
Abstract
Based on a case of suspected ischemic heart disease we review hiatal hernia causing chest pain. Rest echocardiography images were suggestive of cardiac mass in the left atrium. Dobutamine stress echocardiogram was negative for inducible ischemia. Multi-slice computed tomography of the chest was performed showing that a large hiatal hernia was present compressing on the left atrium. Multimodality imaging is necessary for suspected mass compressing the heart, causing chest discomfort.
Introduction
Patients with hiatal hernia (HH) compressing the left atrium, mimicking a left atrial mass have been previously presented in the literature (Citation1). HH has been a challenging diagnosis in the suspicion of chest discomfort and echocardiography images can often be misleading (Citation2). Magnetic resonance imaging (MRI) or multi-slice computed tomography (MSCT) should be performed to establish diagnosis.
Patient
This case is based on a 72-year-old patient referred for ischemic heart disease assessment. Two-dimensional transthoracic echocardiogram and dobutamine stress echocardiogram were performed. Stress echocardiogram was negative for inducible ischemia. Transthoracic echocardiogram showed no signs of structural or functional abnormalities of the left or the right ventricle. However, on the posterior and inferior aspect of the left atrium a mass appeared to be present (). Non-contrast chest MSCT was performed to further clarify diagnosis. In MSCT images the heart appeared normal in size and no pericardial effusion was noted. The thoracic aorta and main pulmonary arteries were normal size. A large HH was present compressing the heart, especially on the left atrium ().
Figure 1. Two-dimensional transthoracic echocardiography image. Four-chamber apical view indicative of mass in the left atrium (white arrow).
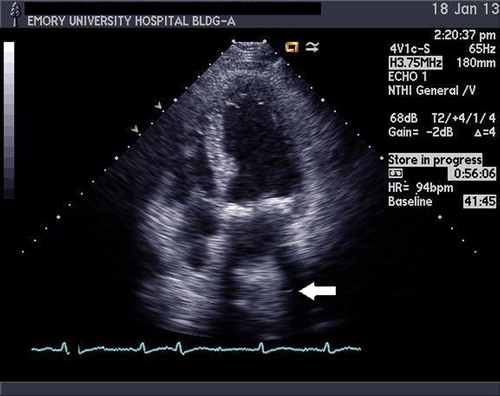
Figure 2. Chest computed tomography axial plane image showing a large hiatal hernia compressing the heart, especially on the left atrium (white arrow).
Only few instances of cardiac compression causing clinical symptoms have been reported when larger hernias occur, usually in elderly patients who may present with syncope (‘swallow syncope’ syndrome). Dynamic electrocardiographic changes due to cardiac compression and clinical presentation of syncope have been documented (Citation3). HH can mislead to the diagnosis of myocardial ischemia in cardiac nuclear imaging (Citation4).
MSCT scanning of the abdomen and thorax is useful, safe and reliable in detection of the HH and its associated complications. Electrocardiogram-gated chest MSCT and cardiac MSCT are useful in the evaluation of chest pain and provide additional information for extra-cardiac findings such as HH (Citation5). Multi-planar MRI is another important tool for HH assessment, MRI can clearly indicate the normal diaphragm as a linear structure and the hernial orifice as a diaphragmatic discontinuity.
Conclusions
HH constitutes a form of posterior mediastinal mass that can compress on the posterior aspects of the heart. It may cause chest discomfort, shortness of breath, syncope or mimic ischemic heart syndromes. During echocardiography HH can be misdiagnosed as intra-cardiac mass and further imaging with MSCT or MRI should be considered.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Lim HS, Leong DP, Alasady M. Massive hiatus hernia mimicking a left atrial mass. Heart Lung Circ. 2013; (Epub ahead of print).
- Alam M. Pitfalls in the echocardiographic diagnosis of intracardiac and extracardiac masses. Echocardiography 1993;2:181–91.
- Karamitsos TD, Arnold JR, Rider OJ, Francis JM, Ferrett C, Neubauer S, et al. Massive hiatus hernia impeding transeosophageal echocardiography in a patient with swallow-syncope syndrome. Hellenic J Cardiol. 2009;50:216–17.
- Ortín J, Fuster D, Muxí A, Setoain X, Paredes P, Duch J, et al. Misleading diagnosis of ischemia by Tc-99m tetrofosmin SPECT resulting from a voluminous hiatal hernia. Clin Nucl Med. 2006;9:581–3.
- Bierry G, Roy C, Buy X, Kellner F, Jiassi H, Gangi A. ECG-gated chest CT angiography: Value for atypical chest pain evaluation. J Radiol. 2009;1:825–31.