
Abstract
Objective:
To descriptively analyze patient characteristics, treatment patterns, and medical resource use of individuals with diabetes mellitus (DM) with and without comorbid major depressive disorder (MDD).
Research design and methods:
Using an administrative claims database, commercially insured adults diagnosed with DM were studied over the calendar years 2005 and 2006. Demographic characteristics, comorbid illnesses, medication use, resource utilization, and costs were examined descriptively among patients with DM both with and without comorbid MDD.
Results:
Patients with DM and MDD were found to have a high resource burden, compared to patients with DM without MDD. Specifically, these patients were found to be more likely to be diagnosed with other comorbid medical conditions, to use multiple medications, and to use more healthcare services such as inpatient visits, emergency admissions, and outpatient visits. Consistent with these findings, costs for these patients were found to be $19,707 per year, compared to $11,237 for patients with DM without comorbid MDD.
Limitations:
The study utilizes data from an administrative claims database of insured individuals and hence, results may not be generalizable. Furthermore, the analysis is unable to examine clinical severity or indirect costs.
Conclusion:
Compared to patients with DM and no comorbid MDD, patients with DM and MDD tend to have a larger burden of disease and to use more healthcare resources.
Introduction
Diabetes is recognized as one of the leading causes of death and disability across geographies. Worldwide, the number of adults with diabetes was estimated to be 171 million in 2000 and is expected to rise to 366 million by the year 2030Citation1. In the United States, the prevalence of diagnosed DM among adults aged 18 years and over has increased steadily over the past decade, from 5.1% in 1997 to 10.1% in early 2009Citation2. The estimated cost of DM in the US has also risen steadily, from $98 billion in 1997Citation3 to an estimated $174 billion in 2007Citation4. These cost estimates represent both direct medical expenditures and indirect costs such as lost productivity.
Patients with DM are vulnerable to severe, long-term complications, including kidney failure, blindness, lower limb amputations, heart disease, and strokeCitation5. In addition to these physical complications, individuals with DM are also at increased risk for mental health disorders, particularly depressionCitation6,Citation7. Relative to non-diabetic individuals, persons with diabetes are 50%Citation8 to 60% more likelyCitation9,Citation10 to have a diagnosis of depression, and some research has indicated that they are also twice as likely to have depression serious enough to warrant treatmentCitation6. Concurrent diagnoses of depression and diabetes have been shown to be associated with poor metabolic control, decreased quality of lifeCitation11–13, and higher medical costsCitation8,Citation9,Citation13,Citation14.
Given the risk of poor outcomes for patients with DM and comorbid major depressive disorder (MDD), this study descriptively analyzed and compared demographic characteristics, treatment patterns, and medical resource use of patients with DM with and without MDD. This research can help identify patients who may be at risk for comorbid MDD and DM so that these patients can be targeted for specific interventions to avoid many of the sequelae that are associated with the co-occurrence of these conditions. This research will also provide a better understanding of the resource and cost impact of comorbid depression among a population of patients with diabetes.
Methods
The MedStat MarketScan Commercial Claims and Encounters (CCE) and Medicare Supplemental and Coordination of Benefits databases form the basis for these analyses. The CCE database includes private sector health data, while the Medicare database contains data for Medicare-eligible retirees with employer-sponsored Medicare Supplemental plans. Both databases are fully Health Insurance Portability and Accountability Act (HIPAA) compliant and link paid claims and encounter data to detailed patient information across sites and types of providers over time.
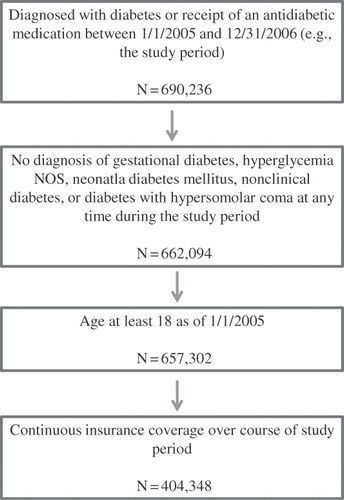
The study population included patients with diabetes who had continuous pharmaceutical and medical insurance coverage between January 1, 2005 and December 31, 2006. In addition to continuous coverage, eligibility required individuals to have either a diagnosis code for type 1 or type 2 diabetes (ICD-9 codes 250.xx) or to have a filled prescription for an antidiabetic agent during the 2-year study period. Patients were excluded if, during the study period, they were under 18 years of age or were diagnosed with gestational diabetes (ICD-9-CM of 648.8x), hyperglycemia not otherwise specified (ICD-9-CM of 251.2x), neonatal diabetes mellitus (ICD-9-CM of 775.1), nonclinical diabetes (ICD-9-CM of 790.29), or diabetes with hyperosmolar coma (ICD-9-CM of 250.2). Given these inclusion and exclusion criteria, the study sample consisted of 404,348 individuals identified as having DM. This group was subdivided into those patients with (n = 5826) and without (n = 398,522) MDD, defined as individuals with a diagnosis code for major depressive disorder (ICD-9 codes 296.2, 296.20–296.26, 296.3, 296.30–296.36) during the study period. illustrates the effect of the inclusion and exclusion criteria on the sample size.
