Abstract
Background and purpose Population data on mortality and life expectancy are generally available for most countries. However, no longitudinal data based on the health-related quality of life outcome from the EQ-5D instrument have been reported for orthopedic patients. We assessed the effect of orthopedic surgery as measured by EQ-5D.
Methods We analyzed EQ-5D data from 2,444 patients who were operated at the Department of Orthopedic Surgery at Karolinska University Hospital, 2001–2005. We also made a comparison between results from this cohort and those from a Swedish EQ-5D population survey.
Results The mean EQ-5D index score improved from 0.54 to 0.72. Hip and knee arthroplasty, operations related to previous surgery, trauma-related procedures, and rheumatoid arthritis surgeries had preoperative EQ-5D index scores of 0.48 to 0.52. All of these groups showed substantial improvement in scores (0.63 to 0.80). Patients with tumors or diseases of the elbow/hand showed higher preoperative scores (0.66 to 0.77), which were similar postoperatively. In most patients, the EQ-5D index score improved but did not reach the level reported for an age- and sex-matched population sample (mean difference = 0.11).
Interpretation Our results can be used as part of the preoperative patient information to increase the level of patient awareness and cooperation, and to facilitate rehabilitation. In future it will be possible—but not easy—to use the EQ-5D instrument as a complementary consideration in clinical priority assessment.
Musculoskeletal conditions are the leading cause of severe long-term pain and disability in the world, affecting hundreds of millions of people (Woofle and Pfleger Citation2003). They are also the main cause of disability in older age groups, and rank among the top 10 causes of disability-adjusted life-years (DALY) in Europe (CitationWHO 2006). This has been recognized by the World Health Organization, endorsing the Bone and Joint Decade (2000–2010) (Woolfe Citation2000). Osteoarthritis is the fifth greatest cause of years lived with disability (YLD) in high-income countries (The Word Bank Citation2006). During the year 2007, 114,000 patients underwent a primary hip or knee joint replacement operation in the UK (CitationEngland and Wales National Joint Registry 2009). Prevalence data from Sweden for the same year show that 1 in 15 elderly women had a knee arthroplasty (CitationSwedish Knee Arthroplasty Register 2009). One of the major goals of the Bone and Joint Decade has been to reduce the burden and cost of musculoskeletal disorders for individuals, healthcare providers, and society in general. At the end of the decade, it is now appropriate to reflect on the outcome of orthopedic surgery.
Improvement in health-related quality of life (HRQOL) is one of the most important goals of orthopedic surgery (Ethgen et al. 2006, Jansson et al. Citation2009). There are several HRQOL instruments available. Among these, the generic instruments can be used for diverse patient groups independently of the underlying disease or disability. Generic instruments include, for example, the EQ-5D (EuroQol), the SF-6D (derived from RAND-36/SF-36), the HUI (Health Utilities Index Mark II/Mark III), and the AQoL (Assessment of Quality of Life) (Kopec and Willison Citation2003). The SF-36 instrument is most commonly used. Most studies have concentrated on specific orthopedic interventions, and most of them show improved HRQOL after surgery (Towheed and Hochberg Citation1996). HRQOL has been used to evaluate the effect of surgical procedures (Hoffmann et al. Citation2006, Akahane et al. Citation2007). Treatment outcome across various elective orthopedic surgical procedures has been compared (Hansson et al. Citation2008, Anderson et al. Citation2009, Osnes-Ringen et al. Citation2009). Generic tools have also been used for the estimation of orthopedic effectiveness of healthcare (Räsänen et al. Citation2006). The generic health-related quality of life instrument—EQ-5D—allows both a description of health status along 5 dimensions and the evaluation of health or the estimation of a health summary score: the EQ-5D score on a scale where 0 is death and 1 is full health (Dolan Citation1997, Brooks et al. Citation2003). The instrument has been included in population surveys in more than 10 countries (Kind et al. Citation1998, Burström et al. Citation2001, Scende and Williams Citation2004). HRQOL and health status measures have often been used as outcomes in clinical trials and studies assessing a variety of orthopedic interventions (Tidermark et al. Citation2003, Cockerill et al. Citation2004, Jansson et al. Citation2005, Löfvendahl et al. Citation2005, Rivero-Arias et al. Citation2005, Odenbring et al. Citation2008, Giannoudis et al. Citation2009).
