
Abstract
Objective:
To evaluate cost effectiveness and cost utility comparing robot-assisted laparoscopic prostatectomy (RALP) versus retropubic radical prostatectomy (RRP).
Methods:
In a retrospective cohort study a total of 231 men between the age of 50 and 69 years and with clinically localised prostate cancer underwent radical prostatectomy (RP) at the Department of Urology, Aarhus University Hospital, Skejby from 1 January 2004 to 31 December 2007, were included.
The RALP and RRP patients were matched 1:2 on the basis of age and the D’Amico Risk Classification of Prostate Cancer; 77 RALP and 154 RRP.
An economic evaluation was made to estimate direct costs of the first postoperative year and an incremental cost-effectiveness ratio (ICER) per successful surgical treatment and per quality-adjusted life-year (QALY). A successful RP was defined as: no residual cancer (PSA <0.2 ng/ml, preserved urinary continence and erectile function. A one-way sensitivity analysis was made to investigate the impact of changing one variable at a time.
Results:
The ICER per extra successful treatment was €64,343 using RALP. For indirect costs, the ICER per extra successful treatment was €13,514 using RALP. The difference in effectiveness between RALP and RRP procedures was 7% in favour of RALP. In the present study no QALY was gained 1 year after RALP, however this result is uncertain due to a high degree of missing data. The sensitivity analysis did not change the results noticeably.
Limitations:
The study was limited by the design resulting in a low percentage of information on the effect of medication for erectile dysfunction and only short-term quality of life was measured at 1 year postoperatively.
Conclusion:
RALP was more effective and more costly. A way to improve the cost effectiveness may be to perform RALP at fewer high volume urology centres and utilise the full potential of each robot.
Introduction
Prostate cancer is in the western world the most frequent malignant disease in urology. Due to the introduction of new diagnostic tools, the incidence increases rapidly with the consequence of heavy stress on the economical burden in public healthcare. Most new cases are feasible for curative treatment such as surgery or radiotherapy. The traditional surgical method, retropubic radical prostatectomy (RRP) has been replaced in the last decade by a computer-assisted methodology – robot-assisted laparoscopic prostatectomy (RALP) – because of its expected better outcome. The cost of RALP is more than twice the cost of RRP. It therefore is relevant and urgent to compare the two methodologies from a cost-effectiveness perspective.
The increased use of RALP from 1% in 2001 to 40% in 2006 has opened up a debate concerning prioritisation of the economic resources between RALP and RRP which is related to the purchase and maintenance of the operative equipment for RALPCitation1–3. As in other countries, the use of RALP in Denmark has expanded rapidly. The incidence of prostate cancer was 136 per 100,000 men and the disease specific mortality 19.5 per 100,000 patients in Denmark in 2008Citation4,Citation5. At Aarhus University Hospital, Skejby, RRP has been performed as a standard procedure since 1997 and is still a common methodology; RALP was introduced in 2005 using the da Vinci system.
RALP is normally considered as a more costlyCitation2,Citation3,Citation6,Citation7 and marginally more effective procedure compared to RRPCitation1,Citation8,Citation9 although no randomised controlled trial has ever been carried out to compare the efficacy, safety and costs of the two alternative surgical procedures. A study by Schroeck et al. found that patients who underwent RALP were three to four times more likely to be regretful and dissatisfied compared to patients undergoing RRP. According to Schroeck et al. this result could be attributed to higher expectations of RALPCitation10. It is important for decision-makers to be informed about the economic consequences and effects of introducing a new medical technology such as RALP. This information is limited and is often supplied by the manufacturer. To our knowledge, no economic evaluation of radical prostatectomy comparing RALP and RRP is available. Unfortunately, it is therefore not yet clarified which alternative of RALP and RRP is most cost effective.
This study aimed at evaluating short-term cost effectiveness and cost utility comparing RALP and RRP, respectively in a group of matched patients.
Methods
Economic evaluation
A health economic evaluation was performed alongside a retrospective cohort-control study of prostate cancer patients treated with radical prostatectomy and followed 1 year postoperatively. The incremental cost-effectiveness ratio (ICER), i.e. the extra costs of RALP compared to RRP divided by the extra gained patient outcome from RALP compared to RRP, was calculated according to international guidelines on health economic evaluationCitation11. The ICER was calculated from a societal perspective, i.e. all costs were included. All prices were quoted in euros, 2008 prices, and exclusive of value added tax (VAT).
