
Abstract
Objectives:
The high life-time prevalence of chronic back pain (25–30% according to surveys in small samples) suggests that it may be a major source of healthcare cost and that prevention of chronic back pain may be both ethically and economically recommendable. To obtain valid economic data on the cost of back pain in Germany, a retrospective claims data analysis was performed.
Methods:
Using data from 2006 of 5.2 million beneficiaries of a German statutory health insurance fund (DAK Unternehmen Leben) covering ∼7% of the German population, mean value analyses report on key healthcare utilization figures from a sickness funds’ perspective. In contrast to other studies, cost data are primary data and not extrapolated, but clinical characteristics include surrogate markers as no clinical case descriptions were available.
Results:
Based on previously investigated diagnosis patterns three types of back pain could be identified: (other) specific back pain (n = 211,216), pain due to spinal disk disease (n = 195,712), and non-specific back pain (n = 534,272). Of all back pain patients, 25.8% were identified as at risk to develop chronic pain, where only 2.6% were detected as patients with chronic back pain. Mean resource utilization and related healthcare costs were significantly higher for beneficiaries with indicators for chronic back pain than for beneficiaries with only risk factors for developing chronic back pain. This especially holds for outpatient analgesic prescriptions (p < 0.05), for in-hospital multimodal pain therapy (p < 0.05), for in-hospital care in general (p < 0.05), as well as for direct cost of care (p < 0.05).
Conclusion:
The results show the potential that could be made accessible by an early detection of back pain patients who bear a risk of pain becoming chronic, both in terms of quality-of-life as well as in financial terms.
Introduction
Back pain belongs to the prominent health problems which are frequently inadequately treated and go along with high direct and indirect costs for patients, sickness funds, and society. Headache and back pain account for the most frequent complaints why patients contact a physicianCitation1. Population-based surveys report an annual prevalence of ∼55–65% of back pain and a lifetime prevalence of chronic back pain of 25–30%Citation2,Citation3.
In 15% of all back pain patients clearly identifiable causes are detected, these patients suffer from specific back pain, whereas the other 85% experience non-specific back painCitation4. Most back pain patients are free of symptoms after 2 months, but for a part of them episodic recurrences occur and a smaller part is developing chronic back pain. Particularly chronic back pain often leads to prolonged sick leave and early retirement which substantially contributes to high healthcare utilization and costsCitation4.
The high estimates of prevalence and cost of care as well as the potential for improvements in back pain therapyCitation5 were the reasons for focusing on back pain within a perennial health services research project on pain on the basis of claims data. The study was initiated to gain new information on the structure and care of pain patients in a large population and under everyday clinical conditions and with primary data on cost. Two previous papers reported on a pre-study using the same database and establishing nine pain prototypes including three types of back painCitation6,Citation7.
We calculated key utilization numbers by two ways of differentiation. First we differentiated between three sub-groups of back pain: (other) specific back pain, pain with spinal disk disease, and non-specific back pain, and second we differentiated between three stages with respect to pain chronification: chronic back pain, risk for development of chronic back pain, and no indicator for chronic back pain. The aim of the study was to obtain realistic data on healthcare utilization depending on back pain type and status in the transition between acute and chronic pain.
Data and methods
Claims data from 2006 of 5.2 million beneficiaries of a nationwide statutory health insurance fund (DAK Unternehmen Leben) covering ∼7% of the German population were used for a retrospective analysis. The database contains demographic data (age, gender, employment status), medical diagnoses coded according to the International Classification of Diseases in the 10th Revision (ICD 10), as well as healthcare utilization data with respect to outpatient primary care, outpatient prescription of medication, remedies and therapeutic aids, hospital care, in-hospital and outpatient rehabilitation care, as well as days of sick leave up to 72 days. We identified those beneficiaries who belonged to the DAK throughout 2006 and 2007 and who presented at least one back pain-related diagnosis in 2006, documented within in-hospital or outpatient care. The core of the analyses are comparisons of mean values differentiated by indicators for chronic back pain.
