
Abstract
Objective:
To evaluate the cost-effectiveness of distributing naloxone to illicit opioid users for lay overdose reversal in Russian cities.
Method:
This study adapted an integrated Markov and decision analytic model to Russian cities. The model took a lifetime, societal perspective, relied on published literature, and was calibrated to epidemiologic findings.
Results:
For each 20% of heroin users reached with naloxone distribution, the model predicted a 13.4% reduction in overdose deaths in the first 5 years and 7.6% over a lifetime; on probabilistic analysis, one death would be prevented for every 89 naloxone kits distributed (95% CI = 32–260). Naloxone distribution was cost-effective in all deterministic and probabilistic sensitivity analyses and cost-saving if resulting in a reduction in overdose events. Naloxone distribution increased costs by US$13 (95% CI = US$3–US$32) and QALYs by 0.137 (95% CI = 0.022–0.389) for an incremental cost of US$94 per QALY gained (95% CI = US$40–US$325). In a worst-case scenario where overdose was rarely witnessed and naloxone was rarely used, minimally effective, and expensive, the incremental cost was US$1987 per QALY gained. If national expenditures on drug-related HIV, tuberculosis, and criminal justice were applied to heroin users, the incremental cost was US$928 per QALY gained.
Conclusions:
Naloxone distribution to heroin users for lay overdose reversal is highly likely to reduce overdose deaths in target communities and is robustly cost-effective, even within the constraints of this conservative model.
Introduction
Heroin overdose accounts for about half of mortality among heroin users worldwideCitation1, but is believed to be an even greater driver of morbidity and mortality amongst heroin users in the Russian FederationCitation2. Neither agonist maintenance therapyCitation3,Citation4 nor supervised injection facilitiesCitation5, which have both been associated with reduced overdose death, are authorized in RussiaCitation6. Moreover, emergency medical services (EMS) are limited in scope and availability in many areas of Russia, and uncommonly utilized due in part to legal and cost concernsCitation2. Distribution of the opioid antagonist, naloxone, for lay administration in the event of overdose has emerged both within Russia and around the world as a promising approach to directly addressing opioid overdoseCitation6–8. Naloxone is a safe, effective, short-acting opioid antagonist for intravenous, intramuscular, subcutaneous, or intra-nasal administration to reverse opioid overdose. Naloxone is traditionally carried by EMS in localities where opioid overdose is encountered and earlier administration of naloxone is associated with fewer overdose-related complicationsCitation9. Naloxone distribution is targeted at opioid users or anyone, including family members, who might witness an opioid overdose and includes brief education about overdose risks and management. Naloxone ‘kits’ in Russia are generally wallet-sized packets containing two administrations of naloxone, syringes, and a brochure.
Naloxone distribution programs have been shown to train drug users to respond effectively to overdoseCitation10, result in frequent successful opioid overdose reversalsCitation11–13, and be associated with a decline in overdose mortality in communitiesCitation14–16. Nonetheless, heroin users who survive overdose frequently suffer future overdosesCitation17 and policy-makers may be concerned about the overall societal cost of heroin useCitation17. To address these concerns, and other distinct circumstances in Russia, we adapted a mathematical model of naloxone distribution originally designed for the US to Russian cities.
Methods
Model
A detailed description of the model development following methods guidance from Stout et al.Citation18 can be found in the appendix of the original paperCitation19. Briefly, we constructed a Markov model with an integrated decision analytic model (see ) in Microsoft Excel 2010™ to estimate the impact of distributing naloxone to heroin users on costs and utility with annual transitions and standard background mortality. The model takes a societal perspective over a lifetime horizon. Input parameters and ranges can be found in ; instantaneous rates were transformed to probabilitiesCitation20. Heroin users entered the model in ‘Heroin use’ and could discontinue and relapseCitation21,Citation22, overdose, or die for other reasonsCitation8. The overdose event was modeled separately and developed with the add-in TreePlan™ (Decision Toolworks, San Francisco, CA). The model produced three cycles of overdose, given the well-documented elevation in risk of overdose among persons who have previously overdosedCitation17.
Figure 1. Model of naloxone distribution to heroin. EMS = emergency medical services. OD = overdose. Markov model with annual cycles and unlisted background mortality. Outcome of overdose events determined by decision analytic tree on right of figure. *Receive naloxone is adjusted in sensitivity analyses by the social network modifier.