The EQ-5D is short and easy to use, and shows good responsiveness (Tidermark et al. Citation2003), i.e. it is capable of capturing clinically important changes. Moreover, it also allows combination of different dimensions of health to form an overall index, the EQ-5D index score, as required for healthcare evaluations and for construction of quality-adjusted life-years (QALYs), a measure frequently used in cost-effectiveness analyses (Gold et al. Citation1996, Meunning and Gold Citation2001, Drummond et al. Citation2005).
Population data on mortality and life expectancy are generally available for most countries. However, no longitudinal data based on the inclusion of the HRQOL outcome by the EQ-5D have been reported in a clinical setting of orthopedic patients. We therefore introduced the EQ-5D instrument at our department in order to measure all patients selected for elective orthopedic operations. The aim of this study was to preoperatively evaluate the HRQOL in our cohort regardless of other co-morbidity factors and also to make a comparison between this cohort and a Swedish EQ-5D population survey. In addition, we wanted to assess the postoperative outcome by the EQ-5D instrument in order to have output data to explore the potential of EQ-5D for medical priority and health economy calculations. We report data from 2,444 patients.
Patients and methods
Study population
Between January 2001 and May 2005, 4,715 elective orthopedic operations were performed at the Department of Orthopedic Surgery, Karolinska University Hospital. We included 4,011 patients during this period, all of whom completed the EQ-5D questionnaire. Acute operations were not included.
The enrollment of patients was done at the ward, and informed consent was given by all patients. At baseline, i.e. on the day before surgery, the first EQ-5D questionnaire was completed by the patient at the ward. The 12-month EQ-5D questionnaire was sent once to the patients by mail 11 months after surgery once, with no reminders. To be included in the 12-month follow-up, patients had to have answered the EQ-5D questionnaire within 3 months. 2,444 patients completed the 12-month EQ-5D questionnaire within 15 months postoperatively. We performed a drop-out analysis of the 1,567 patients who did not answer the 12-month follow-up questionnaire. Age, sex, type of surgery, and preoperative EQ-5D data were scrutinized.
We divided the cohort into 15 groups according to anatomical region and type of surgery. We also compared EQ-5D results for patients older than 20 years of age with those from a Swedish population survey involving 3,069 individuals (Burström et al. Citation2001, Citation2003).
The study design was approved by the ethics committee of Karolinska Institutet (no. 03-631).
Outcomes: the EQ-5D measure
Health-related quality of life data were obtained from the EQ-5D, a self-administered patient questionnaire (CitationEuroQol Group 1990, Brooks Citation1996, Dolan et al. Citation1996). The EQ-5D respondents classify their own health status into 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression with 3 levels of severity (no problems, moderate problems, or severe problems). Dolan et al. (Citation1996) used the time trade-off (TTO) method to rate these different states of health in a large UK population (UK EQ-5D index tariff). As there is no Swedish TTO tariff for EQ-5D health states, and since the only Swedish population survey to assess the EQ-5D used the UK tariff, we used the preference scores generated from the UK population when calculating the EQ-5D index scores for our study population. The patients completed the Swedish-translated questionnaire (EQ-5D 2009). By design, this descriptive system is able to identify 243 unique health states. An index score can be assigned to each of these health states to indicate its value or desirability from the point of view of the general public. Scores in the UK EQ-5D value set range from –0.594 for the worst possible health state to 1.0 for a perfect state of health, with 0 on the scale representing the state of being dead. Negative scores suggest that the corresponding health states are considered worse than being dead. Normally, the EQ-5D questionnaire needs 1 to 3 min for self-completion.
Statistics
The EQ-5D index scores are reported as mean (SD). Age and sex standardized EQ-5D index scores at baseline (preoperatively and at 12 month follow-up (postoperatively) was calculated as the difference between observed scores and the age- (10 year age-groups) and sex-specific mean scores in the population survey. These preoperative and (12-month) postoperative EQ-5D index standardized scores are reported as mean (SD).
