Abstract
Objective: To compare the lifetime costs of freeing astigmatic patients from spectacles after bilateral cataract surgery implanting toric intraocular lenses (IOLs: i.e., Acrysof Toric) versus monofocal IOLs, in France, Italy, Germany and Spain.
Methods: A Markov model followed patient cohorts from cataract surgery until death. Prevalence rates of patients not needing spectacles and the types of spectacles prescribed for those requiring them were obtained from clinical trials and national surveys. The economic perspective was societal. Mortality rates were incorporated into the model. Discount rates were applied. A sensitivity analysis was performed on non-discounted costs.
Results: Fewer patients with toric IOLs needed spectacles for distance vision than patients with monofocal IOLs. With monofocal IOLs more than 66% of patients needed complex spectacles compared to less than 25% implanted with toric IOLs. In France and Italy, toric IOLs reduced overall costs relative to otherwise high spectacle costs after cataract surgery. Savings were €897.0 (France), €822.5 (Germany), €895.8 (Italy) and €391.6 (Spain), without discounting. On applying a 3% discount rate the costs became €691.7, €646.4, €693.9 and €308.2, respectively.
Conclusions: Bilateral toric IOL implants in astigmatic patients decreased spectacle dependence for distance vision and the need for complex spectacles. The economic consequences for patients depended on the national spectacle costs usually incurred after cataract surgery.
Introduction
Typical senile cataract progresses slowly and can cause vision loss if untreated. An estimated 20.5 million (17.2%) Americans older than 40 years have cataract in at least one eyeCitation1. While cataract is the leading cause of blindness worldwideCitation2,3, most developed Western populations have access to cataract surgery (e.g., 6.1 million Americans (5.1%) have pseudophakia/aphakia). The total number of Americans with cataract is predicted to increase to 30.1 million by 2020 and of these 9.5 million are expected to have pseudophakia/aphakiaCitation1. In Belgium the annual rate of cataract surgery per 100,000 inhabitants is more than 1,600; in other European countries the figure is between 500 and 1,000Citation4.
More than 80% of patients regain good best-corrected visual acuity (>8/10) after cataract surgery, depending on pre-existing ocular pathology and follow-up durationCitation5–9. Refractive errors in the elderly have been reported by several surveysCitation10–12. Most show an increase of average spherical error related to age. For example, in the Blue Mountain Eye study average spherical error in individuals aged 49–59 years was less than +0.03 D, increasing to +0.8 D in individuals in their sixties, then to +1.0 D for those in their seventies, and to +1.2 D in people over 80. In this study the prevalence rate of high astigmatism (>1.5D) was 13%. In the long-term, spherical refractive error does not change after cataract surgeryCitation13.
Traditional intraocular lenses (IOLs) are monofocal and after implantation most patients need spectacles for at least near vision, and in cases of astigmatism may need them for distance vision, too. With corneal astigmatism, total astigmatism can be effectively reduced or even eliminated by a properly aligned toric IOL, leading to better visual acuity and no need for spectacles or contact lenses.
Acrysof Toric IOLs are an additional option for cataract patients presenting with significant corneal astigmatism. When this IOL is properly aligned with the corneal astigmatism, total astigmatism of the affected eye can be effectively reduced, or even eliminated, resulting in better visual acuity and no necessity for spectacles or contact lenses. The results of a US clinical trial on the necessity for distance vision spectacles demonstrated the advantage of this IOL strategy. It showed that 97% of patients with bilateral toric implants (11.4% of the whole population) declared they no longer required spectacles for distance vision. Also, statistically significant differences between spectacle purchases (as declared by patients) were noted with regard to lens type or the need for them. With bilateral toric lenses more than 75% of patients either abandoned spectacles or solely needed reading spectacles, as compared to 36% given traditional IOLs. However, any rotation of a toric IOL away from its intended axis can reduce astigmatism correction, hence in 1.6% of cases it is necessary to operate a second time to reposition or replace the implantCitation14.
