
Abstract
Background and purpose — To retain or to sacrifice the posterior cruciate ligament (PCL) in total knee arthroplasty (TKA) remains a matter of discussion. In this systematic review, we wanted to find differences in functional and clinical outcome between the 2 methods.
Methods — We conducted a systematic review and meta-analysis including all randomized controlled trials (RCTs) and quasi-RCTs that have compared PCL retention with PCL sacrifice in TKA with a minimum of 1-year follow-up. Primary outcome was range of motion. Secondary outcomes were knee pain and clinical scoring systems that were preferably validated. Quality of evidence was graded using the GRADE approach. All outcomes available for data pooling were used for meta-analysis.
Results — 20 studies involving 1,877 patients and 2,347 knees were included. In meta-analysis, the postoperative flexion angle had a mean difference of 2 degrees (95% CI: 0.23–4.0; p = 0.03) and the KSS functional score was 2.4 points higher in favor of PCL sacrifice (95% CI: 0.41–4.3; p = 0.02). There were no statistically significant differences regarding other measured clinical outcomes such as WOMAC, KSS pain, clinical and overall score, HSS score, SF-12, radiolucencies, femoro-tibial angle, and tibial slope. The quality of the studies varied considerably. Risk of bias in most studies was unclear; 5 were judged to have a low risk of bias and 5 to have a high risk of bias.
Interpretation — We found no clinically relevant differences between retention and sacrifice of the PCL in TKA, in terms of functional and clinical outcomes. The quality of the studies ranged from moderate to low. Based on the current evidence, no recommendation can be made as to whether to retain or to sacrifice the PCL.
There is an ongoing debate on whether to retain or to sacrifice the posterior cruciate ligament (PCL) during TKA surgery. Arguments for PCL retention are maintenance of natural knee motion and maintained stability (CitationMihalko and Krackow 1999, CitationLombardi et al. 2001). Furthermore, the PCL is believed to have different types of mechanoreceptors for proprioception and kinesthesia, so the PCL might give a better “sense” to the postoperative knee (CitationNelissen and Hogendoorn 2001, CitationSwanik et al. 2004). Retention of the PCL leads to the need for adequate balancing of the ligament; inadequate balancing (i.e. too tight or too loose) may lead to knee pain, deteriorated range of motion, and instability (CitationPagnano et al. 1998, CitationMost et al. 2003). On the other hand, sacrificing the PCL could be helpful in balancing knees with deformities or contractures. Another advantage of sacrificing the PCL is preventing paradoxal femoral rollback (CitationDennis et al. 2004). Femoro-tibial movement will then be dictated by the degree of congruency between the femur and the tibial insert (CitationWolterbeek et al. 2012). Sacrificing the PCL leads to an increase in the flexion gap and (to a lesser extent) an increase in the extension gap (CitationMihalko and Krackow 1999, CitationBaldini et al. 2004).
A Cochrane systematic review from 2005 could not indicate what treatment option (retention or sacrifice of the PCL) is best regarding functional, clinical, and radiological outcome parameters (CitationJacobs et al. 2005). An update of this review was published by us in 2013 and still showed no relevant differences between the 2 groups (CitationVerra et al. 2013).
Since that literature search, several new reports of randomized controlled trials (RCTs) comparing PCL retention with PCL sacrifice have been published, necessitating an update. We wanted to find differences in functional, clinical, and radiological outcome between PCL-retaining and PCL-sacrificing TKA in the current literature.
Methods
Literature search and study selection
We used the same study protocol as developed for our Cochrane systematic review and meta-analysis (CitationJacobs et al. 2005, CitationVerra et al. 2013). We conducted a sensitive search in order to retrieve all the literature available. In consultation with an experienced librarian of the medical library of Leiden University Medical Center (JS), we searched the following databases: Medline (via PubMed), the Cochrane Central Register of Controlled Trials, Embase, Web of Science, CINAHL, Academic Search Premier, Current Contents Connect, and Science Direct. All the databases were searched up to May 19, 2014 using a syntax adapted for each database (Supplementary Table 1). No restrictions or limits were formulated. A final check that no relevant articles were missed was carried out by screening the references from the articles and by performing citation tracking on the articles that were included.