Figure 1. Inclusion – exclusion criteria and sample size.
The analysis examined demographic characteristics, comorbid illness, medication use, resource use, and medical and pharmaceutical costs of the study populations over a 2-year period. Patient characteristics examined included age, sex, region of residence, type of insurance coverage, and the Charlson Comorbidity Index score, constructed for each patient based on medical history assessed using ICD-9-CM codes on patients’ administrative claimsCitation15,Citation16. Major comorbidities were categorized on the basis of the major subsections (e.g., infectious and parasitic diseases) of the ICD-9-CM coding manualCitation17 (2009 Physicians’ Professional ICD-9-CM), while annualized drug class utilization examined the use of specific classes of antidepressants as well as antidiabetic medications. Healthcare utilization assessed annualized hospital, emergency room (ER), outpatient, and total visits and was sub-divided into depression-related, diabetes-related, other, and total healthcare utilization. Annualized medical costs were subdivided into depression-related, diabetes-related, other, total, inpatient, outpatient, ER, and pharmacy. All analyses are descriptive in nature. Differences in continuous variables were examined using t-statistics, while differences in categorical variables were examined using chi-square statistics. All analyses were performed using SAS, Version 9.1 (Cary, NC, USA).
Results
In this study, only 1.4% of patients identified as having DM were also identified as having comorbid MDD. examines the patient characteristics for patients with DM with and without MDD. The majority of these patients were female (53.4%) and the mean (SD) age was 62 (12.7) years. Patients with DM, both with and without MDD, were most commonly insured with comprehensive insurance or a preferred provider organization. Results revealed that a higher proportion of patients in the MDD subgroup were female (63.7 vs. 46.3%; p < 0.0001), and that those with MDD were generally younger (mean age 57.7 vs. 62.2 years; p < 0.0001) than those without MDD.
Table 1. Patient characteristics.
Examining comorbid conditions between the two subgroups () revealed that DM patients with MDD had a slightly higher overall comorbid burden (mean [SD] Charlson Comorbidity Index score of 2.6 [1.98] vs. 2.3 [1.91]; p < 0.0001), and higher rates of many categories of comorbid conditions compared to patients without comorbid MDD. For example, those with DM and MDD were more likely to be diagnosed with diseases of the digestive system (46.8 vs. 32.8%; p < 0.0001), genitourinary system (55.3 vs. 41.9%; p < 0.0001), musculoskeletal system (76.8 vs. 61.2%; p < 0.0001), and respiratory system (63.5 vs. 49.0%; p < 0.0001).
Table 2. Comorbidities.
presents annualized outpatient prescription medication usage by drug class. These results reveal that the vast majority of patients with concurrent diagnoses of DM and MDD received at least one pharmacotherapy (97.5%), with 93% being prescribed at least one antidepressant; 33.7% were prescribed insulin, and 63.7% prescribed a noninsulin antidiabetic agent. The most commonly prescribed classes of antidepressants were selective serotonin reuptake inhibitors (SSRIs) (64.0%) and selective serotonin norepinephrine reuptake inhibitors (SSNRIs) (34.9%), while the most commonly prescribed noninsulin antidiabetic agents were thiazolidinediones (37.6%) and sulfonylureas (37.4%). Not surprisingly, a comparison of those patients with DM and MDD to those with DM without MDD revealed a higher proportion of patients with comorbid MDD were prescribed antidepressants (93.0 vs. 25.5%; p < 0.0001). Patients with DM and MDD were also more frequently prescribed insulin (33.7 vs. 26.8%; p < 0.0001) relative to patients with DM and no diagnosis of MDD. In contrast, a slightly higher proportion of patients with DM without comorbid MDD were prescribed a noninsulin antidiabetic agent (68.8 vs. 63.7%; p < 0.0001), with the most common classes of noninsulin medications prescribed being sulfonylureas (42.6 vs. 37.4%; p < 0.0001) and thiazolidinediones (38.6 vs. 37.6%; p = 0.1141).