The changes in EQ-5D index score from baseline (preoperatively) and 12 months (postoperatively) were calculated and a paired t-test was used to test whether the change from baseline was equal to 0. We also analyzed the fraction of patients (by number and percentage) whose EQ-5D index score changed from baseline to 12 months (improved or deterioriated by > 0.1). Responders and non-responders at the 12-month follow-up were compared regarding age, sex, type of surgery, and preoperative EQ-5D by chi-square tests for qualitative variables and t-tests for quantitative variables. Even though the distribution of the change from baseline was not normal, the central limit theorem implies valid inference using the t-test when the sample size is more than about 30, and all but 1 subgroup had larger sample sizes. Since the fraction of responders was different for the different types of surgery, the comparisons with respect to age, sex, and preoperative EQ-5D score were also adjusted for this difference by analysis of variance and logistic regression.
Results
The final analysis included 2,444 patients, 57% of whom were women, and the mean age at surgery was 56 (SD 18) years (). One third of the patients had osteoarthritis and were operated on for hip or knee replacement. 13% of the patients had operations due to complications after previous surgery. 1 in 10 had trauma related to surgery, and 1 in 10 was operated due to knee disorders. 1.4% had an unknown, unidentified operation procedure code.
Table 1. Details of the 2,444 patients in the study at baseline (preoperatively), including surgical procedures and anatomical regions
The mean preoperative EQ-5D index score at baseline was 0.54, which is 0.29 units lower than would be expected in a population-based sample of the same age and sex distribution. On average, women had lower scores (0.50) than men (0.59) before surgery (p < 0.001), which remained unchanged after adjustment for age and type of surgery. Age did not affect the preoperative score substantially, with the exception of patients younger than 30 years, who had a higher mean score (by 0.12 units) than the average patients. This age effect could to some extent be explained by type of surgery. The different surgical procedures showed a wide spectrum of average EQ-5D index scores at baseline (0.30–0.77).
When comparing the different surgical procedures for the overall mean EQ-5D index score at baseline, procedures related to benign or malignant tumors and elbow/hand diseases scored statistically significantly higher than average, which is important clinically, while patients with hip and spine procedures scored significantly lower than average.
Preoperatively, at baseline, the standardized EQ-5D index score (mean difference between the age- and sex-matched population) was –0.29. All 15 groups of patients had a lower EQ-5D index score than in the matched population (–0.09 to –0.53).
At the 12-month follow-up, the mean EQ-5D index score had increased statistically significantly by 0.18 units from baseline to 0.72 (). The mean EQ-5D in women increased almost to the level of that in men: 0.71 in comparison to 0.73. Patients younger than 30 years had a 12-month mean EQ-5D index score of 0.79 and patients older than 80 years had a 12-month mean score of 0.66.
Table 2. Details of the 2,444 patients in the study at 12 months postoperatively
Patients who underwent hip or knee arthroplasty, had complications after surgery, underwent other knee surgery, had trauma-related procedures, had rheumatoid arthritis or who underwent spine, hip, or infection-related surgery showed statistically significant improvements in mean EQ-5D index score (0.09 to 0.31). Patients with benign or malignant tumors or elbow/hand diseases showed no statistically significant changes in EQ-5D index score.
The standardized EQ-5D index score (mean difference between the age- and gender-matched population) at 12 months of follow-up was –0.11. Hip arthroplasty patients had a mean standardized EQ-5D index score preoperatively of –0.31 but their EQ-5D score improved and reached the level of that of the age- and sex-matched population (standardized EQ-5D index score of 0.00 at 12-month follow-up). Knee arthroplasty, trauma-related operations, other hip and knee surgery, rheumatoid arthritis surgery, surgery after complications, and spine surgery showed major improvements in EQ-5D index score 12 months after operation. However, they did not reach that of the matched population. The mean difference in score from that of the matched population postoperatively varied from –0.07 to –0.21.
One year after surgery, half of the patients experienced an improvement of > 0.1 in their EQ-5D index score and a small group (14 %) reported deterioration in their scores of > –0.1. 69% of the hip arthroplasty patients improved by at least 0.1 and only 6% deteriorated in their EQ-5D index score, in contrast to malignant tumor surgery where only 24% improved more than 0.1 and 30% deterioriated by > –0.1.
