
Abstract
Objective:
To evaluate the burden of hyponatremia in terms of hospital resource utilization, costs, and 30-day hospital readmission among patients hospitalized for heart failure (HF) in routine clinical practice.
Methods:
Hyponatremic (HN) patients (≥18 years of age) with HF discharged between January 2, 2007 and March 31, 2010 were selected from the Premier Hospital Database and matched to non-HN HF patients using exact and propensity score matching. Univariate and multivariate statistics were utilized to compare hospital resource utilization (total and intensive care unit (ICU)) and associated costs and 30-day hospital readmission among cohorts.
Results:
The study population included 51,710 subjects (HN = 25,855, non-HN = 25,855). In comparison to the non-HN cohort, length of stay (LOS) (7.7 ± 8.3 vs 6.3 ± 7.6 days, p < 0.001), hospitalization cost ($13,339 ± $19,273 vs $10,475 ± 15,157, p < 0.001), ICU LOS (4.9 ± 5.4 vs 4.2 ± 5.4 days, p < 0.001) and ICU cost ($7195 ± $9522 vs $5618 ± 10,919, p < 0.001) as well as rate of 30-day readmission (all cause: 25.3% vs 22.2%, p < 0.001; hyponatremia-related: 21.4% vs 5.0%, p < 0.001) were greater for the HN cohort. After adjustment, hyponatremia was associated with a 21.5% increase in hospital LOS, a 25.6% increase in hospital cost, a 13.7% increase in ICU LOS and a 24.6% increase in ICU cost. Additionally, hyponatremia was associated with increased risk of ICU admission (Odds Ratio (OR) = 1.58, [CI = 1.37, 1.84], p < 0.001) and 30-day hospital readmission (all cause: OR = 1.19, [CI = 1.14, 1.24], p < 0.001; hyponatremia-related: 5.10 [CI = 4.77, 5.46], p < 0.001).
Limitations:
Laboratory data for serum sodium level are not available in the Premier database and the severity of hyponatremia could not be established, although several patient variables were controlled for in this study by exact and propensity score matching techniques.
Conclusions:
Hyponatremia in HF patients is a predictor of increased hospital resource use and represents a potential target for intervention to reduce healthcare expenditures.
Introduction
In the US, ∼670,000 people are diagnosed with congestive heart failure (HF) every yearCitation1. Hyponatremia, an electrolyte disorder typically characterized by serum sodium concentrations <135 mEq/L, is a frequent co-morbid condition of patients hospitalized for HF with an occurrence ranging between 11.5–27%Citation2–4. Hyponatremia in HF patients can be a consequence of low cardiac output leading to the non-osmotic release of arginine vasopressin (AVP) and subsequent increase in water reabsorption by the kidneys and/or diuretic useCitation5. The condition is a prognostic marker of worsening HFCitation5.
Among clinical trial HF patients and HF patients in routine clinical practice, hyponatremia is a strong predictor of adverse clinical outcomes, hospital readmission and mortalityCitation2–6. In an analysis of several variables—clinical, hemodynamic, and biochemical—serum sodium concentration prior to treatment initiation was the most powerful predictor of cardiovascular mortality, with hyponatremic (HN) HF patients having a 2.3-fold less median length of survival in comparison to normonatremic HF patientsCitation6. Using the OPTIMIZE-HF registry, Gheorghiade et al.Citation4 reported that, among 48,612 patients with HF, hyponatremia was associated with a 19.5% increased risk for in-hospital death and for every 3 mEq/L incremental decrease in serum sodium concentration below 140 mEq/L at admission re-hospitalization and/or death correspondingly increased by 8%. An analysis of 115,969 patients hospitalized for HF reported that those with severe hyponatremia (≤130 mEq/L) and mild hyponatremia (131–135 mEq/L) had 78% and 29% increased odds for mortality, respectively, in comparison to normonatremic patientsCitation7.
In 2010 in the US the overall economic burden attributed to HF was $39.2 billionCitation1. Based on several studies, the high prevalence of hyponatremia in patients with HF and its association with adverse outcomes and greater healthcare usage suggest the condition contributes substantially to the overwhelming economic burden of HFCitation2–4,Citation7. Although these studies imply an association between hyponatremia and an increased healthcare burden, a causal interpretation is limited as studies were either post-hoc analyses of clinical trial patients with HF, a patient population which may not be reflective of HF patients in routine clinical practice, or the study groups significantly differed in clinical characteristics. In the present study, hospital resource utilization, costs, and 30-day hospital readmission were compared among HN and non-HN HF patients with similar patient profiles in order to assess the incremental burden associated with hyponatremia among HF patients in routine clinical practice.
