the use of technology into everyday health service delivery practice, the project goals are to improve accessibility of healthcare in rural and remote communities, reducing unnecessary hospital visits and travel in a sustainable way. Opportunities will be provided for comparative research studies to demonstrate the cost-effectiveness of this form of health delivery: providing a return on the investment costs, promoting sustainability beyond the duration of this project, encouraging other disciplines and specialities to engage in eHealth initiatives, providing an area for further scientific development to improve the service, and providing business opportunities in eHealth.
Methods
The ITTS project was initiated with a launch meeting in Inverness, Scotland in September 2011, attended by all of the international partners. This first knowledge exchange included a review of the five work packages (see Box 2), which provide the structural basis for accomplishing the tasks required to carry out the 10 proposed projects that are outlined below. An international steering group (ISG) has been formed and the international leads have proceeded with recruitment of staff and establishing networks of enthusiastic clinicians for each project that they were importing.
Box 2. ITTS Project structure and work packages.
The implementation of the ITTS project is structured around five work packages:
WP 1 consists of management, coordination and communication for the project through the subcommittees and developing and implementing a strategy for informing policy across the partnership countries.
WP 2 created and sustains the International Telemedicine Advisory Service (ITAS)—a collaboration of academic experts, experienced service providers, clinicians, enterprise and business representatives—to provide expert advice throughout the project and beyond on the selection, design, implementation and evaluation of demonstrator projects, ensuring excellence throughout all stages of the project.
WP 3 involves detailed planning to produce 10 business cases for the demonstrator projects which identified established and successful best practice, chose sites, estimated costs of implementation and potential benefits and created progress indicators. The aim is to make each well-defined project transnational, sustainable and at scale.
WP 4 will implement the 10 demonstrator projects across the northern periphery, utilizing the business plans developed in WP 3. Implementation will involve utilizing end user input, technical expert advice, citizen panels and the media to determine and publicise best practice; plus sourcing and installing the technology, training the users and establishing practical routines and log keeping.
WP 5 will focus on evaluation and sustainability of demonstrator projects using an evaluation toolkit to measure readiness before implementation and the impact of change after implementation; an analysis of health service activity before and after implementation; interviews with stakeholders; a health economics analysis; surveys of staff and patients; the impact on travel by staff and patients and on carbon emissions; and socio-economic scenarios modelling the impact of further implementation of telemedicine. A final project report and a guide entitled ‘Telemedicine into Everyday Practice’ with an interactive checklist will be generated for policymakers and service planners.
In March 2012, the second international conference, held at the National University of Ireland, Galway, Ireland, included workshops to develop the business case for each project of the 10 proposed projects. The business cases, designed to ensure the investments achieve their goals, have been reviewed by the International Telemedicine Advisory Service (ITAS), which has been convened as part of the ITTS project. ITAS is a collaboration of academic experts, service providers and clinicians to advise on the design, implementation, evaluation and dissemination of the ten projects. Government, industry and university, all perform an equally important role in the triple helix partnership concept of interaction, which creates potential for a source of major innovation in this sector (Citation2). Linking into this development of eHealth business will be a wider role of ITAS. ITAS is also providing expert advice regarding the selection, design, implementation, evaluation and dissemination of demonstrator project representatives and will provide expert advice to the ISG throughout the project.
THE TEN PROJECTS
Videoconferencing consultations
Project 1. Speech therapy services. Speech and Language Therapy (SLT) will be administered from a videoconferencing unit in an urban location to patients located in remote locations. Sweden and Scotland previously successfully delivered SLT by this method. Various forms of speech pathology including stroke patients and children with speech difficulties living in remote and island communities will benefit from this remotely delivered therapy which will reduce travel time and costs for both patients and therapists, thereby improving the patient experience and allowing therapists to care for additional patients by freeing up additional clinical time. Population growth, aging, and medical advances that preserve and prolong life have increased demands for health and rehabilitation services and the application of telemedicine technologies offers effective solutions to this challenge (Citation3).
Project 2. Renal services. Renal services in Norway and in one site in Scotland include links between central and remote local renal units. ITTS plans to include more sites and to use videoconferencing to provide communication for outpatient reviews and also for patients receiving home dialysis. In previous telemedicine experiences, renal patients were satisfied with their choice of home dialysis, and many experienced a normalization of daily life, less dominated by disease, along with exhibiting considerable self-management skills and access to the required close contact with the hospital staff for communication and follow-up (Citation4).