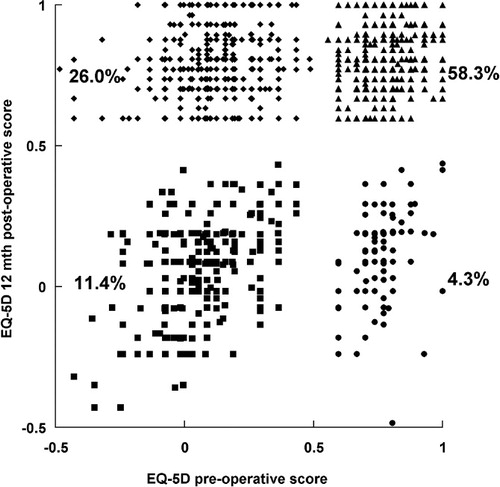
We found that the distribution of the EQ-5D index score was bimodal, and very few individuals scored around the average ( and ). Preoperatively, the EQ-5D index score had a bimodal distribution around 0.1 and 0.7. At 12 months, the distribution was still bimodal but most patients now had scores within the range 0.7–1.0. The pre-and postoperative EQ-5D index scores showed 4 major groups of patients (). The first group of patients (26%) had experienced great improvement, while a second group of patients with high preoperative scores (58%) had improved slightly. A third group with low EQ-5D scores preoperatively (12%) were unchanged, and a fourth small group (4%) perceived a decline in their HRQOL.
Figure 1. A. Bar chart showing preoperative health-related quality of life (EQ-5D) in the orthopedic cohort. Baseline EQ-5D index scores; n = 2,444. B. Bar chart showing postoperative health-related quality of life (EQ-5D) in the orthopedic cohort. 12-month follow-up EQ-5D index scores; n = 2,444.
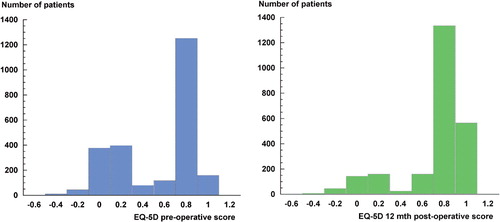
Figure 2. Graph showing health-related quality of life (EQ-5D) in an orthopedic cohort. Preoperative and 12-month postoperative EQ-5D index scores. The first group of patients (26%) had experienced a great improvement (diamonds); a second group of patients (58.3%) with high preoperative scores were slightly improved (triangles). A third group (11.4%) were unchanged, with low EQ-5D index scores (squares), and a fourth, small group (4.3%) had a decline in their scores (circles).
The mean response rate of those who completed the EQ-5D questionnaire at baseline was 85% (). The response rate varied considerably (59–100%), with the lowest response rates for patients with diabetes/infection (59%) and malignant tumors (68%).
Table 3. Total number of elective operations in the study at baseline and responder rate at baseline
In the dropout analyses (Appendix) we found that the responders were more likely to be women, to be older, or to have a low preoperative EQ-5D index score. The response rate also depended on the type of surgery. The responders were on average 5 years older than non-responders (p < 0.001). However, after adjustment for type of surgery this difference was reduced to 3 years, but it was still highly significant (p < 0.001). A comparison between gender and response rate showed that women had a higher response rate (unadjusted comparison, p = 0.0009). Adjustment of the association between gender and response rate for type of surgery reduced the association between gender and response rate (adjusted, p = 0.02). Similarly, after adjusting the difference in mean EQ-5D index score at baseline between responders and non-responders for type of surgery, the difference became less pronounced. On average, the responders had a lower score than non-responders by 0.05 units (p < 0.001). However, after adjustment for type of surgery, this difference was reduced to 0.03 units (p = 0.02).
Discussion
We found that most patients who were operated on for orthopedic conditions experienced an improved health-related quality of life and that their mean EQ-5D index score increased from 0.54 to 0.72 one year after surgery.
As expected, we noted large differences between surgical groups. In contrast to patients with tumor diseases, who scored high with a mean EQ-5D of 0.71, patients scheduled for hip or knee arthroplasty scored considerably lower (0.49 and 0.51, respectively). The indication for surgery is however, totally different in these cases, which must be kept in mind when interpreting these data. Notably, the group of patients treated with hip arthroplasty improved considerably and reached the scores of the age- and sex-matched reference population. Interestingly, patients with tumors improved in HRQOL to some extent in spite of their malignant conditions.
