Sirs,
Rhinophyma is a disfiguring nasal skin disorder affecting primarily Caucasian men in their fifth to seventh decades of life (Citation1). It is characterized by hypervascularity, sebaceous gland hyperplasia, occluded sebaceous ducts, cysts and dermal fibrosis (Citation2). The aetiopathogenesis of rhinophyma is unclear but it is considered to be the final stage of rosacea. This condition can be socially very limiting and functional impairments such as nasal obstruction may also occur (Citation1,Citation3).
There is currently no effective medical treatment for rhinophyma. Surgical excision, dermabrasion, dermaplaning, electrosurgery, electrocautery and cryosurgery have all been used (Citation2,Citation4). Treatments with several ablative lasers such as CO2, erbium:yttrium-aluminium-garnet (Er:YAG) or argon lasers as well as non-ablative diode lasers have been reported with good results (Citation1,Citation5).
We present a patient with cystic lesions associated with rhinophyma who was successfully treated with an ablative fractional laser system. To our knowledge, this is the first such case reported.
A 66-year-old male patient with Fitzpatrick type III skin was referred to our consultation for a mild–moderate rhinophyma with numerous cystic lesions (). Electrocautery could not be performed previously due to non-tolerance of the patient. His medical history included prostate adenocarcinoma which was successfully treated.
Figure 1. Mild–moderate rhinophyma with numerous cystic lesions before treatment.

Three consecutive passes with an ablative fractional yttrium-scandium-gallium-garnet (YSGG) laser at a wavelength of 2790 nm (Pearl Fractional; Cutera, Brisbane, CA, USA) were performed. A scan size of 10 × 14 mm, a spot size of 300 μm, a pulse width of 600 ms, a fluence of 240 mJ per microspot and an approximate density of 8% per pass were used. Before laser treatment, a cream containing a lidocaine base and a prilocaine base (eutetic mixture of local anaesthetics) was applied topically under occlusion for 2 hours to reduce pain.
Post-laser care consisted of gentle steaming, dilute acetic acid compresses three times a day for a week and daily application of a topical antibiotic ointment (Fucidine©) until spontaneous detachment of the scab. Sunscreen with a sun protection factor of 50 was applied for up to 2 months after therapy to prevent postinflammatory hyperpigmentation.
Six days after laser treatment, erythema and crusts were seen but improvement of the cystic lesions associated with rhinophyma could not be clearly appreciated (). One month after laser therapy, marked improvement of the cystic lesions was seen without any significant side effects. This improvement has remained stable for 6 months ().
Figure 2. Crusts and partial improvement could be seen 1 week after laser treatment.

Figure 3. Marked improvement of cystic lesions 3 months after laser treatment.

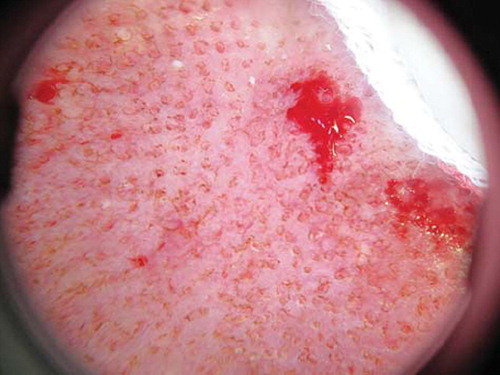
Ablative fractional lasers have been used for rhytides, lentigines, dermal elastosis and scars. These devices create small zones of microdamage to skin separated by untreated zones that serve as reservoirs for wound healing (). Subsequently, in comparison with full-surface ablative lasers, rapid wound healing with a low risk of side effects is seen (Citation6,Citation7).
Figure 4. Dermoscopy immediately after laser treatment: small, round treated zones are separated by unaffected zones.
Three wavelengths are used for ablative fractional systems: CO2 (10 600 nm), Er:YAG (2940 nm) and YSGG (2790 nm) (Citation6). The YSGG fractional laser delivers 300-μm diameter microcolumns that penetrate from 300 to 1500 μm with 40–60 μm of residual thermal damage (RTD). The YSGG laser has a greater water absorption coefficient than the CO2 laser, which theoretically allows finer control of the damage depth. Likewise, the YSGG laser provides greater RTD than the Er:YAG laser but less than the CO2 laser, preventing significant bleeding with fewer incidences of side effects.
In our patient, no clear improvement was seen 6 days after treatment, but 1 month later almost complete resolution of the cystic lesions was observed. We believe that this could be due to progressive transepidermal elimination of sebum through the ablated microcolumns. Another mechanism which could be involved was the overheating of sebaceous glands and the consecutive decreasing of sebum production.
In this case, treatment of cystic lesions related to mild–moderate rhinophyma with an ablative fractional YSGG laser was a safe and effective treatment, with no associated complications. More studies are needed to confirm this result. Moderate or severe cases of rhinophyma probably need more aggressive treatments.
Acknowledgement
The authors declare that they have no conflicts of interest. No funding was received for this manuscript.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Madan V, Ferguson JE, August PJ. Carbon dioxide laser treatment of rhinophyma: A review of 124 patients. Br J Dermatol. 2009;161:814–818.
- Vural E, Royer MC, Kokoska MS. Sculpting resection of rhinophyma using the Shaw scalpel. Arch Facial Plast Surg. 2009;11:263–266.
- Sadick H, Goepel B, Bersch C, Goessler U, Hoermann K, Riedel F. Rhinophyma: Diagnosis and treatment options for a disfiguring tumor of the nose. Ann Plast Surg. 2008;61:114–120.
- Kempiak SJ, Lee PW, Pelle MT. Rhinophyma treated with cryosurgery. Dermatol Surg. 2009;35:543–545.
- Apikian M, Goodman GJ, Roberts S. Management of mild to moderate rhinophyma with a 1,450-nm diode laser: Report of five patients. Dermatol Surg. 2007;33:847–850.
- Metelitsa AI, Alster TS. Fractionated laser skin resurfacing treatment complications: A review. Dermatol Surg. 2010;36: 299–306.
- Dierickx CC, Khatri KA, Tannous ZS, Childs JJ, Cohen RH, Erofeev A, . Micro-fractional ablative skin resurfacing with two novel erbium laser systems. Lasers Surg Med. 2008; 40:113–123.