Table 3. Annualized drug class utilization.
presents annualized healthcare utilization rates and frequency of use. The DM with MDD and DM, compared to patients without comorbid MDD cohorts, had significantly higher number of annual inpatient (0.8 vs. 0.6; p = 0.0003) and outpatient visits (4.7 vs. 3.9; p < 0.0001). Patients with DM and MDD were significantly more likely to have had at least one diabetes-related ER visits (5.6 vs. 3.5%), inpatient visit (2.5 vs. 1.5%; p < 0.0001) or outpatient visit (96.4 vs. 94.1%; p < 0.0001) than patients with DM and no MDD. In addition, the DM with MDD cohort had a higher percentage of individuals with an inpatient admission (37.1 vs. 26.7%; p < 0.0001), ER visit (56.7 vs. 39.8%; p < 0.0001), or outpatient visit (99.5 vs. 98.5%; p < 0.0001)for other causes. Overall, a higher percentage of patients with DM and MDD used services for all reasons combined and had more visits per service than DM patients with MDD.
Table 4a. Resource utilization – frequency of use.
Finally, presents annualized, direct medical and pharmaceutical costs. Patients with DM and MDD, compared to those without comorbid MDD, had higher diabetes-related costs ($781.4 vs. $54.0; p < 0.0001). Consistent with the findings of more comorbidities, higher medication use, and higher resource utilization among patients with DM and comorbid MDD, other costs were also significantly higher for patients with DM and comorbid MDD compared to those without MDD ($18,108.3 vs. $10,727.7; p < 0.0001). In addition, with the exception of diabetes-related inpatient costs, all component costs were significantly higher for patients with DM and comorbid MDD. These differences in component costs resulted in a significant difference in total costs between the two groups. Overall, total annualized healthcare costs were $8470 greater for the DM with MDD cohort than for the DM without MDD cohort. For patients with DM and MDD, results revealed the mean annual cost per patient with DM and MDD was $19,707, compared to a similar cost of $11,237 for patients with DM and no comorbid depression (p < 0.0001). Only about 10% of the costs for the DM and MDD cohort were directly attributable to MDD.
Table 4b. Resource utilization - mean use.
Table 5. Annualized healthcare costs – among users of service.
Discussion
This study provides a descriptive analysis of the demographic characteristics, treatment patterns, and medical resource usage of a population of patients with diabetes mellitus concurrent with major depressive disorder. For comparison purposes, this research also provided a descriptive analysis of those characteristics among a population of patients with DM but without a diagnosis of MDD. Several notable findings were uncovered. First, as is true in the general population and in agreement with previous research from observational studies, the patients in our sample with depression were more likely to be femaleCitation6,Citation14,Citation18,Citation19 and youngerCitation14,Citation19 relative to their counterparts without MDD (see ). It has been hypothesized that biological, life cycle, hormonal and psychosocial factors may all be associated with women's higher depression ratesCitation20. Specifically, women may have depression associated with premenstrual disorder, are vulnerable to depression after giving birth, and often face additional stressed of work and home responsibilitiesCitation20. Furthermore, women are more likely to experience sexual or physical abuse than men and such abuse has been found to be associated with depressionCitation21. The association between younger age and depression among individuals with diabetes has been hypothesized to be associated with the fact that younger adults are more likely to have adolescent onset diabetes, which may be linked to depression due to the complications of diabetes when adapting to puberty, peer-group pressure, and identity formationCitation22. Alternatively, younger patients are more likely to have type 1 diabetes and it is possible that the more complex treatment regimen associated with type 1 diabetes compared to type 2 diabetes in younger patients may increase the risk of depressionCitation22.
Also consistent with previous findingsCitation23–25, diabetic patients with comorbid MDD in this sample had a greater comorbid burden (see ). Seemingly at odds with previous research reporting that major depression affects 15–20% of patients with diabetes and 2–9% of the general populationCitation6,Citation26, only 1.5% of diabetic patients in this sample were also diagnosed with MDD (see ). However, it should be noted that these studies did not rely on administrative claims databases to identify comorbid depression. Research has shown that depression may be under-identified by cliniciansCitation27 and may also be mislabeled or under-reported due to the stigma of mental illnessCitation28. In addition, this analysis relied solely on diagnostic codes and antidepressant use was not considered to be indicative of a diagnosis of MDD, given the high prevalence of the prescribing of antidepressants for other conditionsCitation29. A richer dataset, including formal diagnostic assessments, would be needed for more comprehensive identification of persons with major depressive disorder.