According to Vitale et al Citation15 more than 110 million Americans could, or do, achieve normal vision after refractive correction. However, spectacle prescriptions incur costs for both patients and health insurance providers. The annual direct cost of simply correcting impaired distance vision was at least $3.8 billionCitation15, of which $780 million was related to treating subjects aged >65 years. Few published data exist on the costs associated with spectacle dependence after cataract surgery, apart from a survey conducted by Cuq et al Citation16 in France, Germany, Italy and Spain, which found costs varying from €230 (Spain) to €579 (France). The latter estimates were used recently to populate a medico-economic model comparing complex and monofocal implantsCitation17.
The aim of the present economic analysis was to compare the lifetime costs and consequences of reducing spectacle dependence in astigmatic patients after cataract surgery, by contrasting toric and monofocal IOLs with the foregoing medico-economic model.
Patients and methods
This economic study used a Markov model to estimate the lifetime cost consequences for society (i.e., patients) in four European countries (France, Germany, Italy and Spain) after implanting monofocal or toric IOLs during cataract surgery.
DATA PRO 2008 software was used to build a Markov model simulating cohorts of patients given bilateral IOLs during cataract surgery at age 70 years and following them until death, or age 100 years. Patients were assigned to one of two possible health states after cataract surgery, i.e. spectacles not needed, or spectacles needed and purchased. Frequency rates of ‘spectacles not needed’ and ‘type of spectacles needed’ were derived from the previously cited US controlled clinical trialCitation14 and the European surveyCitation16. A specific health state was created for ‘toric IOL re-intervention risk’ to accommodate cases of axial rotation. During all subsequent cycles patients entered one of the following states: ‘spectacles not needed’, ‘spectacles needed and purchased’, ‘further spectacles not needed’ (i.e., current spectacles satisfactory), and ‘death’ (). The cycle duration was 1 month and patients were dropped from the model at death or on reaching age 100 years. National mortality statistics were used for life expectancyCitation18–21.
The primary analysis compared patients with bilateral toric IOLs versus patients with bilateral monofocal IOLs. A one-way sensitivity analysis was performed without discount.
Prevalence rates of ‘patients not requiring spectacles’ and of ‘spectacle types’ needed after cataract surgery were obtained from the US randomised clinical trialCitation14 and the European dedicated surveyCitation16.
The aims of the 1-year US study, above, conducted at 11 centres, were to compare the AcrySof Toric (Alcon, Forth Worth, TX) IOL with an AcrySof (Alcon, Forth Worth, TX) spherical IOL as control, and to investigate the rotational stability of the toric IOL in subjects with prior corneal astigmatism. It showed that the toric IOL provided excellent efficacy, rotational stability, safety, and independence from distance vision spectacles. Limbal Relaxing Incisions (LRIs) were not permitted. A subset of patients was given bilateral IOL implants and their spectacle requirements were used to model everyday practice as closely as possible. A total of 517 subjects (toric IOL: n=256; control IOL: n=261) were included.
The dedicated European survey demonstrated that spectacles purchased after monofocal IOL implantation varied across the four countries. Accordingly, the US clinical trial results with monofocal IOLs were adjusted for each European market involved. The adjustment was not possible for toric IOLs because corresponding data are not yet available.
The main findings of the US clinical trial and European survey used in the present model are shown in .
In the absence of a pan-European, well-controlled, randomised clinical trial, comparing monofocal with toric IOLs in bilaterally implanted patients, a conservative approach (i.e., minimising the toric benefit) was taken.
The probability of wearing spectacles was estimated from the US clinical trial and applied to the intention-to-treat population (unilateral and bilateral implants) with the subset of bilaterally implanted patients who had a higher probability of freedom from spectaclesCitation14. With respect to the type of spectacles prescribed for toric IOL patients, estimates from the bilaterally implanted US patients were taken to be ‘toric specific’. The type of spectacles required after monofocal implants was taken from the European survey, since spectacle supply and reimbursement are key drivers of refraction choicesCitation16.
