
Abstract
Introduction:
Selection of antihypertensive therapy hinges on an appropriate combination of efficacy, tolerability and compatibility with co-morbidities. Within a given class of antihypertensives, the choice of agent is often driven by cost, with the cheapest appropriate agent being chosen. Amongst the angiotensin receptor blockers (ARBs), this choice will often be losartan, as it is available in generic form. However, as the blood pressure lowering efficacy of losartan is modest, some patients will require an alternative ARB. In the UK this choice is often candesartan, although the agent with greatest BP lowering efficacy is olmesartan. The objective of this study was to use a cost-benefit model to compare the costs associated with target achievement using each of these two agents, in order to guide optimum use of prescribing budgets.
Method:
A probabilistic cost-benefit model was constructed for a cohort of patients with moderate hypertension, based on a standardised titration and maintenance algorithm using either olmesartan or candesartan, combined with thiazide and calcium channel blocker where required. Direct treatment costs were recorded, along with the proportion of patients achieving pre-defined treatment targets at each treatment level. Results were expressed as mean treatment cost per patient reaching target.
Results:
Based on the current QoF target of 150 mmHg systolic, 94.3% of patients on the olmesartan-based regimen reached target of 150 mmHg, compared with 89.0% of those on the candesartan-based regimen. 86% of olmesartan patients reached target on <3 drugs, compared with 74% of candesartan patients. The mean 12-month cost per patient reaching target was £171.36 for olmesartan versus £189.91 for candesartan. Ongoing annual maintenance costs for patients at target were £169.97 and £182.64, respectively. Similar results were obtained when considering alternative treatment targets
Limitations:
The study only compared two ARBs – candesartan and olmesartan and the results relate to prescribing costs only and do not include other healthcare costs. Additionally, the chosen outcome was blood pressure target achievement, rather than clinical endpoints. Given the stated objectives of the model, we do not believe these issues will have introduced bias in the direction of either comparator
Conclusion:
Although olmesartan has an apparently higher acquisition cost than candesartan, its superior BP lowering efficacy means that the overall cost per patient treated to target is actually lower. This result could have significant implications for making savings within primary care prescribing budgets in the UK.
Introduction
The effective management of hypertension constitutes one of the key components of an integrated cardiovascular risk management strategy and is generally predicated on the achievement of a predetermined blood pressure targetCitation1–3. While the level at which this target is set will vary according to the age and pattern of comorbidities of the individual patient, there is general agreement that what matters most to the clinical outcome is the degree of blood pressure lowering achieved, rather than the specific pharmacological agent used to achieve itCitation4. There may be circumstances where a particular class of agent is preferred – a renin angiotensin agent in diabetes for instance – but within a given class distinctions are rarely made on efficacy grounds, cost being a more frequent discriminator.
For most classes of antihypertensive – thiazides, beta-blockers, ACE inhibitors and calcium channel blockers (CCB) – the majority of agents are out of patent protection and available as low-cost generics; in these cases, the choice of agent carries little cost consequence. In the case of angiotensin receptor blockers (ARB), however, only one agent – losartan – is currently available as a generic, with the remaining agents still being marketed as patented products. This means there are significant cost differences associated with the treatment choice made for ARBs ().
From a pure cost-minimisation viewpoint, it is clear that the agent of choice in patients requiring treatment with an ARB should be losartan. However, the prescription data show that only around one in four ARB prescriptions currently issued in England fact for losartan. This may, in part, reflect historical patterns of prescription. Until losartan went off patent in late 2009, it was one of the most expensive ARBs and therefore its use was discouraged by PCTs and candersartan, which had a cheaper acquisition cost was widely used, a pattern reflected in the prescribing data shown in . Inevitably, a switch in treatment recommendation is associated with a significant lag time before it is widely adopted and we may therefore anticipate a change in the observed pattern in the future.
An additional explanation, however, may lie with differing patterns of blood pressure lowering efficacy. Across the range of doses commonly used for the treatment of hypertension, there are differences in the extent to which the various ARBs typically lower blood pressure, with losartan having the lowest mean effect of the commonly used agents ()Citation7.
Figure 1. Placebo corrected mean effect of ARBs on diastolic blood pressure (reproduced with permission from Zannad et al.Citation7).