In a review evaluating changes after hip replacement, the results from all studies were consistent in showing beneficial and often dramatic improvements in HRQOL after elective procedures (Towheed and Hochberg Citation1996). Another review analyzing Short Form-36 and the Western Ontario and McMaster University osteoarthritis index after hip and knee arthroplasties showed similar results, and both procedures were found to be quite effective in terms of improvement in health-related quality-of-life dimensions (Ethgen et al. Citation2004). Surgery for lumbar spinal stenosis can give improvement in self-reported quality of life similar to that in hip and knee arthroplasty (Rampersaud Citation2008). A recently published study demonstrated that spinal surgery can return patients' HRQL to that of age-matched population norms and yield outcomes similar to those in hip and knee replacement patients (Mokhtar et al. Citation2010). As other authors have shown (Hansson et al. Citation2008, Anderson et al. Citation2009), our study confirms that patients who have undergone spine procedures improve in HRQOL as excellently as the arthroplasty patients do.
In a study evaluating patients with inflammatory arthritis using both EQ-5D and SF-6D health assessment questionnaires, the authors recommended the inclusion of at least one preference-based measure in future clinical studies (Harrison et al. Citation2010). We noticed in our study that inflammatory arthritis (rheumatoid arthritis (RA)) patients had a positive effect on HRCOL but the improvement was less than for patients treated with joint replacement. The reason for this could be that surgery had an effect on pain in the actual joint treated but less improvement in other dimensions of health (Osnes-Ringen Citation2009).
The minimal important difference (MID) is important for interpreting the impact of score changes, and is also an important measure for power calculations in studies (Walters and Brazier Citation2003). MID for EQ-5D index score has been reported by Walters and Brazier (Citation2005). For those subjects who reported some changes, a mean EQ-5D index score of 0.07 was found. In our orthopedic cohort, half of the patients had elevated EQ-5D index scores (by more than 0.1) after the operation. 14% had reduced EQ-5D index scores—by more than 0.1—one year after the operation, and one third had less changes (less than 0.1) in their EQ-5D index scores.
This first attempt to collect a whole sample of orthopedic conditions makes it possible to perform cost-utility analysis. A QALY is defined as 1 year in full health. Estimation of QALYs requires data on survival and the corresponding health state score, the health status reflecting the HRQOL of the individual, on a scale from 0 (dead) to 1 (full health) (Gold et al. Citation1996, Meunning and Gold Citation2001, Drummond et al. Citation2005). If utilities are multiplied by the amount of time spent in that particular health state, then they become QALYs. QALYs allow for varying times spent in different states by calculating an overall score for each patient. For the studies in which the follow-up is 1 year, the mean change in utility scores over the 1-year period can be directly interpreted as the MID for a QALY. QALYs may have the potential to influence public policy and decisions about resource allocation.
If baseline characteristics are controlled for the EQ-5D data, our findings could be used for comparison between hospitals. Comparison between provider units in different hospitals or between consultant specialities within a single institution can provide important information that might be applied for benchmarking or performance management.
In addition to clinical priority assessment, criteria in elective orthopedic surgery EQ-5D could be used (CitationNKO 2009). Patients with low scores have low autonomy and should be given high priority (Government 2003, CitationNKO 2009). We found that one third of all patients had a low preoperative HRQOL according to EQ-5D index score and two-thirds of them improved considerably. In future, “soft” HRQOL data (e.g. EQ-5D) might be included in the preoperative evaluation as well as more old-fashioned “hard” data such as radiology. However, to use the instrument in order to make priorities between groups of orthopedic surgical procedures seems to be more controversial, as the patients' individual EQ-5D index scores differed substantially.
The present study has several limitations. It is a prospective follow-up study of patients who underwent surgery, not a prospective randomized controlled trial comparing surgery to nonoperative treatment. However, most of the surgery performed involved accepted interventions (CitationNKO 2009). At baseline, we lost 15% of all patients scheduled for elective surgery. If not all patients are reached at baseline, the patients with the most severe symptoms could be left out and the results would be biased towards patients with less symptoms. However, the numbers of patients included and the response rates were high, apart from for the group of patients with diabetes/infection. For patients who were operated on for diabetes/infection, our results may therefore have been underestimated.