Two outcome measures were used: (1) a successful surgical treatment and (2) quality-adjusted life-years (QALY). Successful radical prostatectomy was defined as no residual cancer (prostate-specific antigen (PSA) <0.2 ng/ml), urinary continence and erectile function with or without medical treatment. To estimate QALY within the first postoperative year, the SF-36 score was translated to SF-6D using Brazier’s algorithmCitation12. The patients were asked to fill out a SF-36 questionnaire at baseline and 1 year postoperatively. SF-36 is a generic, but not a preference-based instrument and, thus, needs to be ‘translated’ into utility-weights to be used to calculate gained QALYs. The difference in the derived utility-weight between baseline and 1 year constitutes the gained QALYs for each group.
A cost-effectiveness analysis was made to estimate ICER per successful operation with and without indirect costs (absence from work) using the human capital methodCitation11. A cost-utility analysis was made to estimate ICER per QALY.
The effects of changes in selected costs and clinical parameters were examined in a one-way sensitivity analysis and independently illustrated in a Tornado chart.
Clinical study
The study cohort consisted of 231 men between 50 and 69 years with prostate cancer stages cT1–T2 undergoing RP at the Department of Urology, Aarhus University Hospital, Skejby from 1 January 2004 to 31 December 2007.
The RALP and RRP patients were matched 1:2 on the basis of age within 5-year groups and the D’Amico Risk Classification of Prostate CancerCitation13; this resulted in inclusion of 77 consecutive RALPs with clinical localised cancer cT1–T2 and 154 matching RRPs, respectively. In total, 356 eligible patients underwent RP (271 RRP and 85 RALP). Patients with stage cT3 disease were excluded because of the higher risk of urinary incontinence and recurrence postoperatively and were mainly assigned to the open procedure.
The power was calculated to be 23% based on the study population of 231 men and the minimum relevant difference for a successful surgical treatment of 7% between the two groups of patients.
All patients were followed prospectively according to department procedures for the Prostate Cancer project. Each patient was observed from day of surgery to 1 year postoperatively where differences in side-effects were assumed to be steady state. Long-term follow-up of the oncological outcome was desirable but was outside the scope of this study.
The in-hospital data were collected from the medical journals. Data on general practitioner consultations, acute hospital admissions were collected from the Danish National Registry of Patients at the Danish National Board of Health and from the Health Service Registry, Central Denmark Region. Data on absence from work was taken from The Sickness Absence Registry at the Ministry of Employment.
All patients had three outpatient visits during the first postoperative year as planned follow-up visits at 3, 6, and 12 months postoperatively. The short form health survey SF-36 was filled in at baseline and 1 year postoperatively.
Costs
The valuation of costs components included in the economic evaluation is listed in .
Table 1. Assessment of cost components in the economic evaluation.
The life time of the da Vinci robot was assumed to be 5 years and depreciated by 3% to estimate the annual costsCitation11. The replacement cost (purchase price) of the da Vinci robot was estimated to be €1.4 millionCitation25 with an equivalent annual cost calculated to be €380,135 using the standard annualisation methodCitation11. Maintenance costs were estimated to be €120,100 per yearCitation25.
It was assumed that 70 RALP procedures were performed annually based on the level of activity in 2008 at our department. The costs for da Vinci were distributed between a total of 110 robot-assisted procedures yearly (70 RALP plus 40 different procedures performed with the same equipment).
The cost of managing side-effects during the first postoperative year by consultations in hospital and primary care as well as the cost of urinary pads and medical drugs were all included in the total cost calculations for both RALP and RRP.
The use of staff resources (nurses and supporting personnel) was estimated by interview. Data concerning sick leave after RP was observed for 1½ years based on previous experiencesCitation26.
The study was approved by the local ethical committee and the Danish Data Protection agency was informed.
Statistics
The two groups of patients were compared using descriptive statistics, tested with t-test, χ2-test or the non-parametric Wilcoxon rank-sum (Mann–Whitney) test as appropriate. Statistical significance was considered when p < 0.05.
Results
There existed a reasonable selection of patients with a larger tumour burden who were to be treated operatively. Patients in the two groups were of equal age (mean age of 62.2 years for RALP and RRP) and risk groups (RALP vs. RRP: patients with preoperative T2 93.5 vs. 94.8%, patients with preoperative Gleason score <7 71.4 vs. 68.8%, and mean PSA 11.6 ng/ml vs. 14.4 ng/ml).