Three types of back pain
We applied a newly developed diagnosis-based algorithm to identify and classify pain patients based on the same database of DAK claims data: This algorithm is based on diagnosis patterns found in beneficiaries who received at least two prescriptions of opioids in 2006 and it was used to identify pain patients among non-opioid beneficiariesCitation6,Citation7. As a result, 65 combinations of diagnosis groups were identified and aggregated to nine pain types: cancer, (other) specific back pain, pain due to intervertebral disk illnesses, pain due to arthrosis, pain after traumatic fractures, pain of multimorbid, high-maintenance patients, neuropathic pain, headache, and non-specific back pain. Three of them were related to back pain. Patients with multiple pain types were assigned to the pain type the involved experts defined as most vital for pain treatment (for further explanation see Freytag et al.Citation6). In the ICD 10 codes related to the defined sub-groups of back pain are listed.
Table 1. ICD 10 codes relevant for definition of back pain types.
Comorbidities
We distinguish between pain-related and non-pain-related comorbidities. Pain-related comorbidities are specified by diagnosis groups defining other pain types which the patient was not assigned to in the first place (such as pain due to arthrosis and arthritis, pain after traumatic fractures, pain of multimorbid, high-maintenance patients, neuropathic pain, headache). Non-pain-related comorbidities are specified by diagnosis groups not included in the set of pain type defining diagnosis groups (such as essential hypertension, prostatic hyperplasia, gastrointestinal diseases, etc.).
Back pain-related cost of care
Healthcare costs were calculated from the sickness funds’ perspective. Valuation of hospital care was based on hospital invoices. To price medical outpatient consultations (general practitioners and specialists) the number of consultations as well as diagnostic and therapeutic procedures were multiplied with provider-specific charges (‘Einheitlicher Bewertungsmaßstab’, EBM, medical fee schedule for physiciansCitation8). Charges (given in points) were translated into Euros using an average point score of 3.5001 Cent. The costs for drugs were based on pharmacy retail prices in 2006. Cost estimations for remedies and therapeutic appliances were based on the respective invoices. Costs for sickness leave benefits equal the amount of money the health insurance fund pays out to beneficiaries with sick leave of more than 42 days.
Pain-related costs were defined on the basis of expert opinion. They include costs for hospital and outpatient healthcare if they appeared in relation to a back pain-specific diagnosis as well as costs for analgesics and non-steroidal anti-inflammatory drugs. The costs for auxiliaries, physiotherapy, and sickness benefits were fully taken into account as the data could not be related to diagnoses.
Indicators for chronic back pain
Based on current recommendations of the German national guideline for low back painCitation9, the newly (2009) introduced ICD code for chronic pain in its German version (F45.41)Citation10, and expert opinion, we defined surrogate markers for three further categories within each back pain type: (a) chronic pain (more than 6 weeks sick leave or two prescriptions of opioids within a period of 180 days); (b) patients at risk for the transition from acute to chronic pain (no indicators of chronic pain, but at least one diagnosis related to psychiatric comorbidity or at least three cases of sick leave in 2006, ), and (c) acute pain (no indicators of (a) or (b)). Note that the ICD code F45.41 for chronic pain with somatic and psychological factors was introduced in 2009 and thus was not available in the database used here. It also puts emphasis on psychiatric comorbidities.
Table 2. ICD 10 codes for psychiatric comorbidities relevant for defining a risk for chronic back pain.
Results
Study population
Based on typical diagnosis patterns, three types of back pain could be identified: (other) specific back pain (n = 211,216), pain with spinal disk disease (n = 195,712), and non-specific back pain (n = 534,272). Altogether, these were 941,100 beneficiaries with at least one back pain-related diagnosis, 18% of the people insured at the statutory healthcare funds concerned. shows the prevalences of the defined sub-groups as well as their sociodemographic characteristics in the DAK sickness fund’s population having an above-average proportion of 65% women. Non-specific back pain (57%) outnumbered the other two back pain types. The population with (other) specific back pain was distinctly older than the other two back pain types.
Table 3. Study population.
Pain-related comorbidity
Beneficiaries with (other) specific back pain show up with pain due to arthrosis or arthritis at the same time in 75% of the cases. Neuropathic pain is a pain-related comorbidity in 28% of the beneficiaries with pain with spinal disk disease as well as in beneficiaries with (other) specific back pain. Due to our algorithm for assigning beneficiaries to pain types, those with non-specific back pain have no other pain-related comorbidities: if they did have other pain-related morbidities those beneficiaries would have been assigned to one of the pain types 1–8, and not to the pain type ‘non-specific back-pain’ (see ).
