
Abstract
Objective:
To estimate the budget impact of everolimus as the first and second treatment option after letrozole or anastrozole (L/A) failure for post-menopausal women with hormone receptor positive (HR+), human epidermal growth factor receptor-2 negative (HER2-) advanced breast cancer (ABC).
Methods:
Pharmacy and medical budget impacts (2011 USD) were estimated over the first year of everolimus use in HR+, HER2- ABC from a US payer perspective. Epidemiology data were used to estimate target population size. Pre-everolimus entry treatment options included exemestane, fulvestrant, and tamoxifen. Pre- and post-everolimus entry market shares were estimated based on market research and assumptions. Drug costs were based on wholesale acquisition cost. Patients were assumed to be on treatment until progression or death. Annual medical costs were calculated as the average of pre- and post-progression medical costs weighted by the time in each period, adjusted for survival. One-way and two-way sensitivity analyses were conducted to assess the model robustness.
Results:
In a hypothetical 1,000,000 member plan, 72 and 159 patients were expected to be candidates for everolimus treatment as first and second treatment option, respectively, after L/A failure. The total budget impact for the first year post-everolimus entry was $0.044 per member per month [PMPM] (pharmacy budget: $0.058 PMPM; medical budget: −$0.014 PMPM), assuming 10% of the target population would receive everolimus. The total budget impacts for the first and second treatment options after L/A failure were $0.014 PMPM (pharmacy budget: $0.018; medical budget: −$0.004) and $0.030 PMPM (pharmacy budget: $0.040; medical budget: −$0.010), respectively. Results remained robust in sensitivity analyses.
Limitations:
Assumptions about some model input parameters were necessary and may impact results.
Conclusions:
Increased pharmacy costs for HR+, HER2- ABC following everolimus entry are expected to be partially offset by reduced medical service costs. Pharmacy and total budget increases were modest.
Introduction
According to the National Cancer Institute, ∼230,480 new cases and 39,520 deaths from breast cancer were projected in the US for 2011Citation1. Approximately 58% of patients with breast cancer are classified as having hormone receptor positive (HR+), human epidermal growth factor receptor-2 negative (HER2-) diseaseCitation2,Citation3. Current treatment guidelines for HR+, HER2- advanced breast cancer (ABC) recommend treatments based on individual patient characteristics, and hormone therapy is the commonly recommended initial treatment for postmenopausal womenCitation4. Hormone therapy with aromatase inhibitors (e.g., letrozole and anastrozole) is the mainstay of initial treatment; however, not all patients respond to the initial hormonal treatment, and most patients who respond initially will later develop resistance and experience disease progressionCitation5,Citation6. Patients experiencing progression after initial treatment with an aromatase inhibitor may be treated with another aromatase inhibitor (e.g., exemestane) or with an estrogen-receptor antagonist (e.g., fulvestrant or tamoxifen)Citation7.
Everolimus (Afinitor®), in combination with exemestane, has recently been approved for the treatment of advanced HR+, HER2- breast cancer in post-menopausal women after they fail treatment with letrozole or anastrozole. Everolimus targets the mammalian target of rapamycin (mTOR) pathway in cancer cellsCitation8. The approval is based on the phase III randomized clinical trial, BOLERO-2 (Breast Cancer Trials of Oral Everolimus; NCT00863655), which has compared the safety and efficacy of everolimus in combination with exemestane to exemestane alone for the treatment of HR+, HER2- ABC in post-menopausal women following failure with letrozole or anastrozoleCitation7. Compared to exemestane alone, combination therapy of everolimus and exemestane was associated with significantly longer progression-free survival (PFS) in the study population. The superior efficacy, measured by PFS, of everolimus plus exemestane was consistent across all sub-groups evaluated in the clinical trial, e.g., patients who had previously taken multiple prior therapies, patients 65 or older, and patients with metastatic diseaseCitation7.
These findings indicate the potential for everolimus to enhance the clinical benefit of hormonal therapy in refractory HR+, HER2- ABC patients. However, in light of healthcare resource constraints, payers require information about the expected budgetary impact of new treatments, such as everolimus, to guide decisions about coverage and formulary placement. The objective of this study was to estimate the budget impact to a US health plan associated with introducing everolimus as a first and second treatment option after letrozole or anastrozole failure in post-menopausal women with HR+, HER2- ABC.
