
Abstract
Radial head represents a secondary elbow stabilizer for varus-valgus and postero-lateral stress. In complex fractures, that cannot be synthesized, the presence of associated ligament injuries makes radial head replacement necessary to restore elbow stability. This study evaluates how the elbow responds to a prosthetic removal after a complex injury repair.
Introduction
The radial head represents a secondary stabilizer of the elbow for varus-valgus and postero-lateral stress. Furthermore, it is the primary opponent of the proximal migration of the radius.[Citation1,Citation2] Often, when a radial head fracture cannot be synthesized,[Citation3] surgeons have to decide whether to perform a resection of the radial head or its prosthetic replacement. The main discriminating factor is represented by possible associated ligament injuries: if the elbow is stable, a radial head resection can provide good clinical results.[Citation4] On the other hand, if ligament lesions determine elbow or forearm instability, a radial head replacement is necessary.[Citation5,Citation6] Although the number of radial head prosthesis is constantly on the rise, literature offers results mainly in the short or the medium term,[Citation7] showing frequent complications that often lead to a revision of the prosthesis. The most frequent problems are overstuffing, mobilization of the implant, or breakage especially of the silicone implants.[Citation8] Radial head fractures are more frequent in a young/adult population,[Citation9] and this category also shows the highest percentage of surgical revision. In these cases, most of the authors agree on choosing a prosthesis replacement. The prosthesis removal, which may be regarded as a secondary resection arthroplasty, may also be an option if the elbow is considered to have regained its stability. However, literature is poor on this subject and provides very few short- to medium-term results about prosthesis revision.[Citation8,Citation10]
We report a case of a patient with radial head fracture-dislocation that underwent an acute prosthesis replacement. Surgical revision was needed after the implant ruptured some 2.5 years after and a resection arthroplasty was preferred.
Case report
We report the case of a 25-year-old male, right handed, who suffered from a fracture-dislocation of the left radial head (Mason IV) after a motorcycle incident (). The patient underwent acute surgery for one attempt of open reduction and internal fixation. It resulted impossible for the comminution of the fracture and the surgeons proceeded to resection of the radial head followed by the implant of a press-fit radial head prosthesis (MoPyC, Tornier SAS Etablissement Bioprofile, Grenoble, France), through a postero-lateral access using the Kocher muscular interval. An insufficient intra-operatively stability requested a reinsertion of collateral lateral ligament performed by a Mytec anchor 2.0. The ligament reinsertion and the implant was initially protected and stabilized with an articulated external fixator, maintained for 40 days after surgery (). The intra-operatively evaluation of flex-extension was complete (0–140°). The patient was dismissed without any major complications.
Figure 1. Radial head fracture (Mason IV).

Figure 2. Radial head prosthesis.

One year after surgery, the patient underwent a clinical, functional and radiological evaluation, under the control of clinicians not involved in the surgery. The patient was also asked to answer the following questionnaires: VAS (visual analogic scale), DASH (disability of the arm, shoulder and hand), MEPS (Mayo elbow performance score) and the Oxford elbow score.
The ROM showed a flexion of the elbow of 140° with a lag extension of 25°, reducible to 20° passively and a complete prono-supination. The elbow was stable on both studied plane. An area of paresthesia was evidenced on the ulnar nerve territory, and the strength showed physiological values. The average results of the scores were the following: VAS 3, DASH 12.5, MEPS 85 and an Oxford Elbow score of 34.
The same patient, at a distance of about 2.5 years from the first traumatic episode, came again to our attention with pain in the left elbow, which appeared after a movement of prono-supination in extension. A rupture of the prosthetic stem was shown on the radiographs (). The patient underwent, as a result, a new surgical procedure. During surgery, after the prosthetic removal, stability tests were performed under anesthesia showing an acceptable stability of the elbow. Based on this evaluation, it was decided not to implant a new radial head prosthesis (). The patient was dismissed without any further complication.
Figure 3. Rupture of the prosthetic stem.