The department only mailed 1 follow-up questionnaire to the patients and no reminders, which led to a loss of more than 40% of those initially included in the study. In the dropout analysis, no major difference was found in the preoperative EQ-5D index scores between the responders and the non-responders. However, the responders tended to be women and to be older, causing our results to be a conservative interpretation. In this analysis, no information on patient co-morbidities or on other types of interfering conditions was collected. Thus, the study can be considered to represent a cross-section of orthopedic patients who undergo surgery at a university hospital.
We selected 1 year as a time outcome measurement because it was an easy endpoint. In some groups of patients (e.g. elderly), it might have been better to have had a shorter time frame because many other factors may have impaired the results.
The choice of algorithm used to convert self-classification scores can affect the index-based score, as shown in a study that compared UK and US scoring algorithms in patients undergoing percutaneous coronary intervention (PCI) (Shrive et al. Citation2007). However, while country-specific societal preferences may reduce the scope in comparing HRQoL estimates across studies from different countries, they are more helpful for local decision-making, especially when allocating resources within national healthcare programs.
The EQ-5D instrument has potential limitations. It may lack responsiveness to small but clinically important changes in health (Dawson et al. Citation2001). In the subgroups of patients who were operated on for elbow/hand, shoulder, and foot problems, we noted only minor health changes. The lack of minimal important differences (MID) for this group must be considered. It is also important to add condition-specific instruments in evaluating outcome after orthopedic surgery.
The bimodal distribution of EQ-5D scores that we found preoperatively and at the 12-month follow-up has also been reported by others (Conner-Spady et al. Citation2001, Xie et al. Citation2007). The EQ-5D algorithm tends to cluster scores in the upper extremity close to 1.0, and around 0.45. We strongly believe that it is the structure of the instrument that causes this phenomenon rather than the fact that it appears to highlight 2 subgroups of patients. This has also been noted in other studies (Rivero-Arias et al. Citation2005, Jansson et al. Citation2009).
We consider that our cohort represents patients in general who have undergone orthopedic surgery. This is the largest orthopedic cohort to be studied regarding HRQL so far, with 426 diagnoses and 446 orthopedic procedures. It could be questioned why we divided the cohort into 15 groups according to anatomical region and type of surgery, but it would have been difficult to present the results in any other way due to the large number of procedures. The drawback of this is that we lost the possibility of presenting details of specific diagnoses and procedures. We notice that our large cohort had a low HRQOL according to EQ-5D index score. A major strength in our report is that we matched our cohort with the Swedish EQ-5D reference population survey (Burström et al. Citation2001, Citation2003). We compared all patients older than 20 years of age and in spite of the finding that most patients felt an improved quality of life, the average preoperative EQ-5D index score of 0.54 is among the lowest reported in the literature so far. In the population survey (Burström et al. Citation2001) it was found that patients with low back pain scored 0.55, patients with stroke 0.43 and those with depression 0.38.
KÅJ designed the study, compiled and analyzed the data, and wrote the manuscript. FG participated in the analysis, and in writing and editing of the manuscript.
We are grateful for the information we received from Professor Gunnar Németh, former head of the Department of Orthopedic Surgery at Karolinska University Hospital, and to Eila Sterner and Kerstin Holmlund who helped with patient recruitment. Karl-Åke Jansson was funded in part by grants from Karolinska Institutet and the Department of Orthopedics at Karolinska University Hospital, Solna.
No competing interests declared.
- Akahane T, Shimizu T, Isobe K, Yoshimura Y, Fujioka F, Kato H. Evaluation of postoperative general quality of life for patients with osteosarcoma around the knee joint. J Pediatr Orthop B 2007; 16 (4):269-72.
- Anderson PA, Puschak TJ, Sasso RC. Comparison of short-term SF-36 results between total joint arthroplasty and cervical spine decompression and fusion or arthroplasty. Spine (Phila Pa 1976) 2009; 15: 34 (2): 176-83.
- Brooks, EuroQol Group. EuroQol. The current state of play. Health Policy 1996: 37: 53-72.
- Brooks R, Rabin R, de Charro F. The measurement and valuation of health status using EQ-5D: A European perspective. Evidence from the EuroQol BIOMED Research Programme. Dordrecht: Kluwer Academic Publishers 2003.