Not surprisingly, and in agreement with previous researchCitation14, antidepressant use was more prevalent among diabetics with MDD (93.0 vs. 25.5%). Interestingly, over one-quarter of the patients without a diagnosis of MDD used antidepressants, indicating that patients in this sample may have been getting treated for depression without a formal diagnosis of MDD. Alternatively, it may indicate that patients were prescribed antidepressants to treat conditions other than depression. Research has shown that antidepressants are often prescribed in the absence of depression to control various medical conditions, including epileptic seizures, pain associated with post-herpetic neuralgiaCitation29, or the pain of diabetic neuropathyCitation30,Citation31. Indeed, a previous study found antidepressant use among 24% of diabetic patients with neuropathy but not MDDCitation14.
In addition to being more likely to use an antidepressant, diabetic patients with a diagnosis of MDD were more likely to use insulin and less likely to use an oral antidiabetic agent. This finding supports previous evidence of an association between comorbid depression and poorer metabolic control among patients with diabetesCitation13,Citation32,Citation33. Alternatively, this association may be due to a worse severity of DM among patients with MDD.
Patients with comorbid MD, relative to their diabetic counterparts without MDD, had larger non-diabetes-related costs. More specifically, more of those with comorbid MDD had one or more inpatient and ER visits and use of antidepressants than those with MDD (inpatient: 40 vs. 27%, p < 0.0001; ER: 57 vs. 40%, p < 0.0001; antidepressant: 93 vs. 26%, p < 0.0001). Moreover, among the patients who had an inpatient or ER visit, the mean cost of that visit was higher among those diagnosed with MDD (inpatient: $11,275 vs. $9433, p < 0.0001; ER: $692 vs. $443, p < 0.0001). For those using antidepressants, the mean cost of antidepressant use was higher among those with comorbid MDD ($1078 vs. $410; p < 0.0001). These results suggest that the treatment of patients with DM and comorbid MDD is complicated and costly, even when compared to those who have DM but no diagnosis of MDD. These results confirm previous research, which has found worse outcomesCitation34, greater healthcare utilizationCitation35, and higher costsCitation8,Citation9,Citation13,Citation14 to be associated with a diagnosis of comorbid depression among individuals with diabetes.
The findings presented in this paper should be interpreted in the context of the limitations of the study design. First, this research was conducted using an administrative claims database and included only patients with medical and prescription benefit coverage; therefore, the results may not generalize well to other populations. Second, the use of diagnostic codes to identify individuals is not as rigorous as formal diagnostic assessments for identifying people with diabetes or major depressive disorder. Third, detailed clinical information required for adjustment on the basis of diabetes history and/or severity was not available; thus, differences observed cannot be attributed directly to depression. Finally, this analysis focused exclusively on direct medical costs associated with a diagnosis of diabetes mellitus with and without comorbid depression; it did not include an assessment of indirect medical costs (e.g., lost patient and caregiver productivity costs) or other important non-economic outcomes (e.g., quality of life).
Conclusions
The results of this retrospective, descriptive analysis support the body of evidence related to patients with DM and MDD, evidence which indicates that these patients tend to have a large burden of comorbidity, healthcare utilization, and healthcare costs. Given the high mean cost of an inpatient hospitalization among patients with DM and MDD, future analyses should further refine the identification of patient characteristics of those with comorbid MDD and DM and examine whether interventions to manage the complexity of these co-occurring conditions may prove cost-effective as well as improve patient outcomes. The results presented here suggest that physicians treating patients with DM should strongly consider also monitoring for depression, and disease management programs should consider including screening and treatment for both DM and MDD.
Transparency
Declaration of funding
This paper was sponsored by Eli Lilly and Company.
Declaration of financial/other relationships
All co-authors are employees of Eli Lilly and Company and this project was completed as part of their employment.