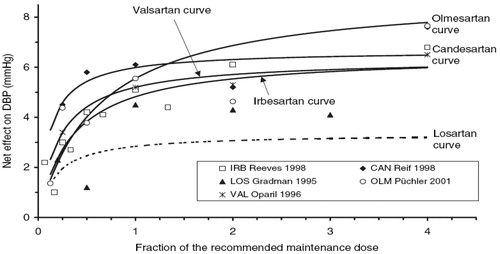
Whilst the BP lowering effect of losartan is likely to be sufficient for many patients with mildly elevated blood pressure, for those with more significant degrees of hypertension, it may prove ineffective. A proportion of those patients prescribed other ARBs are likely to fall into this group.
The decision as to which ARB offers the lowest cost option in this circumstance is complex. The objective of hypertension management is the target achievement, with dosage being titrated and additional agents being added in order to reach a pre-determined goal. The cost of treatment will therefore be determined not by the simple acquisition cost of any individual preparation, but by the overall expenditure required to reach target. This expenditure will be the product of treatment efficacy at any given dose level, coupled with dose-specific costs.
We therefore set out to design a cost-benefit model linked to a target-driven hypertension treatment algorithm. The objective was to compare the mean cost per patient achieving treatment target using either a candesartan-based regimen (the most commonly prescribed ARB) or an olmesartan-based regimen (the ARB with the greatest BP lowering efficacy at normally prescribed doses).
Methods
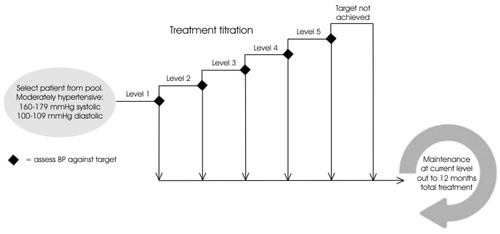
A cost-benefit model was constructed to explore the impact of two different treatment regimens on a cohort of patients with untreated moderate hypertension (starting BP 160–179/100–109 mmHg). The approach combined a decision tree element to simulate the treatment titration phase, followed by an iterative maintenance phase (). The perspective of the model was the NHS in the UK over a period of 12 months, with costs reflecting the direct costs of drug treatment only and benefits the proportion of treated patients reaching one of two pre-specified treatment targets.
Figure 2. Schematic representation of cost–benefit model.
Model flow
The parent cohort of patients was created using systolic and diastolic blood pressures normally distributed about mean values of 170 mmHg and 105 mmHg, respectively, such that 95% of the population had blood pressure values within the range stated above. As there was no expectation of a differential effect of the two drugs in different patient sub-classes, age, sex, co-morbidity and prior treatment were not incorporated into the baseline characteristics of the sample population.
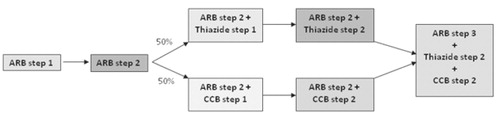
Individual patients were selected from the parent cohort on a probabilistic basis, each selected individual being fed through both olmesartan and candesartan arms simultaneously. Transition between each step of the titration phase was determined according to a pre-specified treatment algorithm ().
Figure 3. Treatment algorithm. ARB step 1: Olmesartan 10 mg/candesartan 8 mg ARB step 2: Olmesartan 20 mg/candesartan 16 mg ARB step 3: Olmesartan 40 mg/candesartan 32 mg Thiazide step 1: Hydrochlorothiazide 12.5 mg/bendroflumethiazide 2.5 mg Thiazide step 2: Hydrochlorothiazide 25 mg/bendroflumethiazide 5 mg CCB step 1: Amlodipine 5 mg CCB step 2: Amlodipine 10 mg.
Target achievement at each step was determined by subtracting the BP lowering efficacy of the specific therapy/dose combination (see below) from the baseline blood pressure of the individual patient. In order to reflect normal between-patient variation, the absolute value of the BP lowering efficacy was varied probabilistically for each patient across the 95% confidence interval of the estimate. Where patients failed to reach target, even at level 5 of the titration schedule, they were classified for the purposes of the model as a ‘target failure’ and assigned to a nominal ‘level 6’.