Methods
Model overview
This model assessed the pharmacy and medical budget impacts during the first year of everolimus entry for the treatment of HR+, HER2- ABC from a third-party payer perspective in the US (). The target population, i.e., post-menopausal women with HR+, HER2- ABC who were candidates for everolimus treatment, included two groups: (1) patients who would receive further cancer treatments immediately after failure of letrozole or anastrozole (i.e., no other treatment between letrozole or anastrozole and further treatments); and (2) patients who would receive further cancer treatments after failure of letrozole or anastrozole and a subsequent treatment. The model was constructed for a hypothetical health plan population of 1 million covered lives. For the scenario prior to everolimus entry, treatment options in the model included exemestane, fulvestrant, and tamoxifen; for the scenario following everolimus entry, combination therapy with everolimus plus exemestane was added to this list. In addition, we assumed that the size of the target population would remain constant before and after the entry of everolimus. The economic impact of everolimus entry was modeled considering the impact on pharmacy costs, as well as changes in medical service costs due to expected improvements in PFS. Individuals were assumed to remain on treatment until progression or death and incur different medical costs before vs after disease progression.
Figure 1. Budget impact model structure. Model structure is based on current modeling standards for the budget impact of pharmaceutical products.
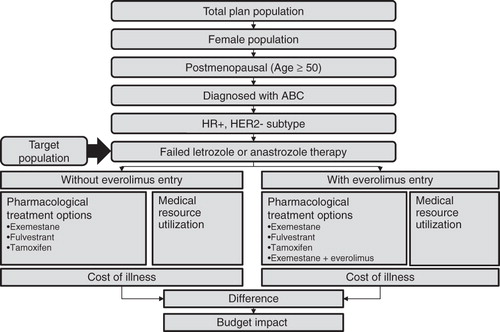
Model output included total annual incremental budget impact in dollars, and budget impact on a per-member per-month (PMPM) basis for the treatment of post-menopausal HR+, HER2- ABC patients during the first year of everolimus entry. All analyses were conducted in Microsoft Excel.
Model inputs and calculation
Target population
The size of the target population in a hypothetical health plan with 1 million enrollees was estimated using inputs derived from public databases, published literature, and assumptions (). Of the 1 million enrollees, 50.8% were assumed to be female, based on the US census estimatesCitation9. The percentage of US women 50 years and older (34%) was obtained from the US census dataCitation9, and was used as a proxy for the proportion of female enrollees who would be post-menopausalCitation10. Based on the published SEER 2008 data, the prevalence of breast cancer within the post-menopausal female population was 3.5%Citation1. The prevalence of advanced disease among patients with breast cancer was 6.9%, based on a recently published epidemiologic data reportCitation11. The proportion of ABC patients with sub-type HR+, HER2- was approximated by the proportion of all breast cancers with this sub-type (58.3%)Citation2. All patients with HR+, HER2- ABC were assumed to have been treated with either letrozole or anastrozole following the diagnosis of advanced diseaseCitation4. Finally, 70% of these patients were expected to have failed treatment with letrozole or anastrozole based on reported response rates of 20–40% for hormonal therapy in HR+ ABCCitation6.
Table 1. Target population inputs.
Candidates for everolimus plus exemestane treatment were estimated among patients who failed letrozole or anastrozole. Specifically, 42.3% of patients would be receiving their first treatment immediately after letrozole or anastrozole in a given year, and these patients were considered as candidates for using everolimus as the first treatment option after letrozole or anastrozole failure. The 42.3% was obtained as the percentage of the BOLERO-2 trial population reporting no prior use of anti-estrogen therapy (tamoxifen or fulvestrant) before the trialCitation7. Moreover, 93.6% of patients who failed letrozole or anastrozole would receive a second treatment after failing letrozole or anastrozole and the first treatment in a given year, and these patients were considered as candidates for using everolimus as the second treatment option after letrozole or anastrozole failure; this percentage is derived as the combined percentage of patients in BOLERO-2 who had already failed other anti-estrogen therapy before the trial (57.7%), and those who failed the first treatment received immediately after letrozole or anastrozole (assumed to be 85% of 42.3%).