Methods
Study design
This study utilized a hospital database maintained by Premier Inc. (Charlotte, NC), a retrospective, patient-level dataset that includes more than 330 million inpatient discharges from more than 600 US acute care hospitals. Patient level detail includes patient and provider demographics, all ICD-9-CM diagnosis and procedure codes, as well as date-stamped administrative records for all pharmacy, laboratory, imaging, procedures, and supplies.
Patient selection and matching
Patients ≥18 years of age and discharged between January 1, 2007 and March 31, 2010 with a principal discharge diagnosis of congestive heart failure (ICD-9-CM code 428.xx) were identified. Patients were excluded if they had been transferred from another acute care facility, transferred to another acute care or critical access facility, or left against medical advice. Labor and delivery patients, patients classified as observational, and those with no cost information were also excluded. After inclusion criteria were met, patients were then classified as hyponatremic (HN) based on the criterion used in Boscoe et al.Citation8: presence of a secondary diagnosis code of hyponatremia or hyposmolality as indicated through a ICD-9-CM diagnosis code of 276.1x. Comorbidities were summarized for each patient using the modified Deyo-Charlson Comorbidity IndexCitation9. Additionally, reported for each patient are illness severity and risk of mortality, as defined by All Patient Refined Diagnosis Related Groups (3M®APR-DRG) assignment.
HN and control (non-HN) patients were matched using a combination of exact and propensity score matching techniques. Patients were first exact matched on age, gender, hospital geographic region, and Medicare Severity–Diagnosis Related Group (MS-DRG) assignment, which is a classification system developed by the Centers for Medicare and Medicaid Services that identifies hospital activity during an episode of patient care. Propensity score matching was further used to create the final study cohorts for outcomes comparisons. The propensity score model included both patient- and hospital-level covariates selected through research literature and clinical inputs.
Outcome measures and statistical analyses
The primary outcomes for analysis included total and intensive care unit (ICU) hospitalization costs, total and ICU length of stay (LOS), ICU admission rate, and 30-day hospital readmission (all cause and hyponatremia-related). Univariate descriptive statistics were calculated for all patient and hospital covariates, with significance determined by chi-square tests for categorical data and Student t-tests for continuous variables. Multivariate analysis of outcome measures utilized generalized linear models. Due to the skewed nature of LOS and cost data, LOS and cost were analyzed using multivariate regression with a gamma distribution and a log link functionCitation10. Binary outcomes (ICU admission and 30-day readmission) were analyzed using multivariate logistic regression. The analysis accounted for potential confounding factors by inclusion of the following covariates: age group, gender, race, admission source, and Deyo-Charlson Comorbidity Index score. These covariates were previously identified by Wald et al.Citation11, and were verified using likelihood-ratio, Hosmer-Lemeshow goodness of fit, and Concordance c statistics.
Results
Patient population
Of 512,524 patients (≥18 years of age) identified with a principal diagnosis of HF during the study period, 28,728 were HN and 483,796 were non-HN. After applying the exclusion criteria there were 443,819 remaining patients (HN = 25,855, non-HN = 417,964). After matching, the final study population included a total of 51,710 subjects (HN = 25,855, non-HN = 25,855).
Key patient demographic variables are presented in . Mean age for both cohorts was 75.4 years and 55.8% of patient cohorts were female. Patient cohorts differed slightly on race distribution, with a slightly higher percentage of HN patients being white (68.3% vs 62.5%, p < 0.001). The majority of patients were admitted through the emergency department (HN = 80.3%, non-HN = 75.9%, p < 0.001). A greater proportion of HN patients had a 3M®APR-DRG Severity of Illness assignment of 4 (extreme; 17.1% vs 9.9%, p < 0.001) and higher risk for mortality (19.8% vs 12.5%, p < 0.001) as defined by 3M®APR-DRG Risk of Mortality assignment, with mean Deyo-Charlson Comorbidity Index (CCI) scores of 4.7 and 4.8, respectively.
Table 1. Baseline demographics and characteristics for matched cohorts of hyponatremic and non-hyponatremic patients.