Table 1. Characteristics of the 20 studies
Articles were selected in 2 steps. In the first step, only the title and abstract were screened. In the second step, articles that passed the first step were retrieved in full text and again evaluated against the inclusion and exclusion criteria. These criteria were as follows: (1) The intervention evaluated in the trials had to be primary TKA comparing PCL retention with sacrifice. (2) The indication for TKA had to be osteoarthritis. (3) Follow-up had to be at least 12 months. (4) Studies had to be RCTs or quasi-RCTs. Quasi-RCTs are studies using, for example, date of birth, patient identification numbers, or alternating sequences for randomization. 2 reviewers (WV and LB) independently selected the trials to be included in the review. Disagreements were resolved by consensus. When no consensus could be reached, a third reviewer (WJ) cast the decisive vote.
Data collection
An already developed and tested data extraction form was used to extract data from the studies included. Items collected were study design features, population data, statistical analysis techniques, intervention characteristics, and all the outcome parameters reported, including results. The primary outcome was range of motion (ROM), including flexion and extension angle separately. Secondary outcomes were knee pain (visual analog scale, Knee Society clinical pain sub-score), validated clinical scoring instruments (such as the Western Ontario and McMaster Universities osteoarthritis index (WOMAC), the knee osteoarthritis outcome scale (KOOS), and the Oxford knee score), other clinical questionnaire scores (such as the Knee Society score (KSS), the Hospital for Special Surgery score (HSS), etc.), radiological implant migration (preferably using radiostereometric analysis (RSA)), complication rate, and other radiological outcomes (such as rollback and radiolucencies). All data were entered into Review Manager version 5.2 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012).
The risk of bias (e.g. selection bias, performance bias, detection bias, attrition bias) was assessed for every study. The risk of selection bias was judged by assessing how the randomization sequence was generated and by assessing how the treatment allocation was concealed. Risk of performance and detection bias was judged by evaluating the methods for blinding of participants, personnel, and observers, as described in the studies. Risk of attrition bias was assessed by judging the completeness of the data, including the follow-up rate. The possible judgements that could be made were low risk of bias, high risk of bias, and unclear risk of bias.
The quality of the evidence was assessed using the GRADE approach (CitationAtkins et al. 2004). In this method for grading of quality, RCTs are considered to be high-quality evidence; however, this can be downgraded to moderate, low, or very low quality for several reasons. These reasons are study limitations (e.g. high risk of bias), inconsistent results, indirectness of evidence, imprecision, or publication bias. The Cochrane Collaboration recommends using this approach to grade the quality of studies in systematic reviews (Higgins and Green 2011).
Analysis
Statistical analyses were conducted using Review Manager version 5.2. Continuous data were entered as mean and standard deviation (SD), and dichotomous outcomes as number of events. Standard deviations were used when available. When not provided, standard deviations were imputed from comparable studies or from original scores (i.e. confidence intervals). Estimates are given with 95% confidence intervals (CIs) where relevant.
In the meta-analysis, if the studies (patients, interventions, outcomes) were regarded to be clinically homogeneous, heterogeneity was first assessed by visual inspection of the forest plots. Furthermore, we investigated heterogeneity using the I2 statistic and, if significant (p < 0.05 using the Q statistic), the source of heterogeneity was investigated by conducting a sensitivity analysis and considering additional clinical reasons for potential clinical heterogeneity. In the absence of significant heterogeneity, and given a sufficient number of trials included, results were combined using mean differences for continuous data and relative risk for dichotomous data. We used a random effects model for all analyses.
Results
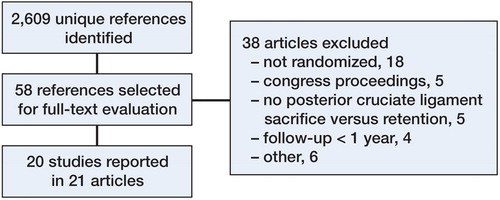
We identified 2,609 unique references. 58 articles were selected for further evaluation, resulting in 21 full-text papers that were used for analysis (, Table 2). The article by CitationVictor et al. (2005) described a population that was also part of the study population of CitationHarato et al. (2008). Data from both articles were used only once. The article from de CitationAndrade et al. (2009) was written in Portuguese and the article from CitationYansheng et al. (2013) was written in Chinese. The data were extracted by professional translators.