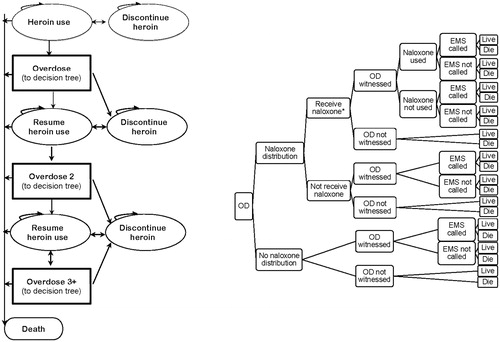
Table 1. Naloxone distribution model parameters.
Adaptation of model
Adaptation of the model included both structural changes and identification of parameters specific to Russia. With regard to structure, we adjusted the starting age to 18 years, the average age of initiating heroin use in RussiaCitation23, and calculated age-specific background mortality from 2010 Russian Federation mortality tables. In addition, we reduced the role of EMS in managing overdose such that EMS had no impact on survival, and increased the role of witnesses in managing overdose such that any overdose that was witnessed had a higher likelihood of survival regardless of interventions employed. These changes were based on research in Russia suggesting that, in contrast to the USCitation19, survival with EMS care is similar or possibly lower (0.90) than survival for those who do not receive EMS care (0.93)Citation23 (perhaps due to delayed or unavailable EMS care, although the absence of naloxone in many ambulances may be another causeCitation2). Given the high rate of witnessing overdose, we assumed that witnessed overdoses had a higher rate of survival than unwitnessed events. EMS thus affected only cost in the adapted model.
We adjusted several parameters to account for different epidemiologic findings, availability of healthcare services, and costs. Given the small studies upon which several parameters were based, the model was calibrated to parallel findings from epidemiologic studies from Russia where available and international sites if no other sources were available (see )Citation17,Citation23–31. Studies have demonstrated high rates of discontinuing heroin use in Russia, but rarely for more than 6 monthsCitation32, and few IDUs in a St Petersburg study were able to abstain for over a yearCitation33 in a setting with no legal agonist maintenance services and very limited availability of other treatment servicesCitation34; thus we assumed that relapse to heroin use would be much higher than US-based estimates of 50% relapse over 5 yearsCitation35. We assumed that 35% would relapse each year, although we maintained an age-based reduction in the risk of relapseCitation36, resulting in a median duration of heroin use among survivors of 31 years (much longer than the US median of 15 years of useCitation31). Although a US-based study found high rates of enrollment in treatment after overdoseCitation37, we did not incorporate an increased likelihood of abstinence after overdose into the baseline model due to limited treatment availability in Russia.
Table 2. Key epidemiologic parameters for model calibration.
We assumed an annual rate of 16% for first-time overdose that declined with age such that the risk was halved at 14 years of heroin useCitation38. This rate was higher than the baseline rate for the US model in order to match epidemiologic data suggesting higher rates of overdose and overdose death (see ); one possible explanation for a differential rate of first-time overdose would be the risks associated with frequent use of home-made opioids in RussiaCitation39. The risks of a second and further overdoses were carried from the original modelCitation38. The increasing risk of overdoseCitation40,Citation41, as well as the declining risk of a first-time overdoseCitation38, were literature estimates, but were also necessary to approximate epidemiologic findings that 10–25% of heroin users overdose each yearCitation17,Citation27,Citation28,Citation42,Citation43, yet only approximately two-thirds of Russian heroin users report ever overdosingCitation23,Citation24.
Based on Russian data, overdoses were estimated to be witnessed 90% of the timeCitation23, with a lower limit of 32% based on a study of fatal overdoses in San FranciscoCitation44. In sensitivity analysis, a social network modifier accounted for variations in the likelihood that heroin users would use with others who had been reached by the naloxone distribution program. The use of EMS is low in Russia (ranging from 13–16%Citation23) and, based on the only published study, we assumed no change in the likelihood of calling EMS if naloxone was administeredCitation45.
The estimated risk of an overdose resulting in death in Russia is 9.3%Citation24, yet the mean age of overdose death is generally in the fourth decade of lifeCitation24,Citation30,Citation46, suggesting that overdoses are more likely to be fatal in later years of opioid use. First-time overdoses, thus, had a mortality rate of 7% when witnessed and 10% when unwitnessed, with an absolute 1.5% increase in the risk of death for the second overdose, and 3% for all subsequent overdoses, resulting in an annual risk of mortality from overdose among active heroin users of ∼0.6% in the early years of use, peaking at 1.9% after 30 years of use. As the mechanism for increased risk of death with recurrent overdoses is not well understood, we applied the same increased risk of death with recurrent overdoses to those receiving naloxone by calculating a relative risk reduction in mortality from these interventions.