Market share
Separate market share distributions across the treatment options were used for patients on their first vs second treatment after letrozole or anastrozole failure. Market shares before everolimus entry were obtained from unpublished market research data [data on file, Novartis Pharmaceuticals; East Hanover, NJ ()]. The market share of everolimus plus exemestane was assumed to increase linearly and reach 10% by the end of the first year following everolimus entry. Market shares for other treatments after everolimus entry were estimated such that everolimus would replace each treatment proportional to their market shares prior to everolimus entry.
Table 2. Market share inputs.
Pharmacy costs
Pharmacy costs for treating HR+, HER2- ABC were estimated for 1 year before and 1 year after everolimus entry, from a US payer perspective. The pharmacy cost per patient per year (PPPY) for each treatment option was calculated based on the average wholesale acquisition cost (WAC), treatment duration, dispensing fees, and co-payment () using the following formula:
Table 3. Pharmacy cost inputs.
The total pharmacy cost for each treatment option was calculated by multiplying the pharmacy cost PPPY by the number of patients expected to receive each treatment based on the market share.
WAC unit prices were obtained from ReadyPrice®Citation12. If multiple unit prices were available, the average of these prices was used. Because patients were assumed to remain on treatment until progression or death, median PFS for each therapy was used as a proxy for treatment duration. Median PFS of everolimus plus exemestane combination therapy and exemestane monotherapy in the target population were 7.8 months and 3.2 months, respectively, based on the everolimus product labelCitation8. In a separate phase III trial with a similar trial population, fulvestrant and exemestane showed no difference in median PFSCitation13; thus, PFS with fulvestrant was also assumed to be 3.2 months. Based on a sub-study of a cross-over trial, median PFS with tamoxifen in the target population was 6.7 monthsCitation14. Treatment duration, estimated by the median PFS, was assumed to be the same regardless of whether the treatment was used as the first or second treatment option after failure with letrozole or anastrozole.
Average number of fills for exemestane, tamoxifen, and everolimus was calculated as the number of days on medication divided by 30, the days-supply for a typical prescription fill. The number of fills for fulvestrant was estimated as the number of doses that a patient would take during the progression-free period following a standard dosing schedule of three administrations in the first month and once per month thereafter. Compliance was assumed to be 100% for all drugs while patients were on medication. This assumption was varied in the one-way sensitivity analyses. The expected co-payment per prescription fill was assumed to be $10 for exemestane and tamoxifen and $40 for everolimus and fulvestrantCitation15. The dispensing fees were assumed to be $1.89 for all treatments, based on the International Society of Pharmacoeconomics and Outcomes Research (ISPOR) guidelinesCitation16. The dispensing fee was inflated to 2011 dollars using the medical component of the consumer price indexCitation17.
Total annual pharmacy costs included the sum of estimated pharmacy costs for all available treatments in a particular year. Costs per member per month (PMPM) were estimated by dividing total monthly pharmacy costs by the total number of plan enrollees. The pharmacy budget impact of everolimus entry was estimated as the difference in pharmacy costs between the pre- vs post-everolimus entry scenarios.
Medical costs inputs
Medical service costs associated with non-progression and progression disease states were obtained from a study that estimated medical charges for inpatient, emergency room, and outpatient services incurred 6 months before and after a distant recurrence of metastasis among breast cancer patients ()Citation18. These charges were converted to costs using cost-to-charge ratio and inflated to 2011 US dollars using the medical component of the consumer price indexCitation17,Citation19. As clinical trials might measure adverse events differently, costs of adverse events were not included in the base case analysis but was considered in the sensitivity analysis.
Table 4. Medical cost inputs.
Medical costs were prorated according to the proportion of the year that patients were expected to live using overall survival data. In the BOLERO-2 trial, mortality rates associated with everolimus plus exemestane combination therapy and exemestane monotherapy were 17% and 23%, respectively, at a median follow up of 12.5 monthsCitation20. Overall survival rates as well as median follow-up times for tamoxifen and fulvestrant were assumed to be the same as that of exemestane monotherapy. For each treatment option, average survival time of a patient during the year was computed using mortality rate and median follow-up time by assuming a constant death rate. Average survival time for first and second treatment options after failure with letrozole or anastrozole was assumed to be the same.
Medical costs PPPY for each treatment was calculated as:
Similar to pharmacy costs, total annual medical costs were estimated as the sum of medical costs for all available treatments in a particular year. Medical budget impact, both in the plan total and PMPM, was estimated as the difference in medical costs during the 1 year before and after everolimus entry.