Project 3. Emergency psychiatry services. Psychiatric patients in an acute condition could receive consultations close to their home with the possibility of 24-h access to psychiatric specialists for admissions at remote centres through the use of videoconferencing. Norwegian telepsychiatry studies have successfully shown that patients and professionals reported no differences in the quality and satisfaction between face-to-face consultations and cost-effective telemedicine methods. This is a solution for the issue of specialist recruitment difficulties and minimises travel for both patients and carers, which is important for those living in remote locations. Emergency telepsychiatry delivered by videoconferencing has the potential to improve patient care for adults and children in many settings and has been found to be safe and effective, as well as satisfactory to both emergency department staff and to the psychiatric patients treated (Citation5).
Project 4. Remote diabetes services. The diabetes consultant could be situated in a central or urban location and through videoconferencing would carry out reviews with patients who have six-monthly or annual appointments. A diabetes nurse would send the consultant the patient's blood glucose meter reading via the Internet. Podiatry and dietary specialists can also be incorporated into the video consultation process. Previous experience with this system proved satisfactory for patients and medical staff, with less travelling to and from remote areas and faster provision of care, which also improved medication control. Previous studies indicate that both teleconsultation and videoconferencing are practical, cost-effective and reliable ways of delivering a worthwhile healthcare service to diabetics (Citation6).
Smartphone and internet-based mobile self-management
Project 5. Tracking physical activity. Sedentary lifestyles are a major concern for governments of developed countries as physical inactivity has been related to increased mortality, lower quality of life and a higher risk of obesity and illnesses, which result in a higher rate of healthcare and hospital visits (Citation7). The majority of smartphones are equipped with miniature accelerometer sensors, which are a reliable method of monitoring mobility in the form of step count (Citation8). This makes them a viable device to track and monitor physical activity within the adult/ adolescent communities. By carrying their smartphone with a pedometer application running in the background, the person will receive biofeedback by providing charts and graphs at any time during the day to the user to enable them to see if they have reached their daily goal. The patient will then report back to the clinician with the data in their smartphone. B. J. Fogg's concept of ‘captology’ (computers as persuasive technology) examines how people are motivated or persuaded while interacting with computers and mobile technologies and this motivation can aid the behaviour change required to increase physical activity for the benefit of their health (Citation9).
Project 6. Support for diabetes. Smartphone self-help tools provide the potential for the patient to input to their phone food intake, physical activity and blood glucose measures and goals thereby allowing them to self- monitor. In some cases, patients can also request an appointment, check laboratory results or ask the healthcare provider a question using a telephone or internet-based application. Handheld communicating devices, such as smartphones, loaded with software to apply physicians’ prescriptions, have been shown to improve glycaemic control. These systems provide immediate assistance to the patient (such as insulin-dose calculation and food choice optimization at meals), and all the data stored in the smartphone can be transmitted to authorized caregivers, enabling remote monitoring and even teleconsultation. The widespread use of smartphones should be of particular value for overcoming the relative shortage of doctors and reducing the health costs associated with a disease of such epidemic proportions.
Project 7. Inflammatory bowel disease. Previous studies have used landline telephones to monitor inflammatory bowel disease (IBD) patients with improvement in satisfaction with their care. An IBD smartphone application has been developed for patients to record their symptoms and their adherence to medication schedules. These data will be transmitted over the mobile phone network to a central computer where custom designed software has been configured with parameters for the acceptable level of symptoms for the patient. If there is a deviation, both the patient and the IBD nurse will receive an alert and the IBD nurse will then contact the patient. Based on a clinical protocol, the nurse will use this service to advise the patient on their care. The use of this technology is expected to assist in the careful monitoring of IBD patients to help maintain their quality of life and reduce hospital admissions.