References
- World Health Organization. Diabetes programme. Available at http://www.who.int/diabetes/facts/world_figures/en/ [Last accessed 18 October 2010]
- Centers for Disease Control and Prevention/National Center for Health Statistics. National health interview survey, 1997–March 2009. Available at http://www.cdc.gov/nchs/data/nhis/earlyrelease/200909_14.pdf. [Last accessed 18 October 2010]
- American Diabetes Association. Economic consequences of diabetes mellitus in the U.S. in 1997. Diabetes Care 1998;21:296-309
- National Diabetes Information Clearinghouse (NDIC). Diabetes overview. http://www.diabetes.niddk.nih.gov. Updated November 2008. Accessed October 17, 2009
- Morgan CL, Currie CJ, Stott NC, et al. The prevalence of multiple diabetes-related complications. Diabetic Medicine 2003;17:146-51
- Anderson RJ, Freedland KE, Clouse RE, et al. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2001;24:1069-78
- Lustman PJ. Anxiety disorders in adults with diabetes mellitus. Psychiatr Clin North Am 1998;11:419-32
- Egede LE, Zheng D, Simpson K. Comorbid depression is associated with increased health care use and expenditures in individuals with diabetes. Diabetes Care 2002;25:464-70
- Finkelstein EA, Bray JW, Chen H, et al. Prevalence and costs of major depression among elderly claimants with diabetes. Diabetes Care 2003;26:415-20
- Nichols GA, Brown JB. Unadjusted and adjusted prevalence of diagnosed depression in type 2 diabetes. Diabetes Care 2003;26:744-9
- Wagner JA, Tennen H. History of major depressive disorder and diabetes outcomes in diet- and tablet-treated post-menopausal women: a case control study. Diabetic Med 2007;24:211-16
- Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med 2000;160:3278-85
- Gary TL, Crum RM, Cooper-Patrick L, et al. Depressive symptoms and metabolic control in African-Americans with type 2 diabetes. Diabetes Care 2000;23:23-9
- Le TK, Able SL, Lage MJ. Resource use among patients with diabetes, diabetic neuropathy, or diabetes with depression. Cost Eff Resour Alloc 2006;4:18
- Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 1992;45:613-19
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373-83
- Physicians’ Professional ICD-9-CM. Salt Lake City, UT: Medical Management Institute, 2008
- Parker G, Hadzi-Pavlovic D. Is the female preponderance in major depression secondary to a gender difference in specific anxiety disorders? Psychol Med 2004;34:461-70
- Egede LE, Zheng D. Independent factors associated with major depressive disorder in a national sample of individuals with diabetes. Diabetes Care 2003;26:104-11
- National Institute of Mental Health. Depression: how do women experience depression? Available at http://www.nimh.nih.gov/health/publications/depression/complete-index.shtml. Accessed May 6, 2011
- Dube SR, Anda RF, Whitfield CL, et al. Long-term consequences of childhood sexual abuse by gender of victim. Am J Prev Med 2005;28:430-8
- Zhao W, Chen Y, Lin M, et al. Association between diabetes and depression: Sex and age differences. Public Health 2006;120:696-704
- Clouse RE, Lustman PJ, Freedland KE, et al. Depression and coronary heart disease in women with diabetes. Psychosom Med 2003;65:376-83
- de Groot M, Anderson RJ, Freedland KE, et al. Association of depression and diabetes complications: a meta-analysis. Psychosom Med 2001;63:619-30
- Peyrot M, Rubin RR. Levels and risks for depression and anxiety symptomatology among diabetic adults. Diabetes Care 1997;20:585-90
- Gonzalez JS, Safren SA, Cagliero E, et al. Depression, self-care, and medication adherence in type 2 diabetes: relationships across the full range of symptom severity. Diabetes Care 2007;30:2222-7
- Jencks SF. Recognition of mental distress and diagnosis of mental disorder in primary care. JAMA 1985;253:1903-7
- Rost, K, Smith, GR, Matthews, DB, et al. The deliberate misdiagnosis of major depression in primary care. Arch Fam Med 1994;3:333-42
- Chen H, Reeves JH, Fincham JE, et al. Off-label use of antidepressant, anticonvulsant, and antipsychotic medications among Georgia Medicaid enrollees in 2001. J Clin Psychiatr 2006;67:972-82
- Poncelet AN. Diabetic polyneuropathy: risk factors, patterns of presentation, diagnosis, and treatment. Geriatrics 2003;58:16-30
- Goodnick PJ. Use of antidepressants in treatment of comorbid diabetes mellitus and depression as well as in diabetic neuropathy. Ann Clin Psychiatr 2001;13:31-41
- Lustman PJ, Williams MM, Sayuk GS, et al. Factors influencing glycemic control in type 2 diabetes during acute- and maintenance-phase treatment of major depressive disorder with bupropion. Diabetes Care 2007;30:459-66
- Lustman PJ, Anderson RJ, Freedland KE, et al. Depression and poor glycemic control: a meta-analytic review of the literature. Diabetes Care 2000;23:934-42
- Black SA, Markides KS, Ray LA. Depression predicts increased incidence of adverse health outcomes in older Mexican Americans with type 2 diabetes. Diabetes Care 2003;26:2822-8
- Vamos EP, Mucsi I, Keszei A, et al. Comorbid depression is associated with increased healthcare utilization and lost productivity in persons with diabetes: a large nationally representative Hungarian population survey. Psychosom Med 2009;71:501-7