The model was run for two different targets. NICE guidelines recommend treating uncomplicated hypertensive patients to a target of 140/90 mmHgCitation1. The UK Quality Outcomes Framework (QoF) recommends a target of 150/90, which therefore tends to be more widely implemented in UK primary careCitation3. We therefore assessed the outcome of the model for:
Systolic target of 150 mmHg
Systolic target of 140 mmHg
Diastolic target of 90 mmHg
Once the chosen target had been achieved in the titration phase, it was assumed that both treatment and blood pressure would remain unaltered for the remainder of the 12-month assessment period. Although, in the real world, poor adherence, adverse events and concomitant disease would tend to conspire to make this an unrealistic scenario, there is no evidence to suggest that these factors would operate any differently in an olmesartan-treated patient than in one treated with candesartan. For the purposes of this analysis, therefore, these factors can be safely ignored.
Treatment efficacy
There are no direct comparative studies that allow us to generate efficacy results for both olmesartan and candesartan-based regimens. The estimates are therefore based on indirect comparisons (). In the case of the magnitude of effect for the ARB alone or in combination with thiazides, these efficacy estimates are based on the results of published integrated analyses of factorial studiesCitation8,Citation9. In the case of add-on therapy with amlodipine, data exist for both agents to prove the benefit in prinicipleCitation10,Citation11, but the range of doses evaluated in the candesartan study was insufficient to provide the information required for this model. We therefore took the incremental blood pressure lowering associated with each dose of amlodipine in the olmesartan studyCitation10 and applied these values to the baseline efficacy for each ARB equally. A similar approach was adopted for step 5, where data on triple therapy only exist for olmesartanCitation11. In this case, the incremental effect associated with amlodipine from this study was applied to the BP lowering efficacy of both ARBs + thiazide from the factorial studies.
Table 2. Estimates of dose-specific BP lowering efficacyCitation8–10,Citation12.
In all cases, estimates of standard error derived from the studies were used to generate 95% confidence intervals for the purposes of probabilistic sampling within the model.
Costs
Costs for all treatments were drawn from the March 2011 edition of the Drug Tariff and the March 2011 edition of the British National FormularyCitation5,Citation13. Where single-tablet combinations existed and were cheaper than the equivalent items prescribed separately, these were used. Hydrochlorothiazide is not available as a separately prescribable generic item in the UK, but only as a component of single-tablet combinations. Conventional practice is to use an alternative agent – typically bendroflumethiazide 2.5–5 mg, which has been shown to be therapeutically equivalent to hydrochlorothiazide 12.5–25 mgCitation14. The model was priced accordingly.
Where patients failed to achieve target, it was assumed that additional unspecified treatments were used to achieve control. Although this level of management was not explicitly modelled, an additional ongoing cost of level 5 + 25% was assigned for the remainder of the 12-month period.
All treatments were costed over 12 × 28-day periods. As the time horizon did not extend beyond 1 year, no discounting was applied.
Outputs
Estimates of mean cost and target achievement rates were assessed by means of 1 million Monte Carlo microsimulations through each treatment arm, carried out using TreeAge Pro 2009. For each of the three treatment targets explored, results are presented for:
Number of patients achieving target
Number of patients at each titration level
Mean expenditure in each treatment group
Cost–benefit ratio (£/patient to target) for each treatment group
Threshold analyses were carried out to assess the point at which uniform modifications to either efficacy or cost estimates would have achieved equality of outcomes in all three models.
Results
Target achievement
94.3% of patients on the olmesartan-based regimen achieved a systolic treatment target of 150 mmHg, compared with 89.0% of those on the candesartan-based regimen. Similarly, 99.8% of olmesartan-treated patients achieved the diastolic target of 90 mmHg, compared with 92.2% of candesartan-treated patients. For the much more challenging systolic target of 140 mmHg, only 49% of candesartan patients reached this goal, compared with 65.5% of those on olmesartan.
The distribution of patients across the titration levels for each of the models is shown in and . Thanks to its greater blood pressure lowering efficacy, there is a clear trend for patients in the olmestartan arm to be reach target at a lower stage in the titration process. For each of the three targets evaluated, there are more olmesartan-treat patients adequately controlled on one drug and fewer requiring treatment with three or more drugs, than is the case for candesartan. Given that increasing dosage and complexity of drug regimen is also associated with increasing cost, this is likely to have a significant effect on the other half of the cost benefit equation.