Resources and costs in the four European countries were based on estimates derived from a previously cited medico-economic modelCitation17, which used costs of resources consumed, spectacles and other medical costs extracted from official national sourcesCitation16. Resources consumed and cataract surgery costs were as follows: (1) surgery (both eyes) and additional intervention costs, as appropriate; (2) bilateral IOLs (monofocal or toric); (3) time allotted to surgery (including transport); and (4) other transport to the clinic. Resources consumed by patients requiring spectacles were, as follows: (1) consultations with ophthalmologists or optometrists for prescriptions; (2) transport and time spent during the visits; (3) visits to optical centres; (4) time spent on choosing and collecting spectacles; and (5) transport to ophthalmologists' or optometrists' offices. The annual rate of spectacle replacement was estimated from the European surveyCitation16 which showed that many patients change their spectacles every 2–3 years (France: 33.3%; Italy: 37.0%; Germany: 42.5% and Spain:48.3%).
In addition to the model, the following periodic consumption of resources relating to spectacles was costed: (1) visits to an optical centre for frame maintenance; (2) time spent on the visit; (3) cleaning materials purchased; and (4) transport to the optical centre.
Costs were expressed as euros. A discount rate of 3% was fixed for the principal analysis.
National tariffs and estimates were used to cost medical resources consumedCitation17. The following unit costs were estimated from national tariffs and other available sources:
| (a) | According to a European surveyCitation16 most people spend from €200 to €400 on a pair of spectacles, except in France where the majority pay more than €500. Spectacle costs are not reimbursed, except in FranceCitation22; | ||||
| (b) | The average cost of cataract surgery varied from €1,050 in Spain to €1,250 in Germany, including the cost of a monofocal intra-ocular implantCitation23–26. The incremental cost for a toric IOL was estimated by applying the break-even price (both strategies having the same overall cost) in the model. | ||||
| (c) | Ophthalmologists' consultation fees varied from €25 in France to €100 in Italy, with optometrists' costs influenced by official regulations, i.e. in Italy and Germany optometry is not a recognised profession and many optometrists do not charge for a visit, whereas in Spain optometrists' costs are regulated at €40 without NHS reimbursementCitation24,27–30; | ||||
| (d) | Spectacle cleaning materials (sprays and cloths) varied widely in cost, according to package size, brand and accessories (chains), hence an approximated average cost of €3 was applied to the present analysis; | ||||
| (e) | as costs per kilometre and type of transportation differed between countries (taxis from €0.9 in France to €1.80 in Spain, with subway and bus costs similar at about €0.20 –– depending on the ticket and distance covered) different internet sourcesCitation31–34 were solicited to obtain an approximated average cost of €0.40 per kilometre weighted by the proportion of subjects using these types of transportationCitation16; | ||||
| (f) | ‘Time spent’ was economically valued using estimated hourly earnings published by the European Union Statistical OfficeCitation35. | ||||
Mean cost estimates are presented in
Results
According to the Markov model, and using national mortality statistics for each country, the average life expectancy of patients aged 70 years ranged from 14.4 years in Germany to 16.0 years in France, reflecting differences in general life expectancyCitation36. The average estimated duration of spectacle use in the two IOL groups was 12.9–14.0 years for the monofocal patients and 13.5–15.0 years for those with toric IOLs (). The duration of using reading spectacles only was much longer in the toric IOL group (10.1–11.2 years) than the monofocal IOL group (1.7–6.6 years). Fewer patients with toric IOLs needed spectacles for distance vision than patients with monofocal IOLs.
shows average resource consumption per patient according to type of IOL implanted and country. Resources used solely on reading spectacles were greater for the toric group. Patients with monofocal IOLs required reading spectacles, too, but this need was satisfied by bifocal or varifocal prescriptions. Hence, the toric IOL group had fewer requirements for bifocal or varifocal combinations owing to the ‘beneficial effect’ of the toric IOL.
Costs between countries were marked, reflecting price differences in spectacle markets.
compares the estimated societal costs for patients implanted with monofocal IOLs or toric IOLs, according to the main scenario. IOL costs are considered equal for the purpose of this table. Savings with toric IOLs stemmed mainly from shifting spectacle needs towards the less expensive reading correction. Savings were reported in all countries: €691.7 (France), €646.4 (Germany), €693.9 (Italy) and €308.2 (Spain). The lower savings in Spain were due to lower spectacle costs. Although major savings were achieved with direct spectacle costs, other costs borne by patients (e.g., transportation and time) remained significant. Savings applied generally irrespective of the actual spectacle costs.
presents a sensitivity analysis without discounting. Undiscounted costs generally increased savings.
