Abstract
Our objective was to propose a testable hypothesis arising from the recent finding of a low index-to-ring finger ratio (2D:4D ratio) in ALS. The 2D:4D ratio finding suggests that prenatal testosterone exposure may play a role in the development of the disease. Research from other fields is presented to suggest that healthy individuals with low 2D:4D ratio have enhanced sporting prowess, particularly with regard to activities requiring endurance and dependent upon slow-twitch muscles. Although studies are of varying quality, some epidemiological findings in ALS also suggest enhanced sporting prowess, as well as a higher risk of developing the disease among members of certain physically active professions. If the 2D:4D finding survives replication then this might explain the reported elevated risk of ALS among professional athletes, the military, and manual professions. Such a relationship might also explain why ALS patients were more likely to have been elite sportspeople in younger life. This hypothesis may serve as a starting point for debate and discussion over the nature of ALS risk factors, as well as generating a number of specific testable hypotheses that may yield insight into the genesis of the disease.
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease that causes weakness, atrophy, and eventually death (Citation1).
The cause of sporadic forms of ALS is unknown, but is frequently held to be some combination of genetic background risk combined with environmental exposure or ‘trigger’; one theory is that common polymorphisms present in the general population each exert small effects on the likelihood of developing ALS (Citation2). However, the environmental triggers for ALS have continued to remain elusive. Apart from a small number of clusters around the Western Pacific, the incidence rates of ALS are relatively consistent worldwide (Citation1), suggesting that broad population-level environmental exposures (such as diet, radiation or groundwater contamination) are unlikely to be identified. In the modern world, occupation strongly influences exposure to potential harms, as has been identified in relation to lung cancer and leukemia resulting from exposure to asbestos and radiation, respectively (Citation3), or erethism found in 19th century milliners resulting from mercury toxicity (Citation4).
A number of studies have explored occupation as a risk factor for the development of ALS, but have identified no obvious common exposure, for instance to chemicals or electromagnetic fields. A recent systematic review of the literature found that people who later develop ALS were more likely than healthy controls to have been employed as farmers, electrical workers, carpenters, soccer players, or military personnel (Citation5). Clearly, these occupations have a number of putative exposures in common such as chemicals (e.g. pesticides), physical exertion (e.g. training), or trauma (e.g. injuries), and so there is still an absence of explanatory theory for these findings. Due to methodological inconsistencies in the literature it is also not possible to perform a true meta-analysis of studies performed to date, and due to low numbers of cases in a given profession and referral bias, even these systematically collected results must be weighed with caution.
Vivekananda et al. recently described an investigation of consecutive patients at a specialist ALS clinic who had their hands photographed and measured to establish the ratio of the lengths of their second and fourth fingers (index and ring fingers, known as the 2D:4D ratio) (Citation6). The 2D:4D ratio is sexually dimorphic, a feature recognized for more than a century (Citation7). Recent interest was stimulated by suggestions that 2D:4D ratio is influenced by higher levels of fetal exposure to testosterone (Citation7), and a number of studies have sought to explore whether 2D:4D might serve as a proxy measure of sex-linked traits or behaviors. Lower 2D:4D ratios are associated with higher levels of athletic ability, for instance (Citation8). Attempts to understand this relationship have established that this is not merely the result of psychological variables such as achievement, social potency, low harm avoidance, control, practice effects, or cognitive variables such as visuo-spatial skills (Citation9). In terms of magnitude, 2D:4D ratio is as independently predictive of performance as the number of years an individual has been practicing a sport (Citation9), and accounts for 25% of the variance in endurance running (Citation10). The mechanism is unclear but may be related to physical composition such as cardiovascular efficiency, aerobic capacity or the ratio of fast-twitch to slow-twitch muscle fibers and is particularly relevant to endurance running (distances greater than 1 kilometre) (Citation10).
Physical exercise has long been considered relevant to the etiology of ALS, although the quality of evidence is generally not robust (Citation11,Citation12). For example, Scarmeas et al. found that in their youth, individuals who went on to develop ALS were more likely than matched controls to be slim, and to excel at athletics (Citation13); the authors suggested “being slim and athletic might be a phenotypic expression of genetic susceptibility to ALS, mediated by some environmental agent”. However, Armon argues that this finding may result from referral bias of more educated, driven individuals seeking treatment from a respected ALS center (Citation14).