Costs
Costs were converted to US dollars, valued at 2010 levels, and discounted 5% per annum, in accordance with methods guidanceCitation47. Naloxone, most commonly distributed as two doses, is remarkably inexpensive in Eurasia, ranging from US$0.61–US$0.89 per 0.4 mg vial in 2010. The total cost of running a naloxone distribution program in Russia ranges from ∼US$9000 to distribute 2000 vials to 304 clients in ChapayevskCitation48 to US$12,700 to distribute 4745 vials to 656 clients in Naberezhnye ChelnyCitation49; for an average annual total cost of US$4 per vial of naloxone distributed and US$24 per client served. As naloxone expires after 24 months, we estimated a total cost of US$8 per kit (two vials) distributed every 2 years, with additional replacement kits after each overdose.
The baseline total cost of EMS was estimated based on costs in Moscow, the most expensive city in Russia, as US$235, including ambulance (5000 RUR/US$161)Citation50 and emergency room care (2300 RUR/US$74)Citation51. The lower limit included only ambulance costs. Because witnesses in Russia are much less likely to call EMS, we assumed that all cases receiving EMS care were severe enough to warrant transport to the emergency room.
Quality-adjusted life years
Quality-adjusted life years (QALYs) were discounted at 5% per annum. The estimate of baseline quality-of-life for this analysis was taken from a study of health-related quality-of-life (HRQoL) among persons with depression in Russia, for which the control group utility was 0.814 by the EuroQol questionnaire (EQ-5D)Citation52. This value was adjusted with a multiplier of the relative utility among injection drug usersCitation53,Citation54, with a conservative estimate of increased quality-of-life during recoveryCitation54.
Analysis
We conducted deterministic and probabilistic analyses of health outcomes (overdose and overdose death rates) and cost-effectiveness (additional cost per QALY gained over the life of the model).
We conducted one-way deterministic sensitivity analyses on all variables and several analyses to evaluate specific scenarios. To evaluate cohorts of heroin users averaging 28 and 38 years of age, we ran the no naloxone model to that age to determine the proportion of the population in each ‘stage’ of heroin use, assuming all heroin users were active users; we then adjusted background mortality and ran the model. To account for the potential cost of outreach efforts, we conducted an analysis increasing the cost of naloxone kits by 50% for each additional 10% of heroin users reached by the program. We also developed ‘worst-case’ and ‘best-case’ scenarios involving extremes of multiple parameters to address uncertainty in the utilization and effects of distributed naloxone. Finally, we ran a probabilistic analysis of 10,000 Monte Carlo simulations; all model parameters were simultaneously varied across ranges defined in with distributions considered normal for proportions and utilities, log-normal for costs, and beta for transition states. We generated confidence intervals from the probabilistic simulations, defined as those values above and below the 2.5% and 97.5% ranges of results. In addition, results were converted to incremental net benefits (μNaloxone − μNo-naloxone, where μ = [(Willingness to pay) × QALYs] − Cost), and a cost-effectiveness acceptability curve was developedCitation55.
We applied the ‘cost’ of heroin use to the utility estimate, in accord with standard economic analyses. However, to address potential concerns among policy-makers that heroin users are too expensive to warrant efforts to improve survival, we developed an alternate cost-effectiveness acceptability curve assuming that heroin users are a net cost to society in addition to their reduced utility and irrespective of any productivity. In the US model, we estimated a 2011 annual cost of US$1000 per heroin user for healthcare and research costs and US$3300 if criminal justice costs were includedCitation56. There is no central estimate in Russia, thus we utilized estimated expenditures on HIV and tuberculosis as a surrogate for healthcare costs. Of the estimated 1.8 million IDUs in Russia, ∼37% are living with HIV, and this risk factor accounted for 62% of new HIV cases in 2009Citation57. There were 980,000 persons living with HIV in RussiaCitation58 and an estimated US$777 million was spent on HIV services in 2008Citation5Citation8. The actual proportion of HIV monies spent on IDUs, sex workers, and men-who-have-sex-with-men is estimated to be only 4.4%Citation59, amounting to a maximum HIV-related expenditure of US$19 per heroin user annually. Under the extreme assumption that all IDUs use opioids and receive proportionate HIV funding, heroin in Russia cost ∼US$267 per user annually in HIV-related expenditures. With regard to tuberculosis, 4–14% of patients with tuberculosis in St Petersburg were drug-dependentCitation60, and an estimated US$1.2 billion was spent on tuberculosis in RF in 2010Citation61, thus tuberculosis expenditures constitute up to US$93 per IDU annually. To mirror US estimates, we assumed that criminal justice costs were twice the maximum expenditures on HIV and tuberculosis ($720), resulting in an estimate of US$832 per annum based on current expenditures and an upper limit of US$1080 per annum, assuming maximal expenditures based on need.