Discussion
The present economic analysis in four European countries (France, Germany, Italy and Spain) estimated the costs and consequences of cataract surgery in patients with pre-existing corneal astigmatism and toric or monofocal IOL implants at age 70, followed-up until death or age 100 years.
The economic perspective was that of society (i.e., patients) since toric IOL technology is new and not currently reimbursed by the countries modelled. Nonetheless, government health services finance almost 100% of cataract surgery and visits to ophthalmologists for vision correction by reimbursements to patients. In addition, these reimbursements always include the price of a standard monofocal IOL implant irrespective of the actual IOL implanted. However, spectacles are not covered by the national health services, except in France where reimbursement rates are low.
The current study was based on national data (mortality and cataract prevalence), clinical trials, and a survey embracing all four countries. Every effort was made to maintain good internal validity (use of randomised clinical trial data) and a good external validity (use of country specific surveys to document the standard of care) in relation to all available data sources, as recommended by most health economics guidelinesCitation37. A randomised clinical trial in all the countries is needed to confirm the findings of this study.
Within a time horizon of 30 years and a 3% discount rate, toric implants introduced economic savings (mainly for patients) in all four countries [ranging from –€308.2 to –€693.9]. The fact that the discount rate significantly modified the results [–€391.6 to –€897.0] is not surprising given the long follow-up period built into the model (up to 30 years).
Non-financial benefits of freedom from distance spectacles after cataract surgery were not evaluated in this analysis. However, in addition to savings with toric IOLs, cataract patients with corneal astigmatism appeared willing to pay for the benefits of spectacle independence. This study has the following limitations: (1) a model cannot replace longitudinal data collection, but the feasibility and economics of such a survey are questionable; (2) it was hypothesised that the prevalence rate of spectacle independence remains constant until the end of a patient's life, whereas the known efficacy of toric implants does not yet extend that far. In addition, refractive errors might be modified by IOLsCitation13; (3) the external validity of the survey concerning spectacle costs could be challenged, but the cost structure was coherent across countriesCitation16; (4) in order to document spectacle independence rates a trial was used in which few patients were implanted bilaterally (5); lastly, spectacle prescription rates were applied from US patients to four European countries where spectacle use and reimbursement are known to be country specific.
The model did not take into account other techniques for correcting astigmatism. It was decided not to include LASIK (laser in-situ keratomileusis) as an alternative, since LASIK has already demonstrated to be a cost-effective alternative to spectaclesCitation38. LRI was not considered during cataract surgery because: (1) according to experts (in the absence of national statistics) it seems to be rarely performed; (2) estimates relating to spectacle type were taken from a trial that did not allow LRIs; and (3) the long-term effectiveness of LRI is questionable and poorly documentedCitation39–42.
The current model showed that cost savings with toric IOLs achieved in four European countries benefited society (i.e., patients, who bore the costs directly). This explains a shift of costs to society, lying entirely outside National Health Service budgets which reimbursed cataract surgery, but not the costs of refraction visits. Patients, on the other hand, avoided the costs related to care and refraction treatment. It is worth noting, too, that the costs met by patients exceeded those of the national health services.
In conclusion, according to the study data and model from a societal perspective, toric IOL implants were a cost saving alternative to monofocal IOLs in cataract surgery. Additional country specific data collection with well-controlled methodology is needed to confirm these findings.
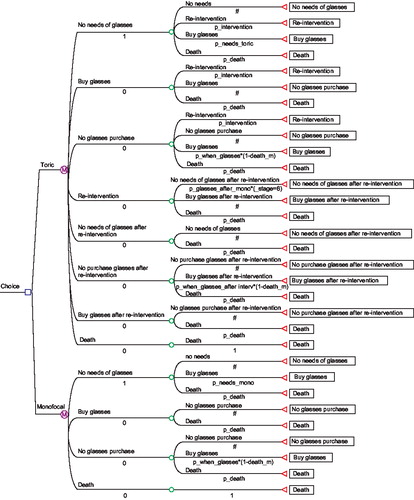
Table 1. Results of the clinical trial comparing toric IOL and monofocal IOL and of the European survey.