Sensitivity analyses
One-way and two-way sensitivity analyses were performed to assess the impact of variations in key model inputs on the results. The parameters considered in the sensitivity analyses included market share, drug price of everolimus, duration of PFS, medical costs, and compliance rate. In the base case, everolimus plus exemestane market share within the target population was 10% by the end of the first year for both the first and second treatment option settings; in the sensitivities, the market share of everolimus plus exemestane in both settings was varied from 5–15%. In addition, a scenario was considered assuming 20% market share for the second treatment option after letrozole or anastrozole failure. The size of the target population, everolimus costs, PFS duration, progression, and non-progression cost inputs were all varied ±25% of their base case values in the sensitivity analyses. A scenario of no medical cost offset (i.e., assuming that progression and non-progression costs were the same) was also included. Compliance rates of all drugs were varied from 100% in the base case to 70%.
Sensitivity analysis was also performed to evaluate the impact of including the cost of adverse events. Only grade 3/4 levels adverse events with at least 5% incidence in any arm of the BOLERO-2 trial (stomatitis and anemia) were consideredCitation7. Unit costs of adverse events (i.e., cost per patient per event) were obtained from the literature. Expected cost of AEs per patient was calculated based on the AE rates and unit costs of adverse eventsCitation21,Citation22, and was estimated at $847 for patients receiving everolimus plus exemestane and $141 for those receiving exemestane alone. Because the clinical trials of fulvestrant and tamoxifen did not report grade 3/4 adverse events, the adverse event costs for exemestane were applied to fulvestrant and tamoxifen.
In the two-way sensitivity analyses, the target population size was varied simultaneously with everolimus cost and medical cost, respectively. Specifically, the target population size was varied from 50–150% of the base case, and at the same time the everolimus cost or medical costs for both progression and non-progression varied ±25% of the base case values.
Results
In a hypothetical health plan with 1 million members, the target population in a given year was estimated to include 72 patients receiving their first treatment immediately after letrozole or anastrozole failure, and 159 patients receiving a second treatment after failing letrozole or anastrozole and the first treatment. Individuals in these groups represent post-menopausal women who would be eligible to receive everolimus plus exemestane combination therapy for HR+, HER2- ABC following letrozole or anastrozole failure.
summarize the expected budgetary impact of everolimus entry in terms of total annual costs and PMPM costs, respectively. Total annual costs (pharmacy and medical) were estimated at $12,050,083 before everolimus entry compared to $12,572,419 post-entry, yielding an estimated total budget impact of $522,336 to a US payer during the first year after everolimus entry. This amount corresponded to a PMPM cost increase of $0.044 in the first year. The total budget impact included an estimated pharmacy budget increase of $692,540 ($0.058 PMPM) and a medical service budget decrease of $170,204 ($0.014 PMPM) within a year following the everolimus entry.
Figure 2. Budget impact for the first year of everolimus entry, (a) plan total, and (b) PMPM.
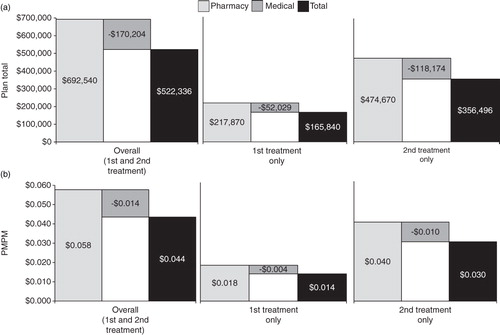
In the target population of patients receiving their first treatment after letrozole or anastrozole failure, the total annual costs (pharmacy and medical) for treating HR+, HER2- ABC were estimated to be $3,687,519 before vs $3,853,359 after everolimus entry, leading to a total budget impact of $165,840 ($0.014 PMPM). The total budget impact included an expected pharmacy budget increase of $217,870 ($0.018 PMPM) and an expected medical budget decrease of $52,029 ($0.004 PMPM).
In the target population of patients receiving their second treatment after letrozole or anastrozole failure, the total annual costs for treating HR+, HER2- ABC were estimated to be $8,362,564 before vs $8,719,059 after everolimus entry. This led to an estimated total budget of $356,496 ($0.030 PMPM) during the first year post-everolimus entry, including an expected pharmacy budget increase of $474,670 ($0.040 PMPM) and a medical budget decrease of $118,174 ($0.010 PMPM).