Model validation
Details regarding calibration of the original model can be found in the appendix of the original paperCitation19. A similar process was undertaken to calibrate the model to be concordant with epidemiologic findings from Russia (). The final model predicted that just over 50% of heroin users would continue to use after 31 years, substantially longer than US estimates that heroin use continues for an average of 15 yearsCitation26,Citation62 due to limited treatment availability. The model predicted an average rate of overdose of 17.7% per year, higher than US estimatesCitation17,Citation27,Citation28, but a low estimate based on data from RussiaCitation23, with the greatest number of overdoses occurring early in a heroin user’s career. The model predicted an average all-cause mortality rate of 2.7% per year, increasing with age among active users. The model predicted an average rate of overdose death among active heroin users of 1.7%, somewhat low compared to literature estimates in excess of 2% per annumCitation2. The model matched the literature estimate of a witnessed overdose resulting in death in Russia of 9.3%Citation23. The predicted median age of overdose death was 36 years, consistent with findings that young heroin users overdose frequently, but the median age of overdose death is in the fourth decade of lifeCitation23,Citation29. The model predicted that, among overdose deaths, an average of ∼17% received medical attention, consistent with estimates from other countries that one-fifth of overdose deaths received EMS careCitation30. The model predicted a 14.4% chance of a naloxone kit being used for overdose reversal, consistent with passively collected program reports from clients returning to obtain another naloxone kit (i.e., number of kits used to reverse overdose/total number of kits dispensed)Citation11,Citation15,Citation63. Forty years after beginning heroin use, 52% of the initial cohort had died and 30% had discontinued use.
Results
Population outcomes
On deterministic analysis, naloxone distribution prevented 7.6% of overdose deaths for each 20% of the heroin using population reached by the program (see and ). We estimate that one overdose death was prevented for every 54 naloxone kits distributed (i.e., ‘number needed to treat’ = 54). On probabilistic analysis, naloxone distribution prevented 7.2% of overdose deaths (95% CI = 1.1–29.5%), with a number needed to treat of 89 (95% CI = 32–260). Naloxone distribution resulted in a reduced rate of overdose death among the full cohort and among active heroin users over the lifetime in all simulations, with a 2.5% increase in recovered heroin users and 3.5% increase in the number of overdoses.
Figure 2. Reduction in overdose death rate from naloxone distribution for lay overdose reversal. Deterministic results represented by solid lines and 2.5% and 97.5% limits of the probabilistic analysis are represented by the dashed lines. Absolute rates were adjusted by the number of active heroin users to represent the effect in a community of users.
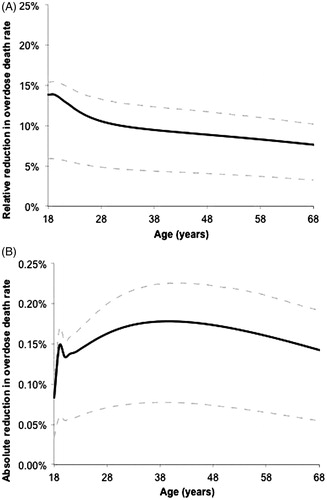
Table 3. Sensitivity analyses.
Cost-effectiveness
Naloxone distribution was cost-effective in our base-case and all sensitivity analyses, with an incremental cost of US$71 per QALY gained ( and Supplementary Figure). Cost-effectiveness was insensitive to the age of targeted users. Cost-effectiveness was somewhat sensitive to the efficacy of lay-administered naloxone at preventing overdose death and the cost of naloxone, but was relatively insensitive to other parameters. If naloxone kit costs increase with expanded coverage, the incremental cost per QALY gained would modestly increase. Naloxone was dominant only if resulting in fewer overdose events through a hypothetical behavior change mechanismCitation64. A worst-case scenario, in which the likelihood of an overdose being witnessed, the efficacy of naloxone, and the likelihood of naloxone being carried at an overdose were minimized and the cost of naloxone was tripled, resulted in an incremental cost of US$2605 per QALY gained.
