
Sir,
Erythema ab igne (EAI) is a persistent reticular macular dermatosis caused by repeated and prolonged subthreshold thermal exposure. It begins as mottling caused by local hemostasis and becomes a reticulated erythema, leading to epidermal atrophy and pigmentation, and occasionally skin ulcers and epithelial atypia. Recently, exposure to various kinds of heat sources, such as heated furniture, car heaters, and even laptop computers, has been reported to cause this condition (Citation1). Reactive angiomatosis can sometimes accompany EAI, and vascular proliferation also appears to be a reactive response to the effect of heat (Citation2).
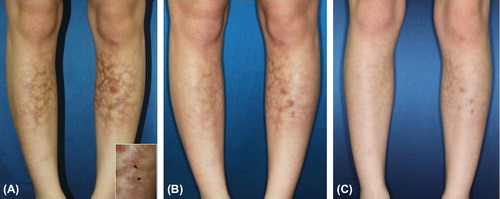
A 22-year-old woman presented with mottled erythematous patches and atrophic scars on both lower legs; she had had these problems for three months after using an electric heater in her workplace. A biopsy of an erythematous patch revealed no epithelial atypia but increased amounts of elastic tissue and melanin pigment in the dermis. A biopsy from a scar lesion yielded similar findings, with reactive proliferation of small blood vessels (). Based on the clinical and histological findings she was diagnosed as EAI. Because scars were accompanied on the lesions, we started active treatment with 1,064-nm low fluenced Q-switched Neodymium-Doped Yttrium Aluminum Garnet (QS Nd-YAG) laser, so called “laser toning”, at weekly intervals. Treatment was with settings of 1.4 J/cm2, 7-mm spot size, and 3 passes with appropriate overlapping. During the course of treatment, the patient did not use any topical agents. Only after one treatment the lesions showed clinical improvement, and with regular treatment, remission continued. After six treatments, the situation was much improved, with good cosmetic results ().
Figure 1. (A) The biopsy specimen from atrophic scar lesion (B) Biopsy from erythematous patch (H&E, X200, inlet: fontana silver stain).
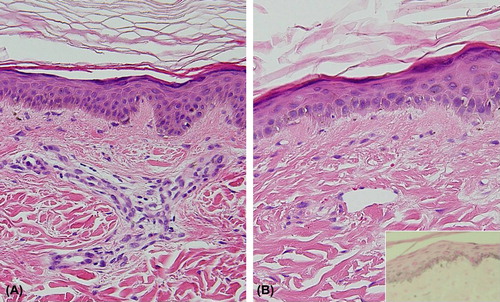
Figure 2. (A) Diffuse reticulated brownish patches with atrophic scars on the anterior aspect of the both lower legs (B) Clinical improvement after first session, and (C) six session of treatments with low fluence 1,064-nm QS Nd:YAG laser (inlet: biopsy sites).
Acute-stage erythematous lesions in EIA typically fade over months, whereas the hyperpigmentation associated with more chronic lesions may persist for years. Although a variety of treatment modalities including imiquimod cream and Kligman's formula have been used, their effects are not satisfactory. Laser toning is commonly used to treat pigmentary disorders such as melasma and post-inflammatory hyperpigmentation, based on a concept of subcellular selective photothermolysis and expanding the clinical boundaries (Citation3). To date, Cho et al. (Citation4) have reported the only successful treatment of EAI with 1064 nm laser toning. We believe that the present case involved severe chronic advanced stage of EIA since it was accompanied by spontaneous ulcers and atrophic scars. We performed the laser treatment after confirming that there was no microscopic evidence of atypia. Although we do not have a clear explanation for the action mechanism of laser toning on the EAI, it is likely that subcellular selective photothermolysis is involved, as in other pigmentary disorders. Considering that changes of elastic fibers after chronic exposure to infrared light may be a common pathogenesis in photoaging and EAI, and successful results could be obtained for various kinds of scars by laser toning, 1,064 QS-Nd:YAG laser may be a useful treatment option for EAI (Citation5). Further studies are needed to identify more precise pathophysiological effects of laser toning, as well as its therapeutic effects and safety.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Bilic M, Adams BB. Erythema ab igne induced by a laptop computer. J Am Acad Dermatol. 2004;50:973–974.
- Mitsuhashi T, Hirose T, Kuramochi A, Tsuchida T, Shimizu M. Cutaneous reactive angiomatosis occurring in erythema ab igne can cause atypia in endothelial cells: potential mimic of malignant vascular neoplasm. Pathol Int. 2005;55:431–435.
- Kim JH, Kim H, Park HC, Kim IH. Subcellular selective photothermolysis of melanosomes in adult zebrafish skin following 1,064-nm Q-switched Nd:YAG laser irradiation. J Invest Dermatol. 2010;130:2333–2335.
- Cho S, Jung JY, Lee JH. Erythema ab igne successfully treated using 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low fluence. Dermatol Surg. 2011; 37:551–553.
- Dang Y, Ren Q, Li W, Yang Q, Zhang J. Comparison of biophysical properties of skin measured by using non-invasive techniques in the KM mice following 595 nm pulsed dye, 1,064 nm Q-Switched Nd:YAG and 1,320 nm Nd:YAG laser non-ablative rejuvenation. Skin Res Technol. 2006;12: 119–125.