Home-based health services
Project 8. Remote support in medical and social care emergencies. To assist individuals with various health and/or social needs to live a more independent and safe lifestyle, a range of telecare technologies have been implemented. Local health, housing and social care partnerships are particularly interested in the further development of telecare technology. Basic telecare packages include a base unit, body transmitter and smoke detectors for the home. The enhanced telecare package consists of various peripheral sensors, which include epilepsy sensors and DDA (Disability Discrimination Act) pagers for people with sensory impairments. The alarms and devices are linked to a call centre and trigger a response when the person requires assistance. Integration of telecare and videoconferencing requires further evaluation to determine if this will further improve patient care and reduce the numbers of false alerts. The report ‘Development of Telecare 2006–2010’ examines the growth and development of telecare in Scotland from 2006 to 2010 and provides an assessment of telecare funding against measurable goals (Citation10).
Project 9. Remote exercise classes for rehabilitation. Patients with long-term conditions living remotely may not be able to attend rehabilitation exercise groups due to distance and difficulty travelling. Also, travelling can exhaust the patient, so even if they can attend a clinic they are often too tired to reap the full benefit of the exercise classes. Videoconferencing units can be set up in the home and in the clinic to allow patients to perform the exercises in the comfort of their own home while benefitting from the same social, educational and clinical benefits of those attending the clinic. The physiotherapist can monitor the home patients using equipment such as a pulse oximeter and can also speak with all the patients and they can interact with each other. The patient can thus perform the exercises when rested and at home. Further advantages can be added such as saving the exercise programme for patients to revisit to exercise on their own. Remote pulmonary rehabilitation programmes are now a routine service in NHS Tayside and NHS Lothian areas. A full report can be found at http://www.sctt.scot.nhs.uk/wp-content/uploads/2012/11/remotepr.pdf (Citation11).
Project 10. Home-based service delivery for patients with multimorbidity. Home monitors for chronic obstructive pulmonary disease (COPD), surgery and community telehealth monitors have been piloted in an effort to reduce crisis hospital admissions and allow for remote monitoring. A touch screen ‘pod’ allows a patient to report symptoms, measure oxygen saturation, weight, body mass index (BMI), pulse, blood pressure and responses about general health. This information is then sent via wired or wireless broadband to a secure server through a firewall into a computer to safeguard data, or in some cases, directly into the electronic patient records. Daily monitoring of the website by health professionals using set parameters and clinical judgment can raise an alert when there are changes in the patient's condition that require intervention. The patient can then be contacted or the information can be passed on to the relevant healthcare teams to respond with an appropriate intervention. Previous patient evaluations indicated that patients feel the benefits include: independence with a sense of security that their condition is being monitored; improved knowledge of and thereby management of their own condition; support for their carers or families through this monitoring, reduced need to contact their healthcare provider if they are stable and also fewer emergency hospital admissions.
Expected Results
All projects undergo a rigorous process of evaluation led by a research fellow employed directly by the project. This fellow visits all project sites and evaluates quantitatively and qualitatively participants and staff involved. Where appropriate, in order to enhance sustainability, additional analysis on efficacy, effectiveness and cost effectiveness is performed depending on the design and local context of the project.
It is anticipated that the demonstrator projects will stimulate the further development of these practices in remote and rural areas. This will allow patients to remain either in their communities or at home. Unnecessary travel, by both patients and healthcare staff will be reduced thereby reducing the carbon footprint of remote healthcare. The elderly or less mobile patients will have increased potential to access equal healthcare to those living in urban areas, which they might otherwise be unable to avail themselves of. The viability of the remote, peripheral and rural regions of the Northern Periphery may be retained through narrowing the social and economic differences between different regions of Europe.
Future innovations revolving around provision of remote health services will be of further benefit to businesses and communities. Extensive information and documentation of the procedures, outcomes and impact of the various telemedicine healthcare projects and dissemination of these to service providers, health policy planning officials and the public will ensure that further uptake and innovation will ensue. With increased demand there will be motivation for the technology to improve and become more readily available which will further the potential for an increased provision of this remote healthcare option.
DISCUSSION
International aspects
International collaboration between the six partner countries has allowed access to an extensive panel of experts from other countries and for all partners to benefit of their varied experiences. The countries are at various stages of experience with different aspects of telemedicine and its accompanying technology and the intercommunication allows for building on each other's knowledge and striving forward towards improvements.