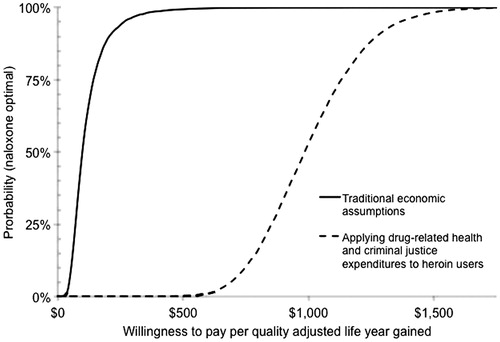
Results from the probabilistic sensitivity analysis were similar to the base case findings. Naloxone distribution increased cost by US$13 (95% CI = US$3–US$32) and QALYs by 0.137 (95% CI = 0.022–0.389) for an incremental cost of US$94 per QALY gained (95% CI = US$40–US$325) (). If we assumed that heroin users are a net cost to society beyond the scope of any other health conditions, naloxone resulted in an incremental cost of US$1000 per QALY gained (95% CI = US$644–US$1450; US$928 on deterministic analysis). See Supplementary Table for absolute outcomes of selected analyses.
Figure 3. Cost-effectiveness acceptability curve of naloxone distribution. y-axis represents the probability that naloxone distribution is preferred at willingness to pay defined on x-axis.
Discussion
We set out to investigate the cost-effectiveness of naloxone distribution in Russian cities by adapting a previously published model and using Russian data as available. Naloxone distribution is likely to reduce opioid overdose mortality in Russia at minimal cost, even under conservative assumptions. Naloxone remained cost-effective if lay administration at a witnessed overdose produced essentially any improvement in survival. However, the reductions estimated in this model were substantially less than real-world reductions in community-level overdose mortality observed concordant with expanded naloxone distribution in several regionsCitation11,Citation13,Citation15,Citation16,Citation65. This difference suggests that the true impact of naloxone may be in excess of our baseline model.
These results are largely consistent with the US analysis, although naloxone distribution may produce greater benefit at a lower cost in Russia. Overdose in Russia is believed to be more frequent, more often witnessed (possibly due to more common family and group living among drug usersCitation66), and less likely to receive medical attention, resulting in an environment in which lay administered naloxone can have a dramatic impact on mortality. The costs of naloxone distribution, EMS care, and healthcare for drug users is much lower in Russia than the US, resulting in a comparatively greater cost-effectiveness, although making naloxone distribution less likely to result in a cost saving from reduced emergency medical care. Overall, these results suggest that naloxone distribution, while generally cost-effective, is even more likely to result in health benefits in regions where heroin users have less access to medical services.
Saving the lives of heroin users may not be a priority for some policy-makers, and may in fact appear to add to state expenditures in unsustainable ways. To address this, we conducted a scenario analysis considering heroin users as a net cost to society. This analysis is not consistent with traditional economic analyses, as we ‘double-charged’ heroin users by reducing their utility (the denominator of the equation) and increasing their costs (the numerator). We do not advocate this approach to economic analyses for drug users as such an approach may codify the stigma of drug use. Nonetheless, naloxone distribution remained cost-effective even under such assumptions.
Limitations
Baseline results may under-estimate the full benefit of naloxone. Some parameters had high degrees of uncertainty, thus we conducted sensitivity and probabilistic analyses and provided confidence intervals. Some parameters relied on data from outside of Russia, including the estimated efficacy of administered naloxone. There are no estimates of quality-of-life among heroin users in Russia, thus we relied upon similar sources as other authors conducting cost analyses, but based our baseline estimate on the product of those estimates and an estimate of the quality-of-life of the general population of Russia. We did not incorporate possible ancillary benefits of naloxone distribution, such as reduced drug use and risk behaviorsCitation67, but did evaluate the latter possibility in a sensitivity analysis. In addition, our model assumed the existence of low-threshold services for heroin users within which naloxone distribution could be embedded; costs may be higher for de novo programs, an increasing concern in Russia as drug service programs have faced major challengesCitation68. Finally, the model relied on epidemiologic data to represent an average of a host of factors that may influence overdose rates, such as poly-drug use, policing tactics, substance use disorder treatment program availability, and changes in heroin supply. Models incorporating such parameters, as this field of research develops, may better predict the impact of overdose interventions.