Figure 4. Numbers of treatments required to reach targets: broken down by ARB and target used.
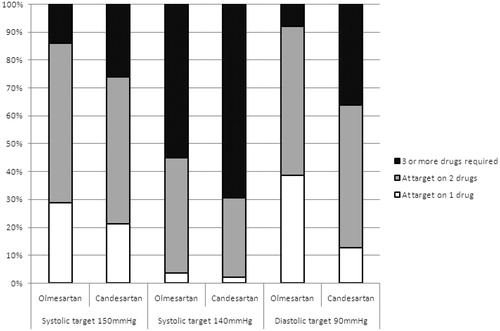
Table 3. Distribution of patients across titration levels.
Cost
Mean expenditure reflected both treatment costs incurred in the titration process and the ongoing costs of maintenance therapy. It is the maintenance costs that are potentially of more relevance in the estimation of long-term ongoing costs, so in , nominal ongoing annual cost at the final dose arrived at in the model is also listed. It will be seen that, as for the target achievement data, the costs associated with olmesartan-based treatment are lower than those of candesartan-based treatment, regardless of the target used.
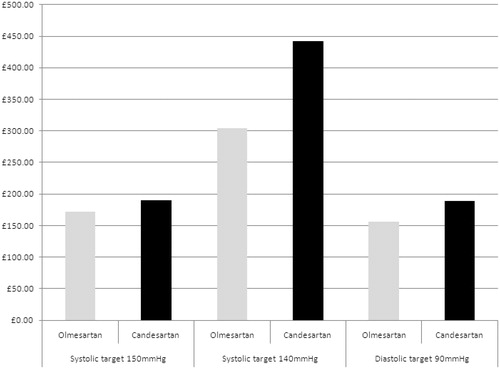
Table 4. Mean estimated 12-month costs per patient + mean cost per patient to target.
Cost benefit
Given that both target achievement and cost outcomes favour the olmesartan-based regimen, it is unsurprising that the cost–benefit ratios also point in the same direction ( and ). The magnitude of difference varies, but appears to be at its greatest for the most challenging target – a systolic BP of 140 mmHg.
Figure 5. Mean cost per patient to target broken down by ARB and target used.
Threshold analyses
It is debatable whether conventional statistical tests of significance have any real meaning in the context of this type of economic modelling, as the results are multimodal rather than normally distributed. What is probably of more practical value is to quantify the magnitude of change required to key variables, in order to be sufficient to remove the observed differences.
There are only two variables of any consequence in this model:
Drug cost
ARB efficacy
Drug cost
The cost of the ARB to the NHS is within the control of the pharmaceutical company, and therefore it is legitimate to explore what magnitude of discount on the price of candesartan would be required to bring the incremental cost–benefit ratio versus olmesartan down to zero.
Assuming that all costs other than candesartan remained unaltered:
In order to equal the cost benefit of olmesartan in the systolic 150 mmHg target model, the price of all strengths of candesartan would need to be reduced by 11%
In order to equal the cost benefit of olmesartan in the systolic 140 mmHg target model, the price of all strengths of candesartan would need to be reduced by 35%
In order to equal the cost benefit of olmesartan in the diastolic 90 mmHg target model, the price of all strengths of candesartan would need to be reduced by 19%
ARB efficacy
Clearly the efficacy of a given ARB is not amenable to change. However, it is possible that the estimates that we have used – which are derived from clinical trials – are not truly representative of the blood pressure lowering that can be obtained in clinical practice. Therefore, in addition to the probabilistic exploration of individual patient response, we also carried out a threshold analysis to answer the question: by how much would the blood pressure lowering efficacy have to be higher than our estimate, in order to match the cost–benefit ratio of olmesartan?
It would be neither practical nor informative to explore each efficacy data point individually. We therefore increased the efficacy of all strengths of candesartan incrementally, while leaving the olmesartan arm unaltered, until the cost-benefit results coincided.