An eloquent study taking advantage of military service records in Sweden found that individuals who went on to develop ALS had a much better profile of physical fitness per kilogram of body weight at age 18 years (Citation15). The authors proposed a hypothesis that “this at-risk phenotype is characterized by relatively more type 1 muscle fibers (slow-twitch fibers)”. A recent population based case-control study also suggests a link between physical exercise and ALS (Citation16). It has been widely reported in the scientific press and media that ALS is elevated among Italian soccer players (Citation17). However, both the link between exercise and, in particular, Italian soccer players, has been refuted by others (Citation14,Citation18) on the basis of low expected case numbers in the comparison populations used. If physical activity were a significant factor, Harwood et al. propose a number of biological mechanisms that may be relevant but which pre-dated the 2D:4D finding (Citation19).
Hypothesis and studies arising
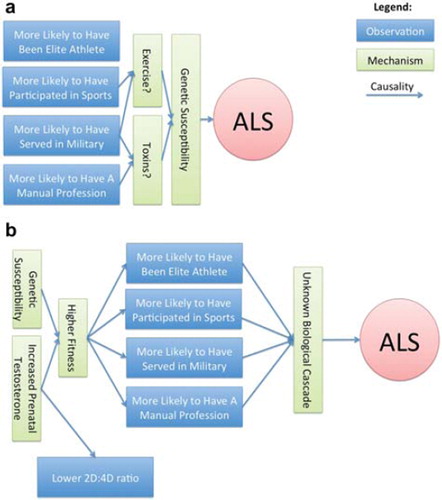
Rather than viewing occupation as increasing risk for exposure to toxins or trauma, we propose instead that there is (and always has been) something unusual about the way that people who will go on to be diagnosed with ALS developed physically in early life, which causes them to have traits that contribute to better athletic performance (see ). These traits may have made them the type of people who can gain entry to, and do well in, high-performance sports or physically intensive professions. Clearly it would be an error to over-generalize this theory, but it may provide a number of research avenues to identify statistical trends or association. The theory generates a number of testable hypotheses:
Figure 1. Two alternative schemas for causal mechanisms underlying the development of ALS. (a) The commonly held paradigm. (b) A prenatal-testosterone exposure paradigm.
Re-analyzing existing data by levels of physical exertion required for different careers would test the hypothesis that those occupations with, on average, a higher physical exertional burden or barrier to entry (e.g. firefighter) than those with a lower burden (e.g. accountant), are those with the highest relative risk ratios of developing ALS. Null hypothesis: there is no significant relationship between physical exertion of occupation and risk of developing ALS.
Using electromyography, the ratio of fast-twitch and slow-twitch muscles in ALS patients can be compared relative to healthy controls and other patients with neurodegenerative or neuromuscular diseases. Null hypothesis: ALS patients have the same ratio of slow-twitch to fast-twitch muscles as healthy controls and neuromuscular controls.
An unexplained characteristic of ALS is a decreased risk of cardiovascular disease among patients and their immediate relatives (Citation20). Speculatively, this could be linked to testosterone's beneficial effect on the cardiovascular system (Citation21). Null hypothesis: there is no significant relationship between cardiovascular disease and markers of testosterone (such as 2D:4D ratio) in PALS or their family members.
Within a family, the sibling that went on to develop ALS may have had higher levels of prenatal testosterone exposure and so have a higher 2D:4D ratio than their siblings. Null hypothesis: the 2D:4D ratio of patients is, on average, no different from their unaffected siblings.
Related to the above, there may be other testosterone-related phenotypic characteristics such as perceived attractiveness, muscle mass, or personality traits in siblings that went on to develop ALS which differ from their same-sex siblings who did not go on to develop ALS. Null hypothesis: male siblings who went on to develop ALS do not differ from unaffected male siblings in characteristics thought to be related to testosterone exposure.
Where new data are to be collected concerning occupational risk factors, these should include objective 2D:4D measurement and, ideally, other biological markers of testosterone metabolism. It is unclear to what extent these hypotheses will be valid in males compared to females. Methodologically, it may be simpler to consider only males as their hormonal profile is less complicated, but conversely there may also be some clues in the reproductive history of female ALS patients.
Due to their rarity, studying the 2D:4D phenomena in patients with familial ALS, particularly those with known mutations such as SOD1, is likely to prove difficult. It is unknown whether this pathway will be relevant to those with an inherited etiology, which includes our animal models of ALS.
Conclusions
We have proposed a concise hypothesis with explanatory power for an unexplained finding in ALS, predictive power that suggests new avenues of research, and falsifiability through re-analysis of existing data or the execution of new research studies. This hypothesis is presented with the goal of stimulating debate, discussion, and data in order to uncover the mechanisms of ALS, improve the outcomes of patients, and some day find a cure.