The outcome measures used in the economic evaluation are shown in . The difference between the RALP and the RRP procedures for successful treatment was 7% in favour of RALP (p = 0.3). More RRP patients reported postoperative erectile function compared to RALP patients. On the other hand, prescriptions for erectile medication were more common among the RALP patients ().
Table 2. Effects used in the economic evaluation based on matched* groups of patients and estimated at 1 year postoperatively.
No QALY was gained for RALP patients 1 year postoperatively (). The majority of RRP patients filled in the SF-36 both at baseline and at 12 months postoperatively compared to RALP, 74.7% versus 33.8%, respectively ().
The mean costs per patient and the estimated ICER are presented in .The mean costs per RALP procedure were twice the costs of RRP 1 year postoperatively. Concerning the mean indirect costs per patient, there was no statistically significance between the two groups of patients ().
Table 3. Mean costs, effects, and incremental cost-effectiveness ratio per successful operation 1 year postoperatively. The parameters are calculated as direct costs and indirect costs (direct costs including absences from work), respectively.
The ICER for direct costs was €64,343 per extra successful treatment using RALP (). Since no QALY was gained in favour of RALP it was not possible to estimate the ICER per QALY.
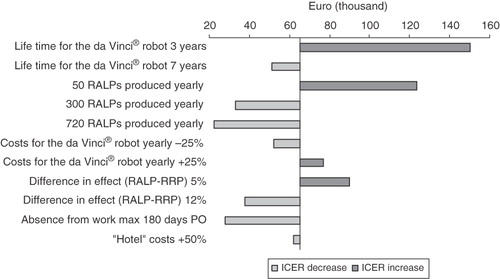
illustrates the impact of selected parameters on the estimated ICER of €64,343 per successful RALP procedure. The ICER decreased when increasing the effectiveness of RALP or with higher utilisation of the da Vinci robot. The costs of RALP would still be higher compared to RRP when the production of RALP was set at 720 annually – this would be equivalent to three RALPs per day, 5 days a week for 48 weeks per year ().
Figure 1. Impact of one-way sensitivity analysis with selected parameters on the estimated ICER of €64,343 per successful treatment using robot-assisted laparoscopic radical prostatectomy. The ICER was estimated assuming 70 RALP were performed annually with the costs for the da Vinci distributed between 110 robot-assisted procedures yearly and a life time for the da Vinci robot of 5 years. A successful treatment was defined as no residual cancer (prostate-specific antigen <0.2 ng/ml), preserved urinary continence and erectile function 1 year postoperatively. RALP robot-assisted laparoscopic radical prostatectomy; RRP, retropubic radical prostatectomy; PSA prostate-specific antigen; PO, postoperatively; ICER, incremental cost-effectiveness ratio.
Discussion
The ICER per extra successful procedure was €64,343 using RALP 1 year postoperatively with a production of 70 RALPs per year and the fixed costs for the da Vinci robot distributed on 110 robot-assisted procedures annually. The more costly RALP procedure was also found to be more effective than RRP. Thus, the assessment of cost effectiveness was not clear per successful RALP procedure. Regarding QALY, RALP procedures were not considered cost effective because the cost were higher and at the same time the procedure was less effective compared to RRP. The selected parameters in the sensitivity analysis did not independently change the results noticeable and our economic evaluation was assessed to be robust to the cost data.
The present study is to our knowledge the first economic evaluation to look at marginal costs (i.e. all costs that vary between the two alternatives) as recommended by most guidelines for health economic evaluations. Additionally, no other cost studies comparing RALP and RRP procedures have estimated costs from a broad societal perspective with a similar high level of precision in costing. The results of previous economic studies are opaque because they are based on different cost models as well as non-clarified methodsCitation2,Citation3,Citation6,Citation7. Minutely, the present study followed the internationally recommended methods for economic evaluationCitation11.
The study estimated incremental effectiveness and costs comparing RALP and RRP procedures. Estimating the success of the treatments we wanted an outcome measure that made a difference and included the potential benefits for RALP stated by the manufacture of the robotic systemCitation27. It is documented that there are no significant differences in continence, erectile function and biochemical progression-free survival between RALP and RRPCitation1,Citation8,Citation9. Therefore, we consider the chosen outcome measure “successful treatment” useful in the discussion of priority of the economic resources between RALP and RRP procedures. The retrospective study design resulted in a low percentage of information on the effect of medication for erectile dysfunction at 1 year postoperatively. A greater share of RALP patients had used prescriptions for medicine for erectile dysfunction compared to RRP patients indicating that more RALP patients might have an erectile function than estimated in our study. Furthermore, two thirds of the RALP patients underwent nerve-sparing surgery compared to half of the patients operated RRP.