Table 4. Pain related comorbidities in three back pain types (hierarchical order).
A characteristic example of a patient with pain type ‘other specific back pain’ would be a 67-year old woman, retired, with osteoporosis without pathological fracture who also suffers from knee arthrosis, intevertebral disk disease, diabetes mellitus type 2, arteriosclerosis, and gastrointestinal disease. A characteristic example of a patient with pain type ‘intervertebral disk disease’ would be a 55-year old man, employed, with intervertebral disk shift with radiculopathy who also suffers from neuropathic pain, non-specific back pain, and essential hypertension. A characteristic example of a patient with pain type ‘non-specific back pain’ would be a 46-year old man, employed, with low-back pain as well as headache and affective disorder.
Non-pain-related comorbidities were distinctly higher in patients with (other) specific back pain, compared to the other two back pain types, especially with respect to essential hypertension, coronary heart diseases, and endocrine metabolic diseases.
Healthcare utilization of back pain patients
An overview of key utilization figures is shown in . Total figures are contrasted to pain-related figures. Patients with (other) specific back pain show the highest utilization and costs, particularly with regard to in-hospital treatment. The highest number of days of work disability due to the relevant back pain type can be observed in patients with pain caused by spinal disk disorders (6.1 days). Pain-related costs account for 21–29% of total costs.
Table 5. Healthcare utilization of back pain patients, 2006.
Healthcare utilization in transition from acute to chronic back pain
The majority of patients of all sub-groups showed no surrogate markers of chronic pain according to our classification; about a third (a fifth of patients with non-specific pain) was rated to be at risk of chronification (). In beneficiaries with (other) specific back pain, 6.8% of patients are shown to suffer from chronic back pain, 3.8% from pain in spinal disk disorders, and 0.5% from non-specific back pain. Of the surrogate markers for chronic pain, consecutive opiate prescription accounted for 87.5% of the cases, long-term sick leave for 12.1%, and 0.5% fulfilled both criteria. Of surrogate markers for risk of future chronic pain, psychiatric comorbidity accounted for 100% of the cases, and 0.6% also fulfilled the sick leave criterion (three and more sick leave cases).
Figures 1–8. Data from ‘Versorgungsatlas Schmerz’Citation16. 95% Confidence Intervals are indicated as vertical lines. Mean values across the three states from acute to chronic pain are indicated as horizontal lines. The shading of the bars in each back pain type has the following meaning: bright = without surrogate markers for chronic pain, middle = with surrogate markers for risk of future chronic pain, dark = with surrogate markers for chronic pain.
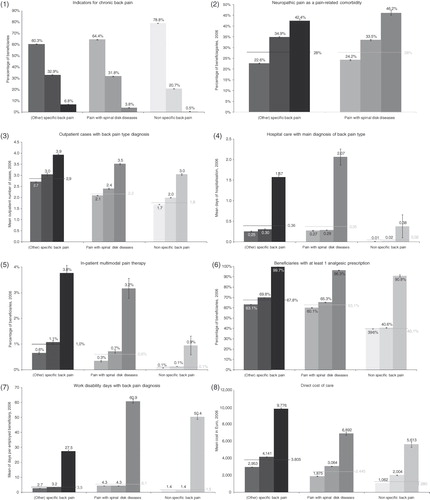
shows the fraction of specific back pain patients having a neuropatic pain comorbidity which increases by the state of pain chronicity. The figure is restricted to the two types of specific back pain, since, due to our algorithm for assigning beneficiaries to pain types in a hierarchical orderCitation6,Citation7, those beneficiaries assigned to ‘non-specific back pain’ per defitionem do not have any pain-related comorbidity (see also ).
In we counted outpatient cases for which the respective physician documented at least one back pain type-specific diagnosis. [Note that an outpatient case in Germany is a quarter in which one or more office visits were billed. An outpatient case embraces all office visits at the same physician per quarter of a year. This method was used since the data did not allow for counting office visits and the diagnoses documented are only available per outpatient case and not per office visit.] The mean number of outpatient cases is highest for (other) specific back pain. In chronic back pain patients the mean number is between 1.4–1.8-times higher than in patients with acute back pain.