Hospital characteristics
There were a total of 446 hospitals represented in both matched cohorts (). Hospital characteristics for cohorts were well balanced with respect to population served (urban: HN = 86.7%, non-HN = 88.4%), teaching status (teaching: HN = 38.1%, non-HN = 38.7%), and bed size.
Table 2. Hospital characteristics of matched cohorts of hyponatremic and non-hyponatremic patients.
Healthcare utilization, readmission, and cost differences among patient cohorts
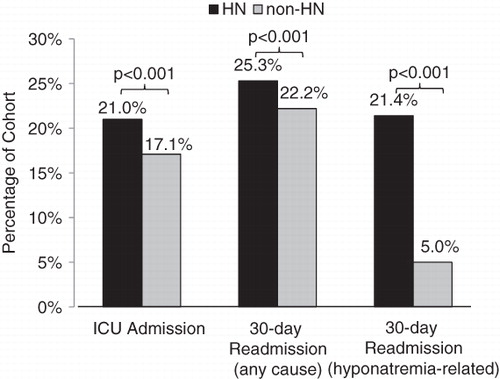
Unadjusted mean LOS was higher for the HN cohort (7.7 ± 8.3 vs 6.3 ± 7.6 days, p < 0.001) as well as mean ICU LOS (4.9 ± 5.4 vs 4.2 ± 5.4 days, p < 0.001), a difference of 1.4 and 0.7 days, respectively (). HN patients utilized hospital resources more which was reflected in their higher mean total cost of hospitalization ($13,339 ± $19,273 vs $10,475 ± $15,157, p < 0.001) and ICU costs ($7195 ± $9522 vs $5618 ± $10,919, p < 0.001; ). HN patients were also more often admitted to the ICU than non-HN patients (21.0% vs 17.1%, p < 0.001) and had a higher rate of 30-day readmission as well (all cause: 25.3% vs 22.2%, p < 0.001; hyponatremia-related: 21.4% vs 5.0%, p < 0.001; ).
Figure 1. Hospital and Intensive Care Unit (ICU) length of stay (LOS) (a) and costs (b) for hyponatremic and non-hyponatremic patient cohorts after matching.
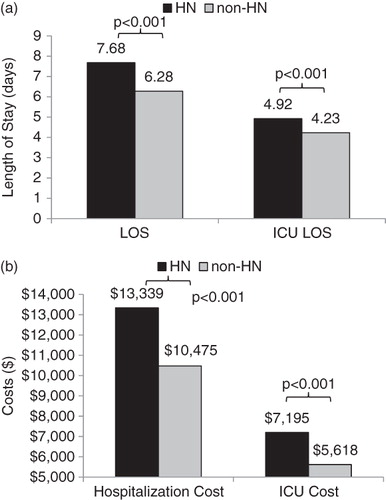
Figure 2. Intensive Care Unit (ICU) admission and 30-day hospital readmission, for any cause and hyponatremia-related for hyponatremic and non-hyponatremic patient cohorts after matching.
Multivariate analysis
After adjusting for patient covariates, HN patients had a 21.5% increase in LOS (confidence interval (CI) = 20.1%, 23.0%, p < 0.001) and an increased mean hospital cost of 25.6% (CI = 23.8%, 27.3%, p < 0.001; ). Similar increases were seen for mean ICU LOS with a 13.7% (CI = 10.0%, 17.6%, p < 0.001) increase and mean ICU cost with a 24.6% (CI = 22.2%, 29.5%, p < 0.001) increase (). Hyponatremia was associated with an increased risk of ICU admission (Odds Ratio (OR) = 1.58, CI = 1.37, 1.84, p < 0.001), as well as readmission within 30 days for any cause (OR = 1.19, CI = 1.14, 1.24, p < 0.001) and hyponatremia-related (OR = 5.10, CI = 4.77, 5.46, p < 0.001; ).
Table 3. Relative increase in healthcare utilization and costs and odds for Intensive Care Unit (ICU) admission and 30-day readmission for hyponatremic patients vs non-hyponatremic patients based on multivariate analysis.
Discussion
The results of this retrospective database study demonstrate that the condition of hyponatremia in HF patients is associated with greater healthcare resource utilization and cost in routine clinical practice. This study also yields more evidence that hyponatremia is a predictor of worsening HF and mortality risk as exemplified by the higher 3M®APR-DRG Severity of Illness and Risk of Mortality assignments for patients in the HN cohort in comparison with the non-HN cohort. Also, the findings of this study are not only consistent, but quite comparable with those of others in which HF patients may have differed in certain characteristics and/or received care in a clinical trial settingCitation3,Citation4,Citation7,Citation12,Citation13.