Figure 1. Flow chart of study selection showing the process of article selection and the reasons for articles being excluded.
Study characteristics
The 20 studies involved 1,877 patients and 2,347 knees. In 17 studies, the comparison between the 2 arms was PCL retention with a cruciate-retaining design versus PCL sacrifice using a posterior-stabilized design. In 3 studies, the same (cruciate-retaining) TKA design was used for both groups. One study used all three treatments (i.e. cruciate-retaining design with ligament retention and with ligament sacrifice and posterior-stabilized design (Table 2).
All studies used a clinical rating scale, either validated (e.g. WOMAC) or unvalidated (e.g. Knee Society score) and reported ROM or flexion measurements. There was very little use of radiostereometric analysis (RSA).
Risk of bias and quality of evidence
5 of the 20 studies included were assessed as having a low risk of bias, 5 of them were assessed as having a high risk of bias, and 10 had an unclear risk of bias.
5 articles described how the randomization sequence for the study was generated (CitationMisra et al. 2003, CitationChaudhary et al. 2008, CitationHarato et al. 2008, CitationRoh et al. 2013, CitationThomsen et al. 2013). The method of concealment of allocation was reported in 6 studies (CitationChaudhary et al. 2008, CitationHarato et al. 2008, CitationKim et al. 2009, CitationSeon et al. 2011, CitationMatsumoto et al. 2012, CitationThomsen et al. 2013). 3 studies used quasi-randomization: CitationAglietti et al. (2005) based choice of treatment on odd/even patient identification numbers, CitationMaruyama et al. (2004) used alternating sequences, and CitationWang et al. (2004) based the treatment on time of hospital admission. Blinding of the outcome assessor was reported in 10 studies (CitationTanzer et al. 2002, CitationMisra et al. 2003, CitationStraw et al. 2003, CitationAglietti et al. 2005, CitationChaudhary et al. 2008, de CitationAndrade et al. 2009, KiCitationm et al. 2009, CitationSeon et al. 2011, CitationMatsumoto et al. 2012, CitationThomsen et al. 2013). CitationSeon et al. (2011) reported explicitly that no blinding was used.