- Burström K, Johannesson M, Diderichsen F. Swedish population health-related quality of life results using the EQ-5D. Quality of Life Reserch 2001: 621-35.
- Burström K. Population Health and Inequalities in Health. Measurement of health - related quality of life and changes in QALYs over time in Sweden. Thesis Stockholm: ReproPrint AB 2003.
- Cockerill W, Lunt M, Silman AJ, Health-related quality of life and radiographic vertebral fracture. Osteoporos Int 2004; 15:113-9.
- Conner-Spady B, Cumming C, Nabholtz JM, Jacobs P, Stewart D. Responsiveness of the EuroQol in breast cancer patients undergoing high dose chemotherapy. Qual Life Res 2001; 10 (6):479-86.
- Dawson J, Fitzpatrick R, Frost S, Gundle R, McLardy-Smith P, Murray D. Evidence for the validity of a patient-based instrument for assessment of outcome after revision hip replacement. J Bone Joint Surg (Br) 2001; 83 (8):1125-9.
- Dolan P. Modeling valuations for EuroQol health status. Med Care 1997: 1095-108.
- Dolan P, Gudex C, Kind P, Williams A. The time-trade-off method: Results from a general population study. Health Econ 1996: 141-54.
- Drummond M, O´bien B, Stoddart G, Torrance G. Methods for the economic evaluation of health care programmes. 3rd edn. New York: Oxford University Press 2005.
- England & Wales - National Joint Registry 2009. Available from http://www-new.njrcentre.org.uk/njrcentre/Default.aspx.
- EQ-5D 2009: Available from http://www.euroqol.org/eq-5d/eq-5d-versions/eq-5d-languages/available-versions.html.
- Ethgen O, Bruyère O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg (Am) 2004; 86:963-74.
- EuroQol Group. EuroQol - A new facility for the measurement of health-related quality of life. Health Policy 1990: 199-208.
- Giannoudis PV, Harwood PJ, Kontakis G, Allami M, Macdonald D, Kay SP, Kind P. Long-term quality of life in trauma patients following the full spectrum of tibial injury (fasciotomy, closed fracture, grade IIIB/IIIC open fracture and amputation). Injury 2009; 40 (2):213-9.
- Gold M, Siegel J, Russel L, Weinstein M (Eds.) Cost-effectiveness in health and medicine. New York: Oxford University Press 1996.
- Government Bill. National Goals for Public Health. Stockholm: Elanders Gotab, Government Bill 2003/03:35. (In Swedish) 2002.
- Hansson T, Hansson E, Malchau H. Utility of spine surgery: a comparison of common elective orthopedic surgical procedures. Spine 2008; 33 (25):2819-30.
- Harrison MJ, Lunt M, Verstappen SM, Watson KD, Bansback NJ, Symmons DP. Exploring the validity of estimating EQ-5D and SF-6D utility values from the health assessment questionnaire in patients with inflammatory arthritis. Health Qual Life Outcomes. 2010; 11; 8:21.
- Hoffmann C, Gosheger G, Gebert C, Jürgens H, Winkelmann W. Functional results and quality of life after treatment of pelvic sarcomas involving the acetabulum. J Bone Joint Surg (Am) 2006; 88 (3):575-82.
- Jansson KA, Nemeth G, Granath F, Blomqvist P. Health-related quality of life in patients before and after surgery for a herniated lumbar disc. J Bone Joint Surg (Br) 2005; 7:959-64.
- Jansson KA, Németh G, Granath F, Jönsson B, Blomqvist P. Health-related quality of life (EQ-5D) before and one year after surgery for lumbar spinal stenosis. J Bone Joint Surg (Br) 2009; 91 (2):210-6.
- Kind P, Dolan P, Gudex C, Williams A. Variations in population health status: results from a United Kingdom national questionnaire survey. BMJ 1998; 316: 736-741.
- Kopec JA, Willison KD. A comparative review of four preference-weighted measures of health-related quality of life. J Clin Epidemiol 2003; 56:317-25.
- Löfvendahl S, Eckerlund I, Hansagi H, Resch S, Hanning M. Waiting for orthopaedic surgery: factors associated with waiting times and patients' opinion. Int J Qual Health Care 2005; 17 (2):133–40.