Our study has some limitations regarding length of follow-up for costs and effectiveness. Only short-term quality of life was measured and should be followed by assessment of quality of life-years ahead. Of the patients who had completed the SF-36, only one in five underwent RALP. Both questionnaires were handed out at baseline, where the patient filled out the first copy. At 6 months follow-up visit the patient was reminded to bring along the completed second questionnaire for the 1 year outpatient control visit. The low percentage for RALP patients filling in the second questionnaire may result in a biased estimate of QALY, if, for example, only the most dissatisfied RALP patients replied. On the other hand, the study by Schroeck et al. also found that patients who underwent RALP were most likely to be dissatisfied compared to RRPCitation10.
Even though the patients included in the present study are matched selection bias is not eliminated. First of all, our matched study is not comparable to randomised controlled trials due confounders such as unintended selection of procedure based on clinical T stages of disease and opportunity for nerve-sparing surgical technique. The clinical study in the present economic evaluation showed a higher share of recurrence in RRP patients indicating a higher risk at final pathology for patients undergoing RRP and that patients with lower tumour stage were predominantly selected to RALP. Secondly, QALY indicates a side-effect, and quality of life might be more crucial to patients operated by RALP compared with a quicker recovery of continence and erectile function. A randomised controlled trial with long-term follow-up of effectiveness and quality of life between RALP and RRP is therefore warranted along with standardised reporting of outcomesCitation28. At least better data on quality of life after RALP and RRP should be obtained.
We calculated the ICER per successful treatment with and without indirect costs. It is uncertain whether the decision makers find it relevant to include indirect costs. Furthermore, estimating absence from work is methodologically uncertain.
Two previous cost studies included the fixed costs for da Vinci basing the calculations on 300 RALP procedures yearly and a lifetime for the da Vinci robot of 7 yearsCitation3,Citation7. Additionally, the annual purchase and the maintenance costs for the da Vinci robot in the two studies were estimated to be lower; €807,800 and €72,629, respectivelyCitation3,Citation7. In our study the purchase was estimated to €1.4 million while the maintenance was €120,100 per year. Consequently, the costs for RALP are higher in our study.
Only one of the previous cost studies had made a sensitivity analysis showing that the costs for RALP are volume dependent where an increased volume of RALP demonstrated a reduction of the costs for RALPCitation7. Even though the present sensitivity analysis also showed that the costs for the RALP procedure decreased when increasing number of RALPs per week, it did not have influence of the assessment of cost effectiveness per successful treatment. Yet, even if RALP was used at the full capacity with three procedures per day, 5 days a week, the costs were still higher compared to RRP. Furthermore, the increased number of RALPs may decrease the life time of the da Vinci robot and the depreciation. The focus of improving the cost effectiveness may be to perform RALP at fewer centres with a high number of robot-assisted procedures, utilise the full potential of each robotic surgical system and increase the effectiveness of RALP.
Conclusions
It is uncertain whether the RALP procedure is cost effective. The incremental costs per extra successful procedure were €64,343. A long-term follow-up of the outcome measures and sick leave may intensify the assessment of the cost effectiveness between the two alternatives.
Transparency
Declaration of funding
No declaration of funding is to be declared.
Declaration of financial/other relationships
No financial or other financial relationship is to be declared.
Acknowledgment
We would like to thank Marianne Godt Hansen for English proofreading in the preparation of this article.