Studies reporting on the primary outcome of knee flexion were graded according to the GRADE approach. These studies were generally assessed as being of low quality. Quality was downgraded due to the high proportion of studies with an unclear risk of bias and the presence of studies rated with a high risk of bias. Also, studies reporting on the secondary outcomes were graded as being of moderate to low quality.
Meta-analysis
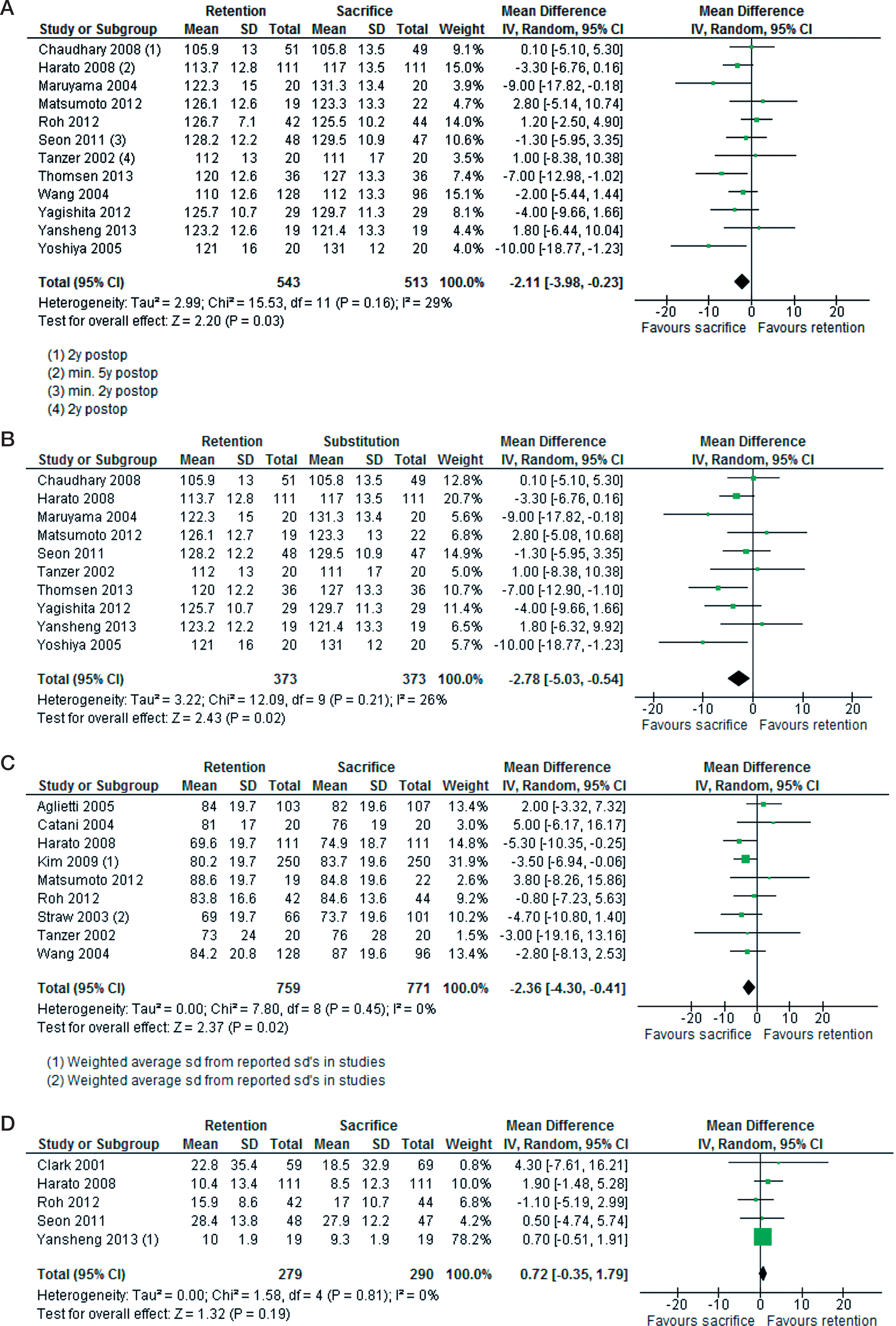
There was low quality of evidence from 12 studies (1,056 knees) that sacrifice of the PCL results in a better flexion angle, with a mean difference of 2 degrees (95% CI: 0.23–4.0; p = 0.03). This is a homogeneous result (I2 = 29%, p = 0.2). Furthermore, there was low quality of evidence from 9 studies (1,530 knees) that sacrifice of the PCL results in a higher Knee Society functional score of 2.4 points (95% CI: 0.41–4.3; p = 0.02) (). These were the only homogeneous and statistically significant differences between PCL retention and sacrifice. The WOMAC score was used in 5 studies; there was a 0.72-point difference between both groups (95% CI: –0.35 to 1.8; p = 0.19) in favor of PCL sacrifice. No other validated scoring systems were available for meta-analysis. Meta-analyses on the outcomes KSS pain, KSS clinical score, KSS overall score, HSS score, SF-12 mental, radiolucent lines, femoro-tibial angle, and tibial slope showed no statistically significant differences and they were comparable in terms of statistical homogeneity.
Figure 2. Forest plots from meta-analysis. A. Knee flexion from all PCL-sacrificing and PCL-retaining TKAs. Shows homogeneous results favoring PCL sacrifice with 2.1 degrees better flexion angle. B. Knee flexion from PCL-retaining TKA design versus posterior-stabilized TKA design. Shows homogeneous results favoring PCL sacrifice, with 2.8-degrees better flexion angle. C. Knee Society functional score from all PCL-sacrificing and PCL retaining TKAs. Shows homogeneous results favoring PCL sacrifice, with 2.4 more points in mean difference. D. WOMAC score from all PCL-sacrificing and PCL-retaining TKAs. Shows homogeneous results without any significant differences (0.78 points favoring PCL retention).