In this study, hyponatremia was associated with a 1.4 day increase in overall hospital LOS, similar to that reported in a study conducted by Shorr et al.Citation7, which found a 0.7 and 1.28 day greater LOS for HN and severe HN HF patients, respectively, in comparison with normonatremic HF patients. In contrast to our study, the Shorr et al.Citation7 study established hyponatremia severity of the HN patient population and, due to limitations of the data source used in our study, we were unable to confirm the impact of greater hyponatremia severity on healthcare resource utilization as reported by Shorr et al.Citation7 Two large, retrospective studies of hospitalized patients in general reported that HN patients had a significantly greater need for ICU care (4–10%)Citation12,Citation13. In the present study, after adjustment of key patient characteristics, hyponatremia was associated with a 13.7% increase in ICU LOS, which corresponded with a 24.6% increase in ICU cost for HF patients. In addition, HF patients with hyponatremia were found to have a mean increase in hospital cost per admission of $2864, in comparison to non-HN HF patients and, after adjustment, hyponatremia was associated with a 25.6% increase in overall hospital costs. Among 115,969 patients hospitalized for HF, Shorr et al.Citation7 estimated that in-hospital costs attributed to hyponatremia were $509 and for severe hyponatremia were $1133, while Callahan et al.Citation13 reported that, among hospitalized patients in general, patients with mild-to-moderate hyponatremia and those with moderate-to-severe hyponatremia had a $1200 and $3540 increase in cost per admission, respectively, in comparison with non-HN patients.
Readmission rates of HF patients, with and without hyponatremia, have been compared in some other studies, all of which were post-hoc analyses of clinical trial patientsCitation3,Citation14,Citation15. Two of these studies, in which only patients with acute class IV HF were evaluated, reported hyponatremia was associated with a significant increase in readmission rates (up to 20% higher)Citation3,Citation15. After adjusting for patient differences, Gheorghiade et al.Citation14 reported that the risk of death or re-hospitalization for HF patients increased by 8% for each 3 mEq/L decrease in serum sodium concentration below 140 mEq/L at admission. In the current study, after adjusting for patient differences, hyponatremia was associated with an increase risk ranging between 14–24% for early hospital readmission for any cause and over a 5-fold greater risk of going back to the hospital within 30 days for hyponatremia among HF patients.
The Agency for Healthcare Quality and Research (AHRQ) reported in 2008 that 10% of the nearly 40 million hospitalizations in the US were potentially preventableCitation16. Avoidable readmissions are a target for healthcare reform and hospitals with high rates of re-admission within 30 days of patient discharge are currently being monetarily penalizedCitation17. The Centers for Medicare and Medicaid Services now publishes Medicare-certified hospitals’ 30-day re-admission rates for heart attack, heart failure, and pneumonia on its Hospital Compare website, drawing further attention to the topicCitation17. HF patients with hyponatremia represent a patient population in which improvement in inpatient and outpatient care of the condition may effectively avoid recurrent hospitalizations, although this remains to be investigated further, especially in routine clinical practice. A cost-analysis study based on results of the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) trial estimated the cost savings of treating HN HF patients with the AVP V2 receptor antagonist, tolvaptan at $265 per admissionCitation18. It will be important in the future to study in routine clinical practice how to further reduce the cost burden associated with hyponatremia.
Limitations
While this study yielded valuable comparative data on a large population of HF patients with and without hyponatremia, some limitations should be considered when interpreting the results. First, patient data in the Premier database are only representative of inpatient hospital costs and exclude outpatient healthcare utilization and costs. Second, laboratory testing data for serum sodium level are not available in this database and, therefore, the severity of hyponatremia could not be established in the HN HF patient population. Third, although several patient variables, including disease severity and comorbidities, were controlled for in this study by exact and propensity score matching techniques, other covariates which may influence the results of this study were not. These include diuretic usage, other electrolyte abnormalities, and renal function. Another limitation of this study is that, while the Premier database contains information from a large number of hospitals across the US, it is possible that it may not be representative of the entire US population of HN HF patients. Lastly, billing and coding errors and missing data could potentially have occurred, although the large patient population size likely precludes a large impact on the results of this study.