References
- Hu JC, Gu X, Lipsitz SR, et al. Comparative effectiveness of minimally invasive vs open radical prostatectomy. JAMA 2009;302:1557-64
- Burgess SV, Atug F, Castle EP, et al. Cost analysis of radical retropubic, perineal, and robotic prostatectomy. J Endourol 2006;20:827-30
- Lotan Y, Cadeddu JA, Gettman MT. The new economics of radical prostatectomy: cost comparison of open, laparoscopic and robot assisted techniques. J Urol 2004;172:1431-5
- The Danish National Board of Health. The Cancer Registry 2008. New figures from The Danish National Board of Health 2009:5. Table 9 [Internet] 2009. Available from: URL: http://www.sst.dk/publ/Publ2009/DOKU/cancerreg/cancerregisteret_2008.pdf. Danish
- The Danish National Board of Health. The Cause of Death Registry 2008. New figures from The Danish National Board of Health 2009:6. Table 5B; B-024 [Internet] 2009. Available from: URL: http://www.sst.dk/publ/Publ2009/DOKU/nye_tal/doedsaarsagsreg_2008.pdf. Danish
- Bolenz C, Gupta A, Hotze T, et al. Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer. Eur Urol 2010;57:453-8
- Scales CD, Jr., Jones PJ, Eisenstein EL, et al. Local cost structures and the economics of robot assisted radical prostatectomy. J Urol 2005;174:2323-9
- Barocas DA, Salem S, Kordan Y, et al. Robotic assisted laparoscopic prostatectomy versus radical retropubic prostatectomy for clinically localized prostate cancer: comparison of short-term biochemical recurrence-free survival. J Urol 2010;183:990-6
- Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol 2009;55:1037-63
- Schroeck FR, Krupski TL, Sun L, et al. Satisfaction and regret after open retropubic or robot-assisted laparoscopic radical prostatectomy. Eur Urol 2008;54:785-93
- Drummond MF, Sculpher M, Torrance G, et al. Methods for the Economic Evaluation of Health Care Programmes, 3rd edn. New York: Oxford University Press, 2005
- Ara R, Brazier J. Predicting the short form-6D preference-based index using the eight mean short form-36 health dimension scores: estimating preference-based health-related utilities when patient level data are not available. Value Health 2008;12:346-53
- D'Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998;280:969-74
- Skodborg G. Equipment costs per open retropubic radical prostatectomy and robot-assisted laparoscopic radical prostatectomy. Department of Urology, Surgical Ward, Aarhus University Hospital, Skejby, Denmark, 2009. Danish. Ref Type: Unpublished Work
- Balle K. Information of mean gross salary per year for employee at Aarhus University Hospital, Skejby, Denmark. Financial Department, Aarhus University Hospital, Skejby, Denmark, 2009. Danish. Ref Type: Unpublished Work
- The Central Denmark Region. Price list 2008. Aarhus University Hospital. 2008. The Central Denmark Region. Danish. Ref Type: Pamphlet
- Department of Transfusion Medicine. Price for blood transfusion. HR Department, Aarhus University Hospital, Skejby, 2009. Danish. Ref Type: Unpublished Work
- The Danish National Board of Health. The Danish National Registry of Patients, diagnosis related groups of in-patients. Ref Type: Data File
- Danish Medical Association. New figures for users of organisation of general practitioners. Average fee per consultation. Organisation of general practitioners [Internet] 2009. Available from: URL: http://www.laeger.dk/portal/page/portal/laegerdk/laeger_dk/politik/nyhedsbreve/nyhedsbreve_plo/nye_tal_fra_plo_brugere/gennemsnitligt%20honorar%20pr%20%20konsultation.pdf. Danish
- Abena A/S. Abri-San Normal. Diapers for adults, medium extent of urinary incontinence. Abena A/S [Internet] 2009.Available from: URL: http://913709.shop09.dandomain.dk/shop/abri-san-normal-4-311p.html. Danish
- SCA Hygiene Products A/S. Range of products. TENA for Men Level 1 og 2. SCA Hygiene Products A/S [Internet] 2009. Available from: URL: http://www.tenabutikken.dk/default.aspx?load=main&Data=ProductList&key=Tena%20for%20men. Danish
- Statistics Denmark. Earnings. [Internet] 2009. Available from: URL: http://www.statistikbanken.dk/statbank5a/default.asp?w=1280. Danish
- Financial and Public Authorities Department, Aarhus Municipality. Home visit by primary care nurse, price per hour. 2009. Ref Type: Unpublished Work
- Infomatum A/S. Medicin.dk. Infomatum A/S [Internet] 2009. Available from: URL: http://www.medicin.dk
- Intuitive Surgical. Information from the manufacture of the purchase and maintenance for the da Vinci® robotic surgical system. 2009. Ref Type: Unpublished Work
- Hohwü L, Akre O, Pedersen KV, et al. Open retropubic prostatectomy versus robot-assisted laparoscopic prostatectomy: a comparison of length of sick leave. Scand J Urol Nephrol 2009;43:259-64
- Eastham JA. Robotic-assisted prostatectomy: is there truth in advertising? Eur Urol 2008;54:720-2
- Murphy DG, Bjartell A, Ficarra V, et al. Downsides of robot-assisted laparoscopic radical prostatectomy: limitations and complications. Eur Urol 2010;57:435-46