- Meunning P, Gold M. Using the years-of health-life measure to calculate QUALYs. Am J Prev Med 2001; 20: 35-9.
- Mokhtar SA, McCombe PF, Williamson OD, Morgan MK, White GJ, Sears WR. Health-related quality of life: a comparison of outcomes after lumbar fusion for degenerative spondylolisthesis with large joint replacement surgery and population norms. Spine J 2010; 10 (4):306-12.
- NKO. Swedish National Competence Centre for Musculoskeletal Disorders (NKO) 2009. Medical indications for orthopaedic procedures. Available from www.nko.se.
- Odenbring S, Wagner P, Atroshi I. Long-term outcomes of arthroscopic acromioplasty for chronic shoulder impingement syndrome: a prospective cohort study with a minimum of 12 years' follow-up. Arthroscopy 2008; 24 (10):1092-8.
- Osnes-Ringen H, Kvien TK, Henriksen JE, Mowinckel P, Dagfinrud H. Orthopaedic surgery in 255 patients with inflammatory arthropathies: longitudinal effects on pain, physical function and health-related quality of life. Ann Rheum Dis 2009; 68 (10):1596-601.
- Rampersaud YR, Ravi B, Lewis SJ, Stas V, Barron R, Davey R, Mahomed N. Assessment of health-related quality of life after surgical treatment of focal symptomatic spinal stenosis compared with osteoarthritis of the hip or knee. Spine J 2008; 8 (2):296-304.
- Rivero-Arias O, Campbell H, Surgical stabilisation of the spine compared with a programme of intensive rehabilitation for the management of patients with chronic low back pain: cost utility analysis based on a randomised controlled trial. BMJ 2005; 330: 1239.
- Räsänen P, Roine E, Sintonen H, Semberg-Konttinen V, Ryynänen OP, Roine R. Use of quality-adjusted life years for the estimation of effectiveness of health care: A systematic literature review. Int J Technol Assess Health Care 2006; 22 (2):235-41.
- Scende A, Williams A (Eds). Measuring self-reported population health: An international perspective based on the EQ-5D. Rotterdam: Euroqol Group 2004.
- Shrive FM, Ghali WA, Johnson JA, Donaldson CP, Manns BJ. Use of the U.S. and U.K. scoring algorithm for the EuroQol-5D in an economic. Evaluation of cardiac care. Med Care 2007; 45:269-73.
- Swedish Knee Arthroplasty Register 2009. Available from http://www.knee.nko.se/english/online/thePages/index.php.
- The Word Bank. Global Burden of Disease and Risk Factors ISBN-10:0-8213-6262-3. The Word Bank, Washington DC: Oxford University Press and the World Bank 2006.
- Tidermark J, Bergström G, Svensson O, Törnkvist H, Ponzer S. Responsiveness of the EuroQol (EQ 5-D) and the SF-36 in elderly patients with displaced femoral neck fractures. Qual Life Res 2003; 12 (8):1069-79.
- Towheed TE, Hochberg MC. Health-related quality of life after total hip replacement. Semin Arthritis Rheum 1996; 26 (1):483-91.
- Xie F, Li SC, Luo N, Lo NN, Yeo SJ, Yang KY, Fong KY, Thumboo J. Comparison of the EuroQol and short form 6D in Singapore multiethnic Asian knee osteoarthritis patients scheduled for total knee replacement. Arthritis Rheum 2007; 15: 57 (6): 1043-9.
- Walters SJ, Brazier JE. What is the relationship between the minimally important difference and health state utility values? The case of the SF-6D. Health Qual Life Outcomes 2003; 1:4.
- Walters SJ, Brazier JE (2005). Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res 2005;14:1523-32.
- WHO. Gaining Health. The European Strategy for Prevention and Control of Noncommunicable Diseases 2006. Report of the 56th Session of the WHO Europe Regional Committee for Europe, Copenhagen, 11-14 September. Available from http://www.euro.who.int/Document/RC56/edoc08.pdf.2006.
- Woolfe AD. The bone and joint decade 2000 –2010. Ann Rheum Dis 2000; 59:81–2.
- Woofle AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003; 81:646–56.