The following physician groups were regarded as relevant for the treatment of back pain: (1) general practitioners and internists, (2) orthopedists, (3) surgeons and neurosurgeons, (4) anesthesiologists, (5) neurologists and psychiatrists, (6) psychotherapists, and (7) physicians specialized in physical and rehabilitative medicine. More than 80% of the patients with specific back pain have visited more than one physician group during 1 year. More than 65% of the patients with chronic specific back pain have visited three or more physician groups.
Diseases causing back pain are rarely treated in-hospital except in patients with surrogate markers for chronic pain (). Very few back pain patients receive in-hospital multimodal pain therapy (). Even in chronic back pain patients the percentage of those receiving a specific pain therapy is only 3.8%, in spite of the proven efficacy of multimodal pain therapy in preventing future sick leaveCitation11.
Two thirds of the patients with pain in spinal disk disorders or (other) specific back pain received at least one prescription for analgesic drugs, including non-steroidal anti-inflammatory drugs (NSAIDs) (), and for non-specific back pain this fraction was only two fifths. These numbers are likely under-estimates for actual pharmacological treatment since, in Germany, several NSAIDs are available over the counter. Strong-acting analgesic drugs are prescribed mostly to patients with specific back pain. As a consequence of our definition, the share of patients with opioid prescription is highest in patients with chronic back pain. (For further information on the duration of opioid treatment, on parameters influencing the continuity of opioid treatment as well as the effect of opioid treatment regimen on work disability, see Höer et al.Citation12.)
Back pain is a frequent reason for sick leave. This in particular holds for pain in spinal disk disorders. The mean number of days of work disability with a back pain diagnosis are strikingly high in the group of patients with chronic back pain (). This observation is the consequence of our definition of chronic back pain indicators in the cases in which sick leave served as an indicator for chronic pain (12.1%) and here it results in a circular argument. However, in the cases in which consecutive opioid prescriptions served as an indicator for chronic pain (87.5%), mean work disability with a back pain diagnosis also was remarkably higher (14 days) than in the group of patients without surrogate markers for chronic pain (4 days).
Finally, the present data show that back pain can be expensive: The stronger the indicators point to the risk or existence of chronic pain, the higher are the direct total costs of care (). This relation holds as well for the share of pain-related direct costs of care, which on average account for ∼25% of total direct costs. Yearly direct costs of care for patients with (other) specific chronic back pain were ∼9800 Euro on average in 2006, where 10,000 Euro is known as the threshold for high cost beneficiaries from a German sickness funds’ perspective. Pain-related costs accounted for 20–30% of total direct cost of care. These percentages also hold for all back pain types with indicators of acute back pain and the risk of development for chronic pain. Only in patients with chronic pain, the percentage of pain-related costs rises up to 47% of total cost in patients with spinal disk diseases (3,265 Euro out of 6,892 Euro), meaning that almost half of one years’ total cost may be caused by back pain. (For further information on the distribution of types of cost see Freytag et al.Citation13).
Discussion
We have analyzed the healthcare utilization of back pain patients in a real world setting by use of health insurance claims data (2006 and 2007) with special respect to the transition from acute to chronic pain.
Based on a previously defined algorithmCitation6,Citation7 three types of back pain were identified: (other) specific back pain (n = 211,216), pain due to spinal disk disease (n = 195,712), and non-specific back pain (n = 534,272).
Using surrogate markers of pain chronicity (psychiatric comorbidity, sick leave, consecutive opioid prescriptions), 2.6% were detected as patients with chronic back pain, but 25.8% of all back pain patients were identified as at risk of future chronic pain. Thus, there are ∼10-times as many patients at risk for chronic pain than actually suffering from chronic pain. This population (242,420, equalling 4.7% of all DAK beneficiaries) is an excellent target for focused preventive back health programs.
Mean resource utilization and related healthcare costs per case were significantly higher for beneficiaries with indicators for chronic back pain than for beneficiaries with only risk factors for future chronic back pain. This especially holds for outpatient analgesic prescriptions (p < 0.05), for in-hospital multimodal pain therapy (p < 0.05), for in-hospital care in general (p < 0.05), as well as for direct cost of care (p < 0.05).