In order to equal the cost benefit of olmesartan in the systolic 150 mmHg target model, the global efficacy of candesartan would have to be 9% higher than our estimates
In order to equal the cost benefit of olmesartan in the systolic 140 mmHg target model, the global efficacy of candesartan would have to be 12% higher than our estimates
In order to equal the cost benefit of olmesartan in the diastolic 90 mmHg target model, the global efficacy of candesartan would have to be 23% higher than our estimates
Discussion
In this analysis we have demonstrated that, in patients with moderate hypertension initiating treatment with an ARB-based regimen, olmesartan is associated with lower drug acquisition costs than candesartan per patient brought to treatment target. Although this may seem at odds with the apparently lower basic NHS price for candesartan, the superior blood pressure lowering efficacy of olmesartan means that patients can achieve targets on lower mean doses of antihypertensive than those required with candesartan and therefore incur lower mean costs.
Furthermore, assuming that the patient’s need for therapy remains relatively unaltered in the medium term, the potential for an ongoing saving exists, as our analysis has suggested that effective maintenance therapy is possible using lower doses of olmesartan than candesartan and a lesser requirement for add-on therapy.
ARBs accounted for around £330 million expenditure in the UK in 2009/10, of which around £85 million was for candesartanCitation15–18. Some of these patients have no compelling reason for being on an ARB at all and could be comfortably switched to an ACE inhibitor at a substantial saving and to no clinical detriment. Others of them, with lesser degrees of hypertension, could legitimately be switched to losartan. However, there will be nonetheless a proportion of patients in this group who have a clear indication for an ARB and genuinely require a more effective agent than losartan. It is this group, in whom in addition to the substantial year 1 savings, the opportunity exists to reduce ongoing expenditure by up to £30 per patient per year that warrants serious consideration of a switch of strategy.
Clearly, as drug acquisition prices are not constant, the results of this model will only be valid for a limited period of time and within the UK (see ). Before extrapolating these results to other circumstances, due allowance should be made for potential differences.
Study limitations
The scope of this study was to assess the budgetary impact of ARB choice and was therefore limited to assessing direct drug acquisition costs and blood pressure target achievement, as these are the outcomes of greatest budgetary relevance in UK primary care. No attempt was made to assess the cost of GP consultations, the management of adverse events, or of any other indirect expenditure. Although legitimate elements of healthcare expenditure, these elements are not directly accrued against specific budgets within the National Health Service and therefore fall outwith our remit. Having said that, there is no reason to suppose that the cost of these elements would vary depending on the ARB chosen, and therefore the relative performance of the two drugs evaluated would be unlikely to have been affected by their inclusion.
We chose to use blood pressure target achievement as a pragmatic surrogate outcome, rather than hard clinical endpoints such as stroke and coronary heart disease. In part this reflects the lack of relevant outcome data for the two agents evaluated. More importantly, however, although there is a clear relationship between absolute blood pressure lowering achieved and reduction in risk of eventsCitation4, hypertension is generally managed on a ‘treat-to-target’ basis. Several large clinical trials have evaluated the impact of using differing drug regimens in achieving targets in otherwise uncomplicated hypertensionCitation19–21. None of these studies have demonstrated any outcome benefit associated with using one treatment over another, target achievement being the only key discriminatorCitation22. We would therefore anticipate no clinical outcome advantage or disadvantage to be associated with the use of olmesartan versus candesartan. The use of a target achievement surrogate therefore seems to be justified.
Finally, the model only compared two ARBs, rather than all seven which are currently available. The exclusion of losartan from was on the grounds that this constitutes the clear first-line choice for mild hypertension, while this model concerns itself with a more difficult to treat cohort. Amongst the second-line ARBs, candesartan represents the clear market leader, thanks to its perceived low acquisition price. We therefore believed it constituted the legitimate comparator for olmesartan, which is the agent with the greatest BP lowering efficacy at standard doses (). There are no other ARBs that exceed the BP lowering efficacy of candesartanCitation23 and their prices are at least as great or higher. It is therefore unlikely that any additional comparisons would have added to the value of this analysis.
Conclusion
Clearly, not every patient with hypertension will require treatment with an ARB, and many of those that do will be satisfactorily controlled by generic losartan. However, for those in whom high baseline blood pressure or a challenging treatment target make losartan unsuitable, this study suggests that there is a sound budgetary case for choosing an olmesartan based regimen over one based on candesartan.
