Sirs,
The carbon dioxide (CO2) fractional laser is a widely used device for the treatment of fine wrinkles, acne scars and pigmentation. The mechanisms of action of CO2 laser resurfacing include tissue ablation, immediate collagen shrinkage and dermal collagen remodelling (Citation1). Down time with the CO2 laser typically lasts a week or more.
The growing demand for minimizing down time for patients has resulted in the development of non-ablative lasers for photorejuvenation treatment. Non-ablative lasers include near-infrared lasers and intense pulsed light devices. However, non-ablative lasers have only minimal effects on neocollagenesis, thereby not providing the same results as ablative laser resurfacing for the treatment of wrinkles and scars (Citation2).
Recently, fractional photothermolysis has been widely used for photorejuvenation treatment. Fractional photothermolysis is achieved by applying an array of microscopic treatment zones of thermal injury to the skin (Citation3). Microscopic epidermal necrotic debris is formed just below an intact stratum corneum overlying each dermal wound. Although fractional thermolysis has shown acceptable clinical outcomes with less down time for patients and fewer overall adverse effects, the down time associated with ablative fractional laser treatment still remains a problem.
There has been no objective method reported that can be universally used to assess down time. With the CO2 fractional laser, the most significant problem with the long down time is that microcrusts remain on patients’ faces – the micronecrotic debris is observed in areas where the laser beam has penetrated. The down time might be accurately assessed by counting these microcrusts. Therefore, a randomized controlled split-face study was performed in patients with CO2 fractional laser treatment.
A recent study reported that the CO2 laser impacts local tissue secretion of transforming growth factor (TGF)-β1 and basic fibroblast growth factor (bFGF) (Citation4). These cytokines play an essential role in wound healing, especially collagenesis (Citation5). The additional topical application of growth factors including TGF, FGF, EGF (epidermal growth factor) and VEGF (vascular endothelial growth factor) might minimize patient down time. The experimental side of the face had a solution with growth factors applied and was compared with the control side of the face where normal saline was applied. The number of microcrusts per unit area was counted on the fourth day after laser treatment.
A randomized controlled split-face study was performed on patients who wanted to have photorejuvenation using the CO2 fractional laser. All the patients were women (mean age: 55 ± 2.45 years) with Fitzpatrick skin types III–IV who had developed photoaging on their face (). The study protocol was approved by the local ethics committee. Written and verbal information including risks, benefits, and potential complications was given to the patients, and a written informed consent was obtained.
Table I. Microcrust counts on day 4, bilaterally.
All the patients had full-face CO2 fractional laser treatment (Linexel™; UTI Co. Ltd, Seoul, Korea). The spot size was fixed at 30 μm and the pulse energy was also fixed at 30 mJ per pulse. The number of laser shots per square centimeter was constantly controlled to a total of 196. The pulse duration was also constantly controlled at 160 μs.
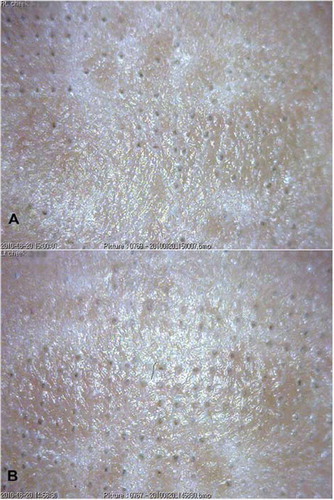
After laser treatment, the face was divided into left and right. Each side of the face was randomly chosen for application of the growth factors (Neotis SGF61™; Caregen Co. Ltd, Mediway, Korea) or normal saline. The product with growth factors included: insulin-like growth factor (IGF)-1, VEGF, basic fibroblast growth factor (bFGF), acidic fibroblast growth factor (aFGF), EGF and TGF-β3 (0.0001% W/W, respectively), in addition to amino acids, vitamins, coenzymes, nucleic acids and minerals such as magnesium (0.01% W/W), potassium (0.04% W/W), calcium (0.02% W/W) and sodium (0.02% W/W). On the fourth day after laser treatment when the crusts on the face typically began to fall off, photographs of the surface of the face at the zygomatic prominent areas, bilaterally, were taken 2 cm down from the lateral margin of the patients’ eyes. A digital microscope (AM313T, Dino-Lite™; AnMo Electronics Co., Taiwan) with 22-fold original magnification was used (). Using the photographs, the number of microcrusts was counted by investigators blinded to the treatment. The mean, standard deviation and paired t-test were performed with the Statistical Package for the Social Sciences v. 16.0 (SPSS, Chicago, IL, USA).