Declaration of interest: PW is an employee of PatientsLikeMe and owns stock/stock options in the company. PatientsLikeMe has received research support from Abbott, Accorda, Avanir, Johnson & Johnson, Merck, Novartis, UCB, and Sanofi. This study received no external funding. The author alone is responsible for the content and writing of the paper.
Related Research Data
References
- Wijesekera LC, Leigh PN. Amyotrophic lateral sclerosis. Orphanet J Rare Dis. 2009;4:3.
- Lill CM, Abel O, Bertram L, Al-Chalabi A. Keeping up with genetic discoveries in amyotrophic lateral sclerosis: the ALSoD and ALSGene databases. Amyotroph Lateral Scler. 2011;12:238–49.
- Driscoll T, Nelson DI, Steenland K, Leigh J, Concha-Barrientos M, Fingerhut M, . The global burden of disease due to occupational carcinogens. Am J Ind Med. 2005;48:419–31.
- O'Carroll RE, Masterton G, Dougall N, Ebmeier KP, Goodwin GM. The neuropsychiatric sequelae of mercury poisoning. The Mad Hatter's Disease revisited. Br J Psychiatry. 1995;167:95.
- Sutedja NA, Fischer K, Veldink JH, van der Heijden GJ, Kromhout H, Heederik D, . What we truly know about occupation as a risk factor for ALS: a critical and systematic review. Amyotroph Lateral Scler. 2009;10:295–301.
- Vivekananda U, Manjalay Z, Ganesalingam J, Simms J, Shaw CE, Leigh PN, . Low index-to-ring finger length ratio in sporadic ALS supports prenatally defined motor neuronal vulnerability. JNNP. 2011;82:635–7.
- Manning JT, Fink B. Digit ratio (2D:4D), dominance, reproductive success, asymmetry, and sociosexuality in the BBC Internet Study. Am J Hum Biol. 2008; 20: 451–61.
- Hönekopp J, Schuster M. A meta-analysis on 2D:4D and athletic prowess: substantial relationships but neither hand out-predicts the other. Pers Indiv Differ. 2010; 48: 4–10.
- Tester N, Campbell A. Sporting achievement: what is the contribution of digit ratio? J Pers. 2007; 75: 663–78.
- Manning JT, Morris L, Caswell N. Endurance running and digit ratio (2D: 4D): implications for fetal testosterone effects on running speed and vascular health. Am J Hum Biol. 2007; 19: 416–21.
- Harwood CA, McDermott CJ, Shaw PJ. Physical activity as an exogenous risk factor in motor neuron disease (MND): a review of the evidence. Amyotroph Lateral Scler. 2009; 10: 191–204.
- Armon C. An evidence-based medicine approach to the evaluation of the role of exogenous risk factors in sporadic amyotrophic lateral sclerosis. Neuroepidemiology. 2003; 22: 217–28.
- Scarmeas N, Shih T, Stern Y, Ottman R, Rowland LP. Premorbid weight, body mass, and varsity athletics in ALS. Neurology. 2002; 59: 773–75.
- Carmel A. Sports and trauma in amyotrophic lateral sclerosis revisited. J Neurol Sci. 2007; 262: 45–53.
- Mattsson P, Lönnstedt I, Nygren I, Askmark H. Physical fitness, but not muscle strength, is a risk factor for death in amyotrophic lateral sclerosis at an early age. JNNP. 2010; Published online early, September 18.
- Beghi E, Logroscino G, Chiò A, Hardiman O, Millul A, Mitchell D, . Amyotrophic lateral sclerosis, physical exercise, trauma and sports: results of a population-based pilot case-control study. Amyotroph Lateral Scler. 2010; 11: 289–92.
- Chiò A, Benzi G, Dossena M, Mutani R, Mora G. Severely increased risk of amyotrophic lateral sclerosis among Italian professional football players. Brain. 2005; 128: 472.
- Carmel A. Re ‘Amyotrophic lateral sclerosis and soccer: a different epidemiological approach strengthens the previous findings’. J Neurol Sci. 2008; 269: 188–90.
- Harwood CA, McDermott CJ, Shaw PJ. Physical activity as an exogenous risk factor in motor neuron disease (MND): a review of the evidence. Amyotroph Lateral Scler. 2009; 10: 191–204.
- Huisman MHB, de Jong DW, Verwijs MC, Schelhass HJ, van der Kooi AJ, de Visser M, . Family history of neurodegenerative and vascular diseases in ALS, a population based study. Neurology. 2011; 77: 1363–9.
- Manning JT, Taylor RP. Second-to-fourth digit ratio and male ability in sport: implications for sexual selection in humans. Evol Hum Behav. 2001: 22: 61–9.