Transparency
Declaration of funding
This study was funded by Daiichi-Sankyo UK. Once the objectives of the study had been agreed, the sponsors played no further part in the modelling or write-up. A copy of the completed paper was seen by the sponsor prior to submission but no alterations were requested or made.
Declaration of financial/other relationship
The author has carried out paid health economic consultancy for Daiichi-Sankyo but has no stockholding or other financial stake in the company. As part of his commercial activities the author has also carried out paid consultancy in the past for large number of pharmaceutical companies, including those that market other antihypertensive treatments.
No assistance in the preparation of this article is to be declared.
References
- National Institute of Health and Clinical Evidence. Hypertension: Guidelines for management of hypertension in adults in primary care. London 2006. http://www.nice.org.uk/CG034
- Mansia G, De Backer G, Dominiczak A, et al. 2007 ESH-ESC Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press 2007;16:135-232
- Department of Health. nGMS Quality and Outcomes Framework 2009-10. London, 2009
- Collins R, Peto R, MacMahon S, et al. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet 1990;335:827-38
- NHS Business Services: Prescription Services. Drug Tariff March 2011
- NHS Business Services: Prescription Services. PCT data for BNF 2.5.5.2. October-December 2010. FoI request No: 513163
- Zannad F, Fay R. Blood pressure-lowering efficacy of olmesartan relative to other angiotensin II receptor antagonists: an overview of randomized controlled studies. Fundam Clin Pharmacol 2007;21:181-90
- Chrysant SG, Weber MA, Wang AC, et al. Evaluation of antihypertensive therapy with the combination of olmesartan medoxomil and hydrochlorothiazide. Am J Hypertens 2004;17:252-9
- Karlson BW, Zetterstrand S, Olofsson B, et al. A dose-response analysis of candesartan-hydrochlorothiazide combination therapy in patients with hypertension. Blood Press 2009;18:149-56
- Chrysant SG, Melino M, Karki S, et al. The combination of olmesartan medoxomil and amlodipine besylate in controlling high blood pressure: COACH, a randomized, double-blind, placebo-controlled, 8-week factorial efficacy and safety study. Clin Ther 2008;30:587-604
- MacGregor GA, Viskoper JR, Antonios TF, et al. Efficacy of candesartan cilexetil alone or in combination with amlodipine and hydrochlorothiazide in moderate-to-severe hypertension. UK and Israel Candesartan Investigators. Hypertension 2000;36:454-60
- Oparil S, Melino M, Lee J, et al. Triple therapy with olmesartan medoxomil, amlodipine besylate, and hydrochlorothiazide in adult patients with hypertension: The TRINITY multicenter, randomized, double-blind, 12-week, parallel-group study. Clin Ther 2010;32:1252-69
- British Medical Association and Royal Pharmaceutical Society. British National Formulary March 2011 (BNF 61) London, 2011
- Anonymous. Hydrochlorothiazide and bendroflumethiazide in low doses – a comparative trial. Acta Pharmacol Toxicol (Copenh) 1984;54(Suppl 1):47-51
- National Statistics. Prescription cost analysis: England 2009. http://www.ic.nhs.uk/statistics-and-data-collections/primary-care/prescriptions/prescription-cost-analysis-england–2009
- ISD Scotland. Prescription Cost Analysis: Scotland 2009. http://www.isdscotland.org/isd/2241.html
- Welsh Assembly. Prescription Cost Analysis Wales 2009. http://www.wales.nhs.uk/sites3/page.cfm?orgid=428&pid=13533
- HSC Business Services Organisation: Prescription Cost Analysis. http://www.centralservicesagency.com/display/statistics
- The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs. diuretic. JAMA 2002;288:2981-997
- Dahlöf B, Sever PS, Poulter NR, et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005;366:895-906
- Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet 2004;363:2022-31
- Staessen JA, Birkenhager WH. Evidence that new antihypertensives are superior to older drugs. Lancet 2005;366:869-71
- Heran BS, Wong MM, Heran IK, et al. Blood pressure lowering efficacy of angiotensin receptor blockers for primary hypertension. Cochrane Database Syst Rev 2008; CD003822