Conclusions
In summary, this analysis of naloxone distribution to heroin users for lay overdose reversal in Russia suggests that the intervention may be highly cost-effective, even under conservative assumptions.
Transparency
Declaration of funding
Adaptation of this model to Russia was supported by the Open Society Foundation; the funder had no role in the design of the study or preparation of the manuscript. The authors take full responsibility for all elements of the study and manuscript.
Declaration of financial/other relationships
The authors declare no financial, employment, or other significant relevant relationships. JME Peer Reviewers on this manuscript have no relevant financial or other relationships to disclose.
Supplementary Material
Download PDF (145.1 KB)Acknowledgments
The authors declare no assistance in the preparation of this article.
References
- Sporer KA. Acute heroin overdose. Ann Intern Med 1999;130:584-90
- Coffin PO. Overdose: a major cause of preventable death in central and Eastern Europe in Central Asia: recommendations and overview of the situation in Latvia, Kyrgyzstan, Romania, Russia and Tajikistan. Vilnius, Lithuania: Eurasian Harm Reduction Network, 2008
- Auriacombe M, Franques P, Tignol J. Deaths attributable to methadone vs buprenorphine in France. JAMA 2001;285:45
- Rhodes T, Sarang A. Drug treatment and the conditionality of HIV treatment access: a qualitative study in a Russian city. Addiction 2012;107:1827-36
- Marshall BD, Milloy MJ, Wood E, et al. Reduction in overdose mortality after the opening of North America's first medically supervised safer injecting facility: a retrospective population-based study. Lancet 2011;377:1429-37
- Coffin PO, Sherman S, Curtis M. Underestimated and overlooked: a global review of drug overdose and overdose prevention. London, England: International Harm Reduction Association, 2010
- Strang J, Kelleher M, Best D, et al. Emergency naloxone for heroin overdose. BMJ 2006;333:614-5.
- Sporer KA, Kral AH. Prescription naloxone: a novel approach to heroin overdose prevention. Ann Emerg Med 2007;49:172-7
- Gonzva J, Prunet B, Deniel C, et al. Early antidote use associated with noninvasive ventilation in prehospital treatment of methadone intoxication. Am J Emerg Med 2013;31:448 e5-6.
- Green TC, Heimer R, Grau LE. Distinguishing signs of opioid overdose and indication for naloxone: an evaluation of six overdose training and naloxone distribution programs in the United States. Addiction 2008;103:979-89
- Doe-Simkins M, Walley AY, Epstein A, et al. Saved by the nose: bystander-administered intranasal naloxone hydrochloride for opioid overdose. Am J Public Health 2009;99:788-91
- Piper TM, Stancliff S, Rudenstine S, et al. Evaluation of a naloxone distribution and administration program in New York City. Subst Use Misuse 2008;43:858-70
- Enteen L, Bauer J, McLean R, et al. Overdose prevention and naloxone prescription for opioid users in San Francisco. J Urban Health 2010;87:931-41
- Sherman SG, Gann DS, Scott G, et al. A qualitative study of overdose responses among Chicago IDUs. Harm Reduct J 2008;5:2-6
- Maxwell S, Bigg D, Stanczykiewicz K, et al. Prescribing naloxone to actively injecting heroin users: a program to reduce heroin overdose deaths. J Addict Dis 2006;25:89-96
- Paone D, Heller D, Olson C, et al. Illicit drug use in New York City. NYC Vital Signs New York, NY: Department of Mental Health and Hygeine, 2010. p 1-4
- Coffin PO, Tracy M, Bucciarelli A, et al. Identifying injection drug users at risk of nonfatal overdose. Acad Emerg Med 2007;14:616-23
- Stout NK, Knudsen AB, Kong CY, et al. Calibration methods used in cancer simulation models and suggested reporting guidelines. PharmacoEconomics 2009;27:533-45
- Coffin PO, Sullivan SD. Cost-effectiveness of distributing naloxone to heroin users for lay overdose reversal. Ann Intern Med 2013;158:1-9
- Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation. Oxford: Oxford University Press, 2006
- Huo D, Bailey SL, Ouellet LJ. Cessation of injection drug use and change in injection frequency: the Chicago Needle Exchange Evaluation Study. Addiction 2006;101:1606-13
- Bruneau J, Brogly SB, Tyndall MW, et al. Intensity of drug injection as a determinant of