Figure 4. Prosthetic removal.

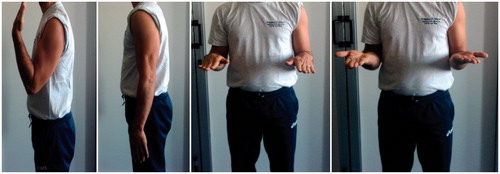
Twenty-seven months after the second surgery, the patient was evaluated investigating all the same parameters listed above. ROM, sensibility and strength showed values similar to those of the previous evaluation (); the paresthesias on the ulnar nerve territory persisted. The varus and valgus stability, evaluated with the elbow in extension, and in 30° and 70° of flexion, appeared similar to the opposite elbow. The new scores showed average results of: VAS 1, DASH 4.2, MEPS 100 e Oxford Elbow Score 46. The scores showed better results than the previous one, and the patient reported a subjective improvement, compared to the time spent with the prosthesis.
Figure 5. ROM after resection artrhoplasty.
Discussion
The main goal of the treatment of radial head fracture should be to restore joint anatomy, in order to allow an early recovery of the ROM, to prevent the onset of the most feared complication of all elbow injuries: the stiffness. In young adults, however, majorly concerned about radial head fractures, the recovery of joint function cannot be obtained without the recovery of stability. That is the reason why, in the presence of ligament injuries resulting in a loss of the primary stabilizers of the elbow, the simple resection of the radial head, without its prosthetic replacement, is not indicated. The goal of this study was to evaluate how the elbow responds to a prosthetic removal after a complex injury repair: the elbow of our patient was found to be stable, both objectively and subjectively.
As far as the evaluation of a single patient does not allow any conclusion, the good clinical result obtained in our study suggests the possibility of forming a scar tissue sufficient to ensure elbow stability after a radial head prosthetic removal in Mason IV fracture.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Johnson JA, Beingessner DM, Gordon CD, et al. Kinematics and stability of the fractured and implant reconstructed radial head. J Shoulder Elbow Surg. 2005;14:195S–201S.
- Hotchkiss RN, An KN, Sowa DT, et al. An anatomic and mechanical study of the interosseous membrane of the forearm: pathomechanics of proximal migration of the radius. J Hand Surg. 1989;14A:256–261.
- Vanni S, Matteotti R, Martinasso A, et al. Riduzione e osteosintesi delle fratture del capitello radiale: Indicazioni e tecnica chirurgica. Aggiornamenti CIO Club Italiano Osteosintesi. Springer editore 2012;18:39–44.
- Iftimie PP, Calmet Garcia J, de Loyola Garcia Forcada I, et al. Resection arthroplasty for radial head fractures: long-term follow-up. J Shoulder Elbow Surg. 2011;120:45–50.
- Morrey BF. Radial head fracture. In: Morrey BF, editor. The elbow and its disorders. 3rd ed. Philadelphia (PA): WB Saunders; 2000. p. 341–363.
- Pike JM, Athwal GS, Faber KJ, et al. Radial head fractures – an update. J Hand Surg Am. 2009;34:557–565.
- Vanni S, Mateotti R, Martinasso A, et al. Le protesi di capitello radiale: Studio retrospettivo a medio termine di 19 pazienti con fratture Mason III e IV. GIOT. 2012;38:268–272.
- Duckworth AD, Wickramasinghe NR, Clement ND, et al. Radial head replacement for acute complex fractures. What are the rate and risks factors for revision of removal? Clin Orthop Relat Res. 2014;472:2136–2143.
- Kaas L, van Riet RP, Vroemen JP, et al. The epidemiology of radial head fractures. J Shoulder Elbow Surg. 2010;19:520–523.
- Van Riet RP, Sanchez-Sotelo J, Morrey BF. Failure of metal radial head replacement. J Bone Joint Surg Br. 2010;92:661–667.