Sub-analysis of outcomes of low-quality studies comparing PCL retention with sacrifice using the same PCL-retaining TKA design in both groups showed no significant differences. Comparison of knee flexion in PCL retention with the PCL-sacrificing posterior-stabilizing design in 10 studies of moderate quality (746 knees) showed a mean difference of 2.8 degrees in favor of posterior stabilization (95% CI: 0.54–5.0; p = 0.02).
Complications were reported in 13 studies, and they ranged from anterior knee pain and femoral notching to deep infection ()
Table 3. Complications reported in the studies selected
Discussion
In this study of the current literature comparing PCL retention with PCL sacrifice in TKA, we did not find any clinically relevant differences between the groups. An extensive report on this topic, covering 17 studies, was published by our group in 2013 within the Cochrane Library of Systematic Reviews (CitationVerra et al. 2013). The newly added studies have not given any new evidence on this topic.
The 20 studies selected are the best available evidence to date for evaluation of the difference between PCL retention and PCL sacrifice in TKA. The assessment of the quality of the evidence showed that it was low to moderate. Incompleteness of reporting issues such as failure to explain randomization methods and blinding raises the likelihood of bias in the studies, resulting in lower grades of quality of evidence. However, we see an improving trend in reporting, as the more recent publications were generally assessed as having a lower risk of bias.
Despite the fact that RCTs are known to provide the least biased evidence, they are not suited for all outcomes. Survival analysis of the TKA cannot easily be investigated in RCTs because of the relatively short follow-up period and relatively small number of patients. In addition, classical survival analysis can be biased by competing risks, which should be accounted for for valid interpretation of outcome (CitationKeurentjes et al. 2012, CitationNouta et al. 2014). Observational, long-term follow-up cohort studies are valuable alternatives. Survivorship analyses of large cohorts showed a 10-year and 15-year survival of 91% and 90% in the PCL-retaining group and 76% and 75% in the PCL-sacrificing, posterior-stabilized group (CitationRand et al. 2003, CitationAbdel et al. 2011). However, other factors could influence these results, such as differences in TKA design or in materials in PCL-retaining and -stabilizing components (CitationEngh 2011). A minimum dataset for cohort studies has been advocated by the AQUILA consortium (CitationPijls et al. 2011).
Our study had several strengths. We used a sensitive search in 8 relevant databases with no language limitations. We also checked references and used citation tracking. Recently published have meta-analyses found and included only between 8 and 12 articles as compared to our 21 (CitationLuo et al. 2012, CitationBercik et al. 2013, CitationLi et al. 2014), while we excluded several RCTs because of the follow-up being less than 1 year (CitationSwanik et al. 2004, CitationIshii et al. 2008, CitationNishizawa et al. 2013, CitationCankaya et al. 2014). Since our study was performed according to the Cochrane guidelines, an elaborate and systematic assessment of quality of evidence and risk of bias was performed. In the meta-analysis, we separately compared the subgroups PCL sacrifice using a PCL-retaining design and PCL sacrifice using a posterior-stabilized design against PCL retention.
One limitation was the lack of high-quality evidence in several articles. Furthermore, we could not present information on outcome measures such as patient experience and satisfaction, gait analysis, micromotion of the components (by RSA), and kinematic outcome measures such as antero-posterior stability and contact position. The importance of the predictive value of RSA and survival in TKA has been analyzed extensively (CitationNelissen et al. 2011, CitationPijls et al. 2012).
Future research on the question of PCL retention or sacrifice in TKA should consist of RCTs that have identical follow-up times, that include long(er)-term follow-up in their protocols, and that add outcome measures such as gait analysis, patient experience, and patient satisfaction. In addition to this, recently developed outcome measures such as the “forgotten joint score” can be used (CitationBehrend et al. 2012). To study long-term TKA survival or complications, large observational studies are needed, focusing on retention or sacrifice of the PCL. Moreover, reporting in future studies must be more complete when describing study methods in order to reduce the likelihood of bias, and authors should also mention important confounders regarding outcome such as preoperative ROM measurements.