Table 2. Unit costs (societal) according to country and type of resource consumed (€).
Table 3. Average time (years) with and without spectacles in the Markov model period according to toric, monofocal implants and countries.
Table 4. Average resources per patient consumed in the Markov model period according to toric, monofocal implants and countries.
Table 5. Cost consequences (€) according to toric and monofocal IOLs per country from the societal perspective – discount rate 3%.
Table 6. Cost consequences (€) according to toric and monofocal IOLs per country from the societal perspective – discount rate 0%.
Acknowledgement
Declaration of interest: This analysis was supported by a grant from Alcon France SA, Rueil-Malmaison, France. The analysis was performed by Cemka Eval, Bourg-la-Reine, France. Dr Gilles Berdeaux is employed by Alcon France. The authors would like to thank Robert Pigache MD, FFPM for his help with reviewing the English text.
Notes
* Acrysof Toric is a registered trade name of Alcon Laboratories Inc, Fort Worth, TX, USA.
References
- Congdon N, Broman KW, Lai H, et al. Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Arch Ophthalmol 2004;122:487–494.
- Javitt JC, Wang F, West SK. Blindness due to cataract: epidemiology and prevention. Annu Rev Public Health 1996;17:159–177.
- Agency for, Health Care, Policy Research. Cataract in Adults: Management of Functional Impairment. Rockville, MD: AHCPR, 1993
- OECD. Health at a Glance 2007, Organisation for Economic Co-operation and Development (OECD), Paris, 2007.
- Anmarkrund N, Bergaust B, Bulie T, et al. Evaluation of a flexible one-piece open-loop anterior chamber lens Symflex 350B 3-4 years after implantation. Acta Ophthalmol 1993;71:796–800.
- Pötzsch DK, Lösch-pötzsch M. Four year follow-up of the Memorylens. J Cataract Refract Surg 1996;22:1336–1341.
- Schmack WH, Gerstmeyer K. Long-term results of the foldable CeeOn edge intraocular lens. J Cataract Refract Surg 2000;26: 1172–1175.
- Milazzo S, Turut P, Artin B, et al. Long-term follow-up of three-piece, looped, silicone intraocular lenses. J Cataract Refract Surg 1996;22(Suppl 2):1259–1262.
- Linnola RJ, Holst A. Evaluation of a 3-piece silicone intraocular lens with poly(methyl methacrylate) haptics. J Cataract Refract Surg 1998;24:1509–1514.
- Attebo K, Ivers RQ, Mitchell P. Refractive errors in an older population: the Blue Mountains Eye Study. Ophthalmology 1999;106: 1066–1072.
- Sawada A, Tomidokoro A, Araie M, et al. Refractive errors in an elderly Japanese population: the Tajimi study. Ophthalmology 2008;115:363–370.
- Vitale S, Ellwein L, Cotch MF, et al. Prevalence of refractive error in the United States, 1999-2004. Arch Ophthalmol 2008;126:1111–1119.
- Guzowski M, Rochtchina E, Wang JJ, et al. Refractive changes following cataract surgery: the Blue Mountains Eye Study. Clin Experiment Ophthalmol 2002;30:159–162.
- ALCON R&D Biostatistics. Biostatistics Clinical Study Report. Bilateral spectacles independence. Ref Pc1427.18 Date: 2/22/2006
- Vitale S, Cotch MF, Sperduto R, et al. Costs of refractive correction of distance vision impairment in the United States, 1999–2002. Ophthalmology 2006;113:2163–2170.
- Cuq C, Lafuma A, Jeanbat V, et al. A European survey of patient satisfaction with spectacles after cataract surgery and the associated costs in four European countries (France, Germany, Spain and Italy). Ophthalmic Epidemiol 2008;15:234–241.
- Lafuma A, Berdeaux G. Modelling lifetime cost consequences of ReSTOR in cataract surgery in four European countries. BMC Ophthalmol 2008;8:12.
- Institut National de la Statistique et des Études Économiques. Recensement de la population 1999 – Exploitation principale – Ed INSEE, Paris, France, 1999. Available at: http://www.insee.fr/. [Last accessed March 2009].