Sensitivity analysis results
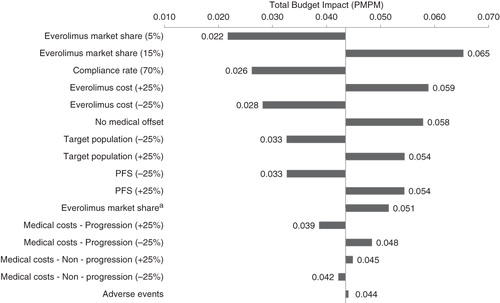
One-way sensitivity analyses showed that model results were robust to changes in key input values; total 1 year budget impact after the introduction of everolimus ranged from $0.022–$0.065 PMPM in the one-way sensitivity analyses (). The model results were most sensitive to market share of everolimus plus exemestane, therapy compliance rates, and drug cost of everolimus.
Figure 3. One-way sensitivity analyses. aEverolimus plus exemestane market share: 20% market share as the second treatment option after letrozole or anastrozole failure.
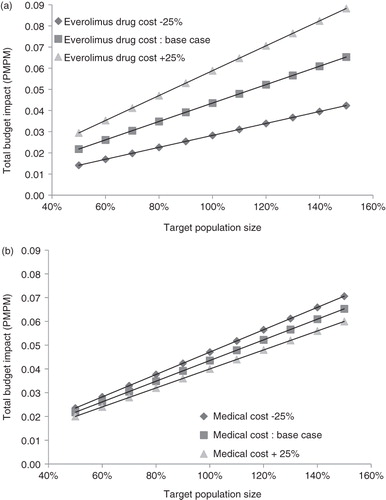
Two-way sensitivity analyses demonstrated the impact of variations in both target population size and drug () or medical cost (). Total budget impact of everolimus entry was the highest ($0.088 PMPM) when assumptions simultaneously considered 50% larger target population size and 25% higher everolimus cost, compared to the base case. The smallest budget impact ($0.014 PMPM) corresponded to 50% smaller target population and 25% lower everolimus cost, compared to the base case. Varying medical costs simultaneously with target population size had a smaller impact on model results (ranging from $0.020–$0.071 PMPM) than varying everolimus costs simultaneously with target population size (ranging from $0.014–$0.088 PMPM).
Figure 4. Two-way sensitivity analyses. (a) Target population size and everolimus cost. (b) Target population size and medical cost.
Discussion
Commonly recommended treatment options for post-menopausal women with HR+, HER2- ABC include hormone therapy with anti-estrogens (tamoxifen, fulvestrant) and the third-generation aromatase inhibitors (letrozole, anastrozole, and exemestane). However, there are substantial unmet needs in this population, especially after primary non-response or disease relapse with letrozole or anastrozole treatmentCitation6. The recent BOLERO-2 trial showed that the combination of everolimus with exemestane significantly prolonged PFS compared to exemestane alone (7.8 months vs 3.2 months) among post-menopausal women with HR+, HER2- ABC after letrozole or anastrozole failureCitation8, making everolimus plus exemestane a promising treatment option for this patient population. Yet, because everolimus is associated with higher drug acquisition costs compared to alternatives, such as exemestane monotherapy or tamoxifen, for which generic drugs are available, the economic impact of including everolimus as a new treatment option would be of interest to payers. The present study sought to evaluate the budget impact of adding everolimus to a health plan formulary for this indication. This study is the first to report the estimated budget impact of introducing everolimus as a treatment option for HR+, HER2- ABC among post-menopausal patients who have previously failed letrozole or anastrozole therapy. Budget impact analysis has become increasingly important to the comprehensive economic assessment of new pharmaceutical products. The estimated impact of a newly-available drug on annual pharmacy and medical expenditures is crucial not only for financial planning, but also for anticipating its effect on service provision within the healthcare systemCitation23.