In conclusion, based on this systematic review and meta-analysis of all currently published RCTs, there are no clinically relevant differences between retention and sacrifice of the PCL in terms of clinical, functional, and radiological outcome.
IORT_A_973329_SM5037.pdf
Download PDF (28.1 KB)WCV: literature search, selection of articles, and writing of the manuscript. LGHvdB and WCHJ: selection of articles and revision of the manuscript. JWS: literature search. ABW and RGHHN: revision of the manuscript.
No competing interests declared.
Research was funded by Sanquin Blood Bank, the Netherlands and the Dutch Rheumatology Association (LRR grant).
- Abdel MP, Morrey ME, Jensen MR, Morrey BF. Increased long-term survival of posterior cruciate-retaining versus posterior cruciate-stabilizing total knee replacements. J Bone Joint Surg Am 2011; 93: 2072-8.
- Aglietti P, Baldini A, Buzzi R, Lup D, de Lapo L. Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: a prospective randomized study. J Arthroplasty 2005; 20: 145-53.
- Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ 2004; 328: 1490
- Baldini A, Scuderi GR, Aglietti P, Chalnick D, Insall JN. Flexion-extension gap changes during total knee arthroplasty: effect of posterior cruciate ligament and posterior osteophytes removal. J Knee Surg 2004; 17: 69-72.
- Behrend H, Giesinger K, Giesinger JM, Kuster MS. The “forgotten joint” as the ultimate goal in joint arthroplasty: validation of a new patient-reported outcome measure. J Arthroplasty 2012; 27(3): 430-6.
- Bercik MJ, Joshi A, Parvizi J. Posterior cruciate-retaining versus posterior stabilized total knee arthroplasty: a meta-analysis. J Arthroplasty 2013; 28(3): 439-44.
- Cankaya D, Ozkurt B, Aydin C, Tabak AY. No difference in blood loss between posterior cruciate ligament retaining and posterior cruciate ligament stabilized total knee arthroplasties. Knee Surg Sport Tramatol Arthrosc 2014; 22(8): 1865-9.
- Catani F, Leardini A, Ensini A, Cucca G, Bragonzoni L, Toksvig-Larsen S, Giannini S. The stability of the cemented tibial component of total knee arthroplasty: posterior cruciate-retaining versus posterior-stabilized design. J Arthroplasty 2004; 19: 775-82.
- Chaudhary R, Beaupre LA, Johnston DW. Knee range of motion during the first two years after use of posterior cruciate-stabilizing or posterior cruciate-retaining total knee prostheses. A randomized clinical trial. J Bone Joint Surg Am 2008; 90: 2579-86.
- Clark CR, Rorabeck CH, MacDonald S, MacDonald D, Swafford J, Cleland D. Posterior-stabilized and cruciate-retaining total knee replacement: a randomized study. Clin Orthop Relat Res 2001; (392): 208-12.
- de Andrade M AP, Honorio de Carvalho Jr L, Goncalves M BJ, de Castro C AC, and Frontes B PC. Clinical evaluation of total knee arthroplasties with posterior cruciate ligament retain and sacrifice. Rev Brasil de Med 2009; 66: 48-51.
- Dennis DA, Komistek RD, Mahfouz MR, Walker SA, Tucker A. A multicenter analysis of axial femorotibial rotation after total knee arthroplasty. Clin Orthop Relat Res 2004; 428(11): 180-9.
- Engh GA. Is long-term survivorship really significantly better with cruciate-retaining total knee implants?: Commentary on an article by Abdel et al.: “Increased long-term survival of posterior cruciate-retaining versus posterior cruciate-stabilizing total knee replacements”. J Bone Joint Surg Am 2011; 93: e136-2
- Harato K, Bourne RB, Victor J, Snyder M, Hart J, Ries MD. Midterm comparison of posterior cruciate-retaining versus -substituting total knee arthroplasty using the Genesis II prosthesis. A multicenter prospective randomized clinical trial. Knee 2008; 15: 217-21.