Figure 1. Patient number 6. (A) Side of the face with growth factor application. The microcrust count was 90 as assessed by digital microscope evaluation (per 1.6 × 1.2 cm2; original magnification × 22). (B) Side of the face with normal saline application. The microcrust count was 115. The photography was performed symmetrically on both sides 2 cm down from the lateral margin of the eyes.
The results showed no significant differences in the number of microcrusts between the side of the face with growth factors and the normal saline side (, p > 0.05). The mean number of microcrusts on the side with growth factors (115.6 ± 185.6 per 1.6 × 1.2 cm2) was slightly lower than on the side with normal saline (128.7 ± 305.0 per 1.6 × 1.2 cm2), but the difference was not statically significant. Among the patients, one temporarily showed folliculitis and one presented with a mild itching sensation on the side spread with growth factors. However, significant side effects were not observed.
Theoretically, the topical application of growth factors is beneficial for wound healing. Recently, it was reported that the topical application of bFGF and PDGF was effective for the management of mucosal lesions related to graft-versus-host disease (Citation6). Gold et al. presented that human growth factor cream showed efficacy for skin rejuvenation after a micro-laser peel (Citation7,Citation8). However, in our study, the results showed that the application of growth factors was not effective. There are two main factors that might account for the different results. First, is the difference between the vehicles. Gold et al. used human growth factors in combination with a hyaluronan serum whereas the mixture in our study was dissolved in water. Second, is the application method. In our study the growth factors were applied only once, just after CO2 fractional laser treatment, whereas in Gold et al.'s study the hyaluronan serum with human growth factors was applied daily for a month.
We conclude that more frequent application of growth factors might be beneficial for wound healing and a higher concentration of growth factor might be needed to decrease the down time. A change of vehicle, such as to a cream or ointment, might increase the absorption rate of the topical application of growth factors. Also, a larger number of patients might provide significant differences. To our knowledge, this is the first study to investigate the topical application of a growth factor solution on patients after CO2 fractional laser treatment. A novel non-invasive assessment method, counting the number of microcrusts by digital microscope, was developed for evaluating the state of wound healing after laser treatment.
Acknowledgement
This work was supported by the SRC/ERC program of MOST/KOSEF (R11-2005-017-05003-0) and Basic research program through the NRF funded by the Ministry of Education, Science and Technology (2010-0002431).
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Ross EV, McKinlay JR, Anderson RR. Why does carbon dioxide resurfacing work? A review. Arch Dermatol. 1999;135: 444–54.
- Gold MH. Update on fractional laser technology. J Clin Aesthet Dermatol. 2010;3:42–50.
- Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional photothermolysis: A new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004;34:426–38.
- Manolis EN, Kaklamanos IG, Spanakis N, Filippou DK, Panagiotaropoulos T, Tsakris A, . Tissue concentration of transforming growth factor beta1 and basic fibroblast growth factor in skin wounds created with a CO2 laser and scalpel: A comparative experimental study, using an animal model of skin resurfacing. Wound Repair Regen. 2007;15:252–7.
- Prignano F, Campolmi P, Bonan P, Ricceri F, Cannarozzo G, Troiano M, . Fractional CO2 laser: A novel therapeutic device upon photobiomodulation of tissue remodeling and cytokine pathway of tissue repair. Dermatol Ther. 2009; 22(suppl 1):S8–15.
- Picardi A, Lanti A, Cudillo L, Cerretti R, Dentamaro T, De Angelis G, . Platelet gel for treatment of mucocutaneous lesions related to graft-versus-host disease after allogeneic hematopoietic stem cell transplant. Transfusion. 2010;50: 501–6.
- Gold MH, Cohen J, Katz B. High content hyaluronan serum combined with human growth factor and cytokine skin cream as regimen for pre- and post-micro-laser-peel skin and wound care. J Am Acad Dermatol. 2007;56(suppl 2): AB203.
- Gold MH, Katz B, Cohen J, Biron J. Micro laser peel in combination with topical hyaluronan and human growth factors: An efficient regimen for skin rejuvenation. J Am Acad Dermatol. 2008;58(suppl 2):AB141.