The model accounted for the potential entry of everolimus as either a first or second treatment option after letrozole or anastrozole failure. Over 68% of the estimated 1-year budget impact stemmed from the uptake of everolimus plus exemestane as a second treatment option after failure of letrozole or anastrozole. This was because the target population receiving a second treatment option was expected to be much bigger than that receiving a first treatment option after letrozole and anastrozole failure. Overall, adding everolimus for HR+, HER2- ABC is projected to have a limited impact on total budget for a US health plan ($0.044 PMPM). In the year following everolimus entry, the estimated increase of $0.058 PMPM in pharmacy costs is likely to be partially offset by reductions in medical service expenditures (−$0.014 PMPM). Medical cost offsets mainly result from the improved efficacy of everolimus plus exemestane combination treatment in delaying disease progression relative to other treatments, and the incremental costs associated with disease progression. Results remained robust in sensitivity analyses and were most sensitive to market share, compliance, and everolimus drug costs. In all one-way sensitivity analyses, total budget impact remained low, with a maximum budget impact of $0.065 PMPM when everolimus market share was 15%. In the two-way sensitivity analyses, total budget impact varied from $0.014–$0.088 PMPM, the maximum corresponding to an increase in everolimus cost by 25% and an increase in target population size by 50%. The low estimated impact of everolimus entry on total plan budget and large potential gains in PFS from everolimus plus exemestane combination therapy support the formulary placement of everolimus for post-menopausal women with HR+, HER2- ABC who have failed letrozole or anastrozole.
Limitations
As with most economic models, results from this budget impact analysis are contingent on the assumptions that were applied. While every effort was made to obtain key model inputs from the best available evidence, assumptions about some parameters were necessary for the budget impact estimation and may impact the model output. First, due to limited real-world data on treatment patterns and outcomes in HR+, HER2- ABC, published data from clinical trials were used to estimate the prevalence of letrozole- or anastrozole-refractory disease, as well as the percentages of these individuals who would require a first and/or second treatment option after letrozole or anastrozole failure within a given year. The model estimation should be validated or refined as additional data from real-world clinical practice become available. Second, in the absence of detailed information about adherence to different treatment options, the model assumed 100% compliance for all medications while patients were on treatment. Differing levels of compliance to different treatment options for HR+, HER2- ABC may be an important determinant of clinical outcomes in real-world practice; nevertheless, the assumption of perfect compliance is conservative with respect to everolimus due to the higher acquisition cost of this medication relative to alternative treatments. For example, assuming a 70% compliance rate lowered the total budget impact by 40%. Third, median PFS for each drug, which is used as a proxy for mean duration on medication, was obtained from separate clinical trials. Although these studies had similar eligibility criteria, heterogeneity across the trial populations may still exist, which may affect the PFS estimates associated with different treatments. Lastly, data were not available to estimate separate median PFS and overall survival between patients receiving their first vs second treatment option following letrozole or anastrozole failure. It was also necessary to assume that overall survival with tamoxifen and fulvestrant would be the same as reported for exemestane monotherapy in BOLERO-2. The model could be further updated as additional clinical data are available.
Conclusion
For post-menopausal patients with HR+, HER2- ABC who have previously failed letrozole or anastrozole therapy, introduction of everolimus as a new treatment option in combination with exemestane is projected to increase the pharmacy budget while reducing medical service expenditures, yielding a modest net increase in total budget from a US payer perspective. Results from this analysis may be useful for formulary placement decisions of breast cancer therapies.
Transparency
Declaration of funding
Funding for this study was provided by Novartis Pharmaceuticals Corporation (East Hanover, NJ), the manufacturer of everolimus.
Declaration of financial/other relationships
Jipan Xie, Melissa Diener, Gourab De, Hongbo Yang, and Eric Q. Wu are employed by Analysis Group, Inc., which received consulting fees for this study. Madhav Namjoshi is employed by and holds stock options in Novartis.
Acknowledgments
Medical writing services were provided by Arielle G. Bensimon, who is employed by Analysis Group, Inc.