- Higgins J P T, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org
- Ishii Y, Noguchi H, Matsuda Y, Takeda M, Kiga H, Toyabe S. Range of motion during the peri-operative period in total knee arthroplasty. Arch Orthop Trauma Surg 2008; 128: 795-9.
- Jacobs WC, Clement DJ, Wymenga AB. Retention versus sacrifice of the posterior cruciate ligament in total knee replacement for treatment of osteoarthritis and rheumatoid arthritis. Cochrane Database Syst Rev 2005; 4: CD004803.
- Keurentjes JC, Fiocco M, Schreurs BW, Pijls BG, Nouta KA, Nelissen RG. Revision surgery is overestimated in hip replacement. Bone Joint Res 2012; 1(10): 258-62.
- Kim YH, Choi Y, Kwon OR, Kim JS. Functional outcome and range of motion of high-flexion posterior cruciate-retaining and high-flexion posterior cruciate-substituting total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am 2009; 91: 753-60.
- Li N, Tan Y, Deng Y, Chen L. Posterior cruciate-retaining versus posterior stabilized total knee arthroplasty: a meta-analysis of randomized controlled trials. Knee Surg Sports Traumatol Arthrosc 2014; 22(3): 556-64.
- Lombardi AV, Mallory TH, Fada RA, Hartman JF, Capps SG, Kefauver CA, Adams JB. An algorithm for the posterior cruciate ligament in total knee arthroplasty. Clin Orthop Relat Res 2001; (392): 75-87.
- Luo SX, Zhao JM, Su W, Li XF, Dong GF. Posterior cruciate substituting versus posterior cruciate retaining total knee arthroplasty prostheses: a meta-analysis. Knee 2012; 19(4): 246-52.
- Maruyama S, Yoshiya S, Matsui N, Kuroda R, Kurosaka M. Functional comparison of posterior cruciate-retaining versus posterior stabilized total knee arthroplasty. J Arthroplasty 2004; 19: 349-53.
- Matsumoto T, Muratsu H, Kubo S, Matsushita T, Kurosaka M, Kuroda R. Intraoperative soft tissue balance reflects minimum 5-year midterm outcomes in cruciate-retaining and posterior stabilized total knee arthroplasty. J Arthroplasty 2012; 27(9): 1723-30.
- Mihalko WM, Krackow KA. Posterior cruciate ligament effects on the flexion space in total knee arthroplasty. Clin Orthop Relat Res 1999; (360): 243-50.
- Misra AN, Hussain MR, Fiddian NJ, Newton G. The role of the posterior cruciate ligament in total knee replacement. J Bone Joint Surg Br 2003; 85: 389-92.
- Most E, Zayontz S, Li G, Otterberg E, Sabbag K, Rubash HE. Femoral rollback after cruciate-retaining and stabilizing total knee arthroplasty. Clin Orthop Relat Res 2003; (410): 101-13.
- Nelissen RG, Hogendoorn PC. Retain or sacrifice the posterior cruciate ligament in total knee arthroplasty? A histopathological study of the cruciate ligament in osteoarthritic and rheumatoid disease. J Clin Pathol 2001; 54: 381-4.
- Nelissen RG, Pijls BG, Kärrholm J, Malchau H, Nieuwenhuijse MJ, Valstar ER. RSA and registries: the quest for phased introduction of new implants. J Bone Joint Surg Am 2011; 93 suppl 3: 62-5.
- Nouta KA, Pijls BG, Fiocco M, Keurentjes JC, Nelissen RG. How to deal with lost to follow-up in total knee arthroplasty: a new method based on competing risks approach. Int Orthop 2014; 38(5): 953-9.
- Nishizawa Y, Matsumoto T, Kubo S, et al. The influence of patella height on soft tissue balance in cruciate-retaining and posterior-stabilised total knee arthroplasty. Int Orthop 2013; 37: 421-5.
- Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ. Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop Relat Res 1998; (356): 39-46.
- Pijls BG, Dekkers OM, Middeldorp S, Valstar ER, van der Heide HJ, van der Linden HM, Nelissen RG. AQUILA: assessment of quality in lower limb arhtroplasty. An expert Delphi consensus for total knee and hip arthroplasty. BMC Musculoskelet Disord 2011; 12: 173.