Conclusions
Hyponatremia among HF patients is associated with greater healthcare resource utilization and cost, including greater admittance to the ICU and longer LOS and early readmission rate. This suggests that treatment of this condition may potentially reduce the healthcare burden of patients with HF while improving patient outcomes.
Transparency
Declaration of funding
This research was supported by Otsuka America Pharmaceutical, Inc., Princeton, NJ, which manufactures tolvaptan for the treatment of hyponatremia.
Declaration of financial relationships
AA and Dr SD are consultants for and have received honoraria from Otsuka America Pharmaceutical in connection with conducting this study. RC and KF are employees of Otsuka America Pharmaceutical. JL is an employee of Novosys Health, which has received research funds from Otsuka America Pharmaceutical in connection with conducting this study and development of this manuscript. TL is an employee of Premier Inc., which has received research funds from Otsuka America Pharmaceutical.
Acknowledgments
We would like to acknowledge Melissa Lingohr-Smith from Novosys Health in the editorial support and review of this manuscript. Some aspects of this study were presented as poster presentations at the 15th Annual Scientific Meeting of the Heart Failure Society of America (HFSA), September 18–21, 2011 in Boston, MA.
References
- Centers for Disease Control and Prevention. Heart failure fact sheet. http://www.cdc.gov/DHDSP/data_statistics/fact_sheets/fs_heart_failure.htm. Accessed April 9, 2012
- Chen MC, Chang HW, Cheng CI, et al. Risk stratification of in-hospital mortality in patients hospitalized for chronic congestive heart failure secondary to non-ischemic cardiomyopathy. Cardiology 2003;100:136-42
- Gheorghiade M, Rossi JS, Cotts W, et al. Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE Trial. Arch Intern Med 2007;167:1998-2005
- Gheorghiade M, Abraham WT, Albert NM, et al. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE-HF registry. Eur Heart J 2007;28:980-8
- Romanovsky A, Bagshaw S, Rosner MH. Hyponatremia and congestive heart failure: a marker of increased mortality and a target for therapy. Intern J Nephrol 2011;2011:732-46
- Lee WH, Packer M. Prognostic importance of serum sodium concentration and its modification by converting-enzyme inhibition in patients with severe chronic heart failure. Circulation 1986;73:257-67
- Shorr AF, Tabak YP, Johannes RS, et al. Burden of sodium abnormalities in patients hospitalized for heart failure. Cong Heart Fail 2011;17:1-7
- Boscoe A, Paramore C, Verbalis JG. Cost of illness of hyponatremia in the United States. Cost Eff Resour Alloc 2006;4:1-11
- Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 1992;45:613-9
- Nixon RM, Thompson SG. Parametric modeling of cost data in medical studies. Statist Med 2004;23:1311-31
- Wald R, Jaber BL, Price LL, et al. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med 2010;170:294-302
- Zilberberg MD, Exuzides A, Spalding J, et al. Epidemiology, clinical and economic outcomes of admission hyponatremia among hospitalized patients. Curr Med Res Opin 2008;24:1601-8
- Callahan MA, Do HT, Caplan DW, et al. Economic impact of hyponatremia in hospitalized patients: a retrospective cohort study. Postgrad Med 2009;121:186-91
- Gheorghiade M, Abraham WT, Albert NM, et al. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE-HF registry. Eur Heart J 2007;28:980-8
- Dunlay SM, Gheorghiade M, Reid KJ, et al. Critical elements of clinical follow-up after hospital discharge for heart failure: insights from the EVEREST trial. Eur J Heart Fail 2010;12:367-74
- Stranges E, Stocks C. Potentially preventable hospitalizations for acute and chronic conditions, 2008. HCUP Statistical Brief #99. Rockville, MD: Agency for Healthcare Research and Quality, 2010. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb99.jsp. Accessed April 10, 2012
- Stone J, Hoffman, GJ. Medicare hospital readmissions: issues, policy options and PPACA. (R40972). Washington, DC: Congressional Research Service, 2010. http://www.hospitalmedicine.org/AM/pdf/advocacy/CRS_Readmissions_Report.pdf. Accessed May 5, 2012
- Chiong JR, Kim S, Lin J, et al. Evaluation of costs associated with tolvaptan-mediated length-of-stay reduction among heart failure patients with hyponatremia in the US, based on the EVEREST trial. J Med Econ 2012;15:276-84