References
- National Cancer Institute. SEER Cancer Statistics Review 1975-2008. SEER, 2011. http://seer.cancer.gov/csr/1975_2008/. Accessed October 24, 2011
- Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 2006;295:2492–502
- Hannemann J, Kristel P, van Tinteren H, et al. Molecular subtypes of breast cancer and amplification of topoisomerase II alpha: predictive role in dose intensive adjuvant chemotherapy. Br J Cancer 2006;95:1334–41
- National Comprehensive Cancer Network I. NCCN clinical practice guidelines in oncology: breast cancer. 2011;NCCN.org. Accessed October 5, 2011
- Gonzalez-Angulo A, Morales-Vasquez F, Hortobagyi G. Overview of resistance to systematic therapy in patients with breast cancer. Madame Curie Bioscience Database [Internet]. Austin, TX: Landes Bioscience, 2000
- Johnston S. New strategies in estrogen receptor-positive breast cancer. Clin Cancer Res 2010;16:1979–87
- Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med 2012;366:520–9
- U.S. Food and Drug Administration. Approved label for everolimus. FDA, Silver Spring, MD, 2012. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.DrugDetails. Accessed on September 13, 2012
- US Census Bureau. Table 1: intercensal estimates of the resident population by sex and age for the United States: April 1, 2000 to July 1, 2010 (US-EST00INT-01). US Census Bureau, Washington, DC, 2010
- Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet 1997;350:1047–59
- Ho J, Zhang L, Todorova L, et al. Budget impact analysis of ixabepilone used according to FDA labeling in treatment-resistant metastatic breast cancer. J Manag Care Pharm 2009;15:467–75
- Drug Topics RedBook. ReadyPrice Software, 2011. Access through MICROMEDEX 2.0; Thomson Reuters (Healthcare) Inc. Montvale, NJ. http://thomsonreuters.com/products_services/healthcare/healthcare_products/clinical_deci_support/micromedex_clinical_evidence_sols/med_safety_solutions/red_book/. Accessed February 22, 2012
- Chia S, Gradishar W, Mauriac L, et al. Double-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: results from EFECT. J Clin Oncol 2008;26:1664–70
- Thürlimann B, Hess D, Köberle D, et al. Anastrozole ('Arimidex') versus tamoxifen as first-line therapy in postmenopausal women with advanced breast cancer: results of the double-blind cross-over SAKK trial 21/95--a sub-study of the TARGET (Tamoxifen or 'Arimidex' Randomized Group Efficacy and Tolerability) trial. Breast Cancer Res Treat 2004;85:247–54
- Klepser DG, Huether JR, Handke LJ, et al. Effect on drug utilization and expenditures of a cost-share change from copayment to coinsurance. J Manag Care Pharm 2007;13:765–77
- Mansley EC, Carroll NV, Chen KS, et al. Good research practices for measuring drug costs in cost-effectiveness analyses: a managed care perspective: the ISPOR Drug Cost Task Force report--Part III. Value Health 2010;13:14–17
- BLS data series. Consumer Price Index - All Urban Consumers. Washington, DC, 2012
- Lamerato L, Havstad S, Gandhi S, et al. Economic burden associated with breast cancer recurrence: findings from a retrospective analysis of health system data. Cancer 2006;106:1875–82
- Centers for Medicare & Medicaid Services. Baltimore, MD. Statewide average operating cost-to-charge ratios for urban and rural hospitals (case weighted) March 2000. Medicare program: changes to the hospital inpatient prospective payment systems and fiscal year 2001 rates. http://www.federalregister.gov/articles/2000/08/01/00-19108/medicare-program-changes-to-the-hospitalinpatient-prospective-payment-systems-and-fiscal-year-2001#t-37. Accessed November 21, 2012
- Hortobagyi GN, Piccart M, Burris H, et al. Everolimus for postmenopausal women with advanced breast cancer: updated results of the BOLERO-2 Phase III Trial. Thirty-Fourth Annual CTRC-AACR San Antonio Breast Cancer Symposium -- Dec 6--10, 2011; San Antonio, TX, SABCS abstracts 2011
- Ershler WB, Chen K, Reyes EB, et al. Economic burden of patients with anemia in selected diseases. Value Health 2005;8:629–38
- Dial E, Fournier A, Moyneur E, et al. Frequency and cost of adverse events in renal cell carcinoma (RCC) patients receiving angiogenesis inhibitor therapies. J Clin Oncol 2008;26(Suppl):abstr 14609
- Mauskopf JA, Sullivan SD, Anneman SL, et al. Principles of good practice for budget impact analysis: report of the ISPOR task force on good research practices - budget impact analysis. Value Health 2007;10:336–47
- U.S. Food and Drug Administration. Approved label for exemestane. FDA, Silver Spring, MD, 2011. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.DrugDetails. Accessed October 26, 2011
- U.S. Food and Drug Administration. Approved label for Faslodex (Fulvestrant). FDA, Silver Spring, MD, 2011. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.DrugDetails. Accessed October 26, 2011
- U.S. Food and Drug Administration. Approved label for tamoxifen. FDA, Silver Spring, MD, 2011. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.DrugDetails. Accessed October 26, 2011