- Pijls BG, Valstar ER, Nouta KA, Plevier JW, Fiocco M, Middeldorp S, Nelissen RG. Early migration of tibial components is associated with late revision: a systematic review and meta-analysis of 21,000 knee arthroplasties. Acta Orthop 2012: 83(6): 614-24.
- Rand JA, Trousdale RT, Ilstrup DM, Harmsen WS. Factors affecting the durability of primary total knee prostheses. J Bone Joint Surg Am 2003; 85-A: 259-65.
- Roh YW, Jang J, Choi WC, et al. Preservation of the posterior cruciate ligament is not helpful in highly conforming mobile-bearing total knee arthroplasty: a randomized controlled study Knee Surg Traumatol Arthroscop. 2013; 21 (12): 2850-9.
- Seon JK, Park JK, Shin YJ, Seo HY , Lee KB, Song EK. Comparisons of kinematics and range of motion in high-flexion total knee arthroplasty: cruciate retaining vs. substituting designs. Knee Surg Sports Traumatol Arthrosc 2011; 19: 2016-22.
- Shoji H, Wolf A, Packard S, Yoshino S. Cruciate retained and excised total knee arthroplasty. A comparative study in patients with bilateral total knee arthroplasty. Clin Orthop Relat Res 1994; (305): 218-22.
- Straw R, Kulkarni S, Attfield S, Wilton TJ. Posterior cruciate ligament at total knee replacement. Essential, beneficial or a hindrance? J Bone Joint Surg Br 2003; 85: 671-4.
- Swanik CB, Lephart SM, Rubash HE. Proprioception, kinesthesia, and balance after total knee arthroplasty with cruciate-retaining and posterior stabilized prostheses. J Bone Joint Surg Am 2004; 86-A: 328-34.
- Tanzer M, Smith K, Burnett S. Posterior-stabilized versus cruciate-retaining total knee arthroplasty: balancing the gap. J Arthroplasty 2002; 17: 813-9.
- Thomsen MG, Husted H, Otte KS, Holm G, Troelsen A. Do patients care about higher flexion in total knee arthroplasty? A randomized controlled double-blinded trial. BMC Musc Skeletal Dis 2013; 14: 127.
- Verra WC, van den Boom LG, Jacobs WC, Clement DJ, Wymenga AA, Nelissen RG. Retention versus sacrifice of the posterior cruciate ligament in total knee arthroplasty for treating osteoarthritis. Cochrane Database Syst Rev 2013; 10: CD004803.
- Victor J, Banks S, Bellemans J. Kinematics of posterior cruciate ligament-retaining and -substituting total knee arthroplasty: a prospective randomised outcome study. J Bone Joint Surg Br 2005; 87: 646-55.
- Wang CJ, Wang JW, Chen HS. Comparing cruciate-retaining total knee arthroplasty and cruciate-substituting total knee arthroplasty: a prospective clinical study. Chang Gung Med J 2004; 27: 578-85.
- Wolterbeek N, Garling EH, Mertens BJ, van der Linden HM, Nelissen RG, Valstar ER. Kinematics of a highly congruent mobile-bearing total knee prosthesis. Knee Surg Sport Traumatol Arthrosc 2012; 20(12): 2487-93.
- Yagishita K, Muneta T, Ju YJ, Morito T, Yamazaki J, Sekiya I. High-flex posterior cruciate-retaining vs posterior cruciate-substituting designs in simultaneous bilateral total knee arthroplasty: a prospective, randomized study. J Arthroplasty 2012; 27: 368-74.
- Yansheng WU, Yongsheng LI, Baicheng CH. Effect of posterior cruciate ligament retaining or not on knee joint proprioception. Chinese J Reperative and Reconstructive Surg 2013; V27: 7.
- Yoshiya S, Matsui N, Komistek RD, Dennis DA, Mahfouz M, Kurosaka M. In vivo kinematic comparison of posterior cruciate-retaining and posterior stabilized total knee arthroplasties under passive weight-bearing conditions. J Arthroplasty 2005; 20(6): 777-83.