The limitations of this study primarily result from restrictions that go along with claims data analysis in general: This is in particular the lack of direct clinical information such as examination or history’s results. For the present study this was crucial in two ways: First, defining sub-groups of back pain had to rely on an indirect claims-based diagnosis algorithmCitation6,Citation7. Second, for the attempt to identify patients with chronic back pain presence of psychiatric diagnoses was taken for a risk factor of pain becoming chronic, the repeated prescription of strong-acting opioids or ongoing sick leave for existing chronicity instead of direct information on the duration of pain, which is important information for pain classification according to the German national guideline on low back pain. However, duration of pain is not the primary marker of pain chronicity. The theoretical construct of chronic pain as a disease is a loss of the warning function, which cannot be tested clinicallyCitation14. In some patients, e.g. with hip osteoarthritis, pain may—like acute pain—still be reversible by surgery, even after decades, whereas in other patients some characteristics of chronic pain may be present from the beginningCitation15. Psychosocial parameters are the best available predictors for pain to become chronic, and their treatment requires additional therapeutic efforts. For these reasons, they have been introduced into a new chronic pain diagnosis in the German version of ICD 10 in 2009Citation10.
Non-employed patients are disadvantaged in the present analysis with respect to the definition of chronicity, which in this group exclusively relies on the prescription of opioids. This most likely results in an under-estimation of the percentage of patients with chronic back pain. Nevertheless, these aspects are of no further significance for the results of our study since it was not our aim to estimate the prevalence of chronic back pain, but to differentiate healthcare utilization by indicators of pain chronification. The same logic holds for the distribution of beneficiaries across the three back pain types.
Despite the limitations discussed, the present study contributes to the understanding of back pain patients’ healthcare. The strength of the results can particularly be seen in the statistical advantages that are related with the large size of the cohort under analysis. Claims data arise from everyday clinical conditions and, thus, are better able to describe everyday clinical care than possible under the limited conditions of clinical trials. Moreover, all cost data in this paper are real expenses in the year 2006 for 7% of the German population, without using any extrapolations.
Conclusion
This health insurance claims data analysis confirmed that the highest healthcare utilization and cost per patient occurred in patients with specific back pain and in patients with surrogate markers of chronic pain. The opposite was true for total cost to the health insurance funds, since uncomplicated non-specific back pain is by far the most frequent type. Patients at risk to develop chronic pain outnumbered those already experiencing chronic pain by a factor of 10 and made up for 26% of the patients in this study, equalling 4.7% of the DAK beneficiaries. These results show the potential that could be made accessible by an early detection of back pain patients who bear a risk of pain becoming chronic, both in terms of quality-of-life as well as in financial terms.
Transparency
Declaration of funding:
This study was funded by Grunenthal GmbH, Germany, manufacturer of opioids, and executed by the IGES Institute, Germany. The project was overseen by an advisory board with delegates from the German Society for the Study of Pain e.V. (DGSS: RDT), German Society for Pain Therapy e.V. (DGS: GMS), Interdisciplinary Society for Orthopedic Pain Therapy (IGOST: HRC), and Professional Association of Physicians and Psychologic Psychotherapists in Pain and Palliative Medicine in Germany e.V. (BVSD: RT). This advisory board received travel reimbursement for face-to-face meetings, but no honoraria.