Various challenges occur with international collaboration. Different regulations and healthcare systems require adjustments in approach to the implementation of the 10 demonstrator projects. Reporting of confidential data in a secure fashion via telecommunication methods such as mobile phones, videoconferencing and the internet requires careful consideration of the methods of transmission. Language differences create an additional challenge for three of the countries; however, all can communicate in English, and therefore, this is the language used in meetings, conferences and written documents.
Our extensive communications policy facilitates contact between all the team members carried out by email, teleconferencing and videoconferencing, and at six-monthly face-to-face conferences rotated through the countries. Initial communications focused on determining which countries would be implementing the 10 demonstrator projects, developing interest and collaboration with enthusiastic clinical teams and producing business cases. The ITTS website http://www.transnational-telemedicine.eu was developed to disseminate information regarding the projects, partners, ITAS and a forum for displaying news and events. This web site includes an intranet to enable internal communications in the form of working documents, business cases, project manuals, meeting information and reports, work packages and progress reports. It is also possible to sign up to a mailing list on the web site to receive the ITTS newsletter.
Reflection
With the governance structures in place, leadership from Scotland while remaining cognisant of international and cross-cultural differences, the international project partners have begun the process of transnationalizing the demonstrator projects. The challenges of different languages, countries, healthcare systems and communities being involved in a project of this scale are obvious.
There have been a few key components to the successful progression of the project to date which are worth reflecting on. Firstly, efficient leadership have been vital to the on-going progress and success of the projects. This leadership needs to be provided not only by the lead partner for the day to day running on the project but also needs to be devolved in terms of responsibility and delivery across all the work packages and individual projects.
Secondly, clear lines of communication particularly around meetings and actions are vital and indeed technology such as videoconferencing can play an important role in delivering the same.
Finally, the success of individual projects in the health arena will often rise or fall on the basis of motivated clinical teams. Therefore, it is imperative to devote time and energy, often much more than anticipated, in building up such networks across partner countries.
Access to knowledge and experience from previous projects, extensive teamwork with joint decision making and a shared vision has helped progress the outlines of projects to viable frameworks for implementation of the telemedicine health solutions outlined in the project proposal.
Conclusion
The goal of the six countries comprising the ITTS team, aided by the NPP, is sustainable leading edge eHealth delivery via new technologies across the remote and rural areas of the Northern Periphery regions of Europe. The ITTS team encourage all healthcare providers to at least explore possible technological solutions within their own context. Familiarization with its capabilities will broaden comprehension of the immense benefit possible in improving healthcare delivery for not only rural and remote patients but communities everywhere. In addition, it provides increased professional satisfaction and the delivery of more cost-effective healthcare.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
REFERENCES
- http://www.northernperiphery.eu (accessed 17 June 2012).
- http://www.triplehelixconference.org (accessed 17 June 2012).
- Mashima PA, Doarn CR. Overview of telehealth activities in speech-language pathology. Telemed J E Healt. 2008;14:1101–17.
- Rygh E, Arild E, Johnsen E, Rumpsfeld M. Choosing to live with home dialysis-patients’ experiences and potential for telemedicine support: A qualitative study. BMC Nephrol. 2012;13:13.
- Yellowlees P, Burke MM, Marks SL, Hilty DM, Shore JH. Emergency telepsychiatry. J Telemed Telecare. 2008;14:277–81.
- Verhoeven F, van Gemert-Pijnen L, Dijkstra K, Nijland N, Seydel E, Steehouder M. The contribution of teleconsultation and videoconferencing to diabetes care: A systematic literature review. J Med Internet Res. 2007;9:e37.
- Varo JJ, Martínez-González MA, Martínez JA. Obesity prevalence in Europe (in Spanish). An Sist Sanit Navar. 2002;25 (Suppl. 1):103–8.
- Culhane KM, O’Connor M, Lyons D, Lyons GM. Accelerometers in rehabilitation medicine for older adults. Age Ageing. 2005;34: 556–60.
- Stanford Persuasive Tech Lab. What is captology? http://captology.stanford.edu/about/what-is-capatology.html (accessed 20 June 2012).
- Joint Improvement Team. http://www.jitscotland.org.uk/publications-1/telecare/ (accessed 19 December 2012).
- Evaluation of remote pulmonary rehabilitation in Scotland. http://www.sctt.scot.nhs.uk/wp-content/uploads/2012/11/remotepr.pdf (accessed 22 June 2012).