- Statistisches Bundesamt Deutschland (Federal Statistical Office, Germany) Available at: www.destatis.de. [Last accessed March 2009].
- ISS Istituto Superiore di Sanità (dati ISTAT). Available at: www.iss.it. [Last accessed March 2009].
- World Population Prospects. The 2004 Revision. Datasets in Excel and pdf formats. New York: United Nations, Department of Economic and Social Affairs – Population Division, 2005.
- Liste des produits et des prestations. Sécurité Sociale. L'assurance maladie. Available at: http://www.codage.ext.cnamts.fr/codif/tips/chapitre/index_chap.php?p_ref_menu_code=46&p_site=AMELI. [Last accessed July 2007].
- Publication de l'échelle nationale des coûts (données 2003-2004). Agence Technique de l'Information sur l'Hospitalisation. Available at: http://www.atih.sante.fr/?id=000370000DFF. [Last accessed March 2009].
- Centro de Estudios en Economia de la Salud y de la Política Social (SOIKOS) [Spanish Database on Medical Costs]. SOIKOS Database 2004. Available at: http://www.soikos.com. [Last accessed July 2007].
- DRG on Line Available at: http:// www.drg.it. [Last accessed March 2009].
- Medizincontrolling/DRG Research Group. Universitätsklinikum Münster Westfälische Wilhelms-Universität Münster. Available at: http://drg.uni-muenster.de/de/webgroup/m.brdrg.php?baserate=2900&showgrafik=0&version=GDRG2005;&mdc=02 July 2007. [Last accessed July 2007].
- Classification Commune des Actes Médicaux. CCAM France NGAP Sécurité sociale. Available at: http://www.ameli.fr/l-assurance-maladie/documentation-technique/t2a-ccam-et-lpp/index.php. [Last accessed March 2009].
- Ministero della Sanità. Nomenclatore Tariffario delle prestazioni ambulatoriali DM 22.7.96; Gazzetta Ufficiale n° 216, 14.9.96.
- Gebühren-Handbuch 2000. Kommentar für Ärzte. EBM. GOÄ. Maximilian G. Broglie, u. a, Inter Medical, Wiesbaden, Taschenbuch [3922264018].
- Kassenärztlichen Vereinigungen, 2000. Available at: http://www.ebm2000plus.de. [Last accessed March 2009].
- Société Nationale des Chemins de Fer. Available from: www.sncf.fr. [Last accessed July 2007].
- Mobilcheck Deutsche Bahn, ADAC. Available at: http://www.bahn.de. [Last accessed July 2007].
- CONSUMER EROSKI nº 92, oct 2005. Available at: http://revista.consumer.es/discapacitados/es/20051001;/actualidad/tema_de_portada/#language. [Last accessed July 2007].
- Régie autonome des transports parisiens. RATP. Titres et tarifs. Available at: http://www.ratp.fr/. [Last accessed July 2007]
- EUROSTAT - Available at: http://epp.eurostat.ec.europa.eu. [Last accessed March 2009].
- OECD health data. IRDES, Paris, France.
- Hjelmgren J, Berggren F, Andersson F. Health economic guidelines - similarities, differences and some implications. Value Health 2001;4:225–250.
- Berdeaux G, Alio J, Martinez J-M, et al. Socio-economics aspects of laser in situ keratomileusis, spectacles & contact lens in mild to moderate myopia. J Cataract Refract Surg 2002;28:1914–1923.
- Kaufmann C, Peter J, Ooi K, et al. The Queen Elizabeth Astigmatism Study Group. Limbal relaxing incisions versus on-axis incisions to reduce corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg 2005;31:2261–2265.
- Müller-Jensen K, Fischer P, Siepe U. Limbal relaxing incisions to correct astigmatism in clear corneal cataract surgery. J Refract Surg 1999;15:586–589.
- Bayramlar H, Totan Y, Daghoglu MC. Limbal relaxing incision for the management of mixed astigmatism after photorefractive keratectomy and laser thermal keratoplasty. J Cataract Refract Surg 2000;26:1266.
- Bleckmann H, Keuch RJ. Implantation of spheric phakic posterior chamber intraocular lenses in astigmatic eyes. J Cataract Refract Surg 2002;28:805–809