Declaration of financial/other interests:
AF, GS, and AH have disclosed that they are employees of the IGES Institute, which received the financial support to execute the data analyses and publication of results described in the manuscript. GMS, AB, HRC, GG, RT, and RDT have disclosed that they are members of the advisory board to the project and do not receive financial reimbursement except for travel expenses. GG receives research grants from different health insurance funds and physician’s associations. AB, GMS, and RT occasionally give speeches on behalf of Grunenthal. RDT received research-funds, consulting fees, and remuneration from: Allergan, Astellas, Boehringer Ingelheim, Galderma, Glaxo Smith Kline, Grünenthal, Dr. Kade, Lilly, Merck, Sharpe & Dohme, Merz, Nycomed, Pfizer, Sanofi, Schwarz Pharma. CMRO peer reviewers may have received honoraria for their review work. The peer reviewers on this manuscript have disclosed that they have no relevant financial relationships
References
- Breivik H, Collett B, Ventafridda V, et al. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. European Journal of Pain 2006; 10:287–333
- Kohler M, Ziese T. Telefonischer Gesundheitssurvey des Robert Koch-Instituts über chronische Krankheiten und ihre Bedingungen [Telefonic Health Survey of the Robert Koch Institute about chronic diseases and their conditions], 2004, Berlin, Robert Koch-Institut, Gesundheitsberichterstattung des Bundes
- Schmidt CO, Raspe H, Pfingsten M, et al. Back pain in the German adult population: prevalence, severity, and sociodemopraphic correlates in a multiregional survey. Spine 2007;32:2005-11
- Bundesministerium für Bildung und Forschung (BMBF). Chronischer Schmerz. Ergebnisse der Forschung verbessern die Versorgung der Patienten [Chronic pain. Reasearch results improve patients‘ care]. Berlin: BMBF publik 2001
- Schmidt CO, Kohlmann T. Versorgungssituation bei Rückenschmerzen. [Health care situation in back pain]. M Koch und HR Vogel: Weißbuch Schmerz 2008 [White Book on pain 2008]: 21-25; Stuttgart: Thieme
- Freytag A, Schiffhorst G, Thoma R, et al. Identifikation und Gruppierung von Schmerzpatienten anhand von Routinedaten [Identification and grouping of pain patients according to claims data]. Der Schmerz 2010;1:12-2
- Schiffhorst G, Freytag A, Höer A, et al. Schmerztypische Diagnosemuster in Routinedaten – Identifikation mittels Classification and Regression Trees (CART) [Pain-specific diagnosis patterns – identification by means of Classification and Regression Trees]. Das Gesundheitswesen 2010;72:347-55
- Kassenärztliche Bundesvereinigung. Einheitlicher Bewertungsmaßstab 2005 [Uniform physicians’ fee scale 2005]. Köln: Deutscher Ärzte-Verlag GmbH, 2005
- German Medical Association (BÄK), National Association of Statutory Health Insurance Physicians (KBV), Association of the Scientific Medical Societies in Germany (AWMF). Nationale Versorgungsleitlinie Kreuzschmerz- Langfassung [National guideline for low back pain – long version]; 1.0. 2010. 30-11-2010. http://www.kreuzschmerz.versorgungs leitlinien.de/
- Nilges P, Rief W. F45.41 Chronische Schmerzstörung mit somatischen und psychischen Faktoren – eine Kodierhilfe [F45.41 Chronic pain disturbance with somatic and psychological factors – a coding aid]. Der Schmerz 2010;24:209-12
- Busch H, Bodin L, Bergström G, et al. Patterns of sickness absence a decade after pain-related multidisciplinary rehabilitation. Pain 2011;152; 8:1727-33
- Höer A, Freytag A, Schiffhorst G, et al. Opiodversorgung von Versicherten mit Rückenschmerzen. Ergebnisse einer Versorgungsforschungsanalyse auf der Basis von Routinedaten einer gesetzlichen Krankenkasse [Opioid therapy in patients with back pain. Claims data analysis for patient groups characterisation, for influences on opioid therapy and work disability]. Der Schmerz 2011;25;2:174-83
- Freytag A, Thiede M, Schiffhorst G, et al. Versorgungskosten von Rückenschmerzen und die Bedeutung der Schmerzchronifizierung – Ergebnisse einer GKV-Routinedatenanalyse [Costs of care of back pain and the significance of pain chronification – results of a claims data analysis], Gesundheitsökonomie & Qualitätsmanagment 2011; DOI: 10.1055/s-0031-1281578
- Baron R, Koppert W, Strumpf M, et al. Praktische Schmerztherapie: Interdisziplinäre Diagnostik – multimodale Therapie [Practical pain therapy: Interdisciplinary diagnostics – multimodal therapy]. Springer: Berlin Heidelberg; 2nd Edition, 2011
- Gerbershagen HU. Das Mainzer Stadienkonzept des Schmerzes. Eine Standortbestimmung [Mainz dimensions for pain staging]. In: Klinger D, Morawetz R, Thoden U, et al. (Eds.). Antidepressiva und Analgetika [antidepressants and analgesics]. Arachne Verlag: Vienna, 1996:71-95
- Grünenthal GmbH (Ed.). Versorgungsatlas Schmerz [factbook on pain], Velbrück: Weilerswist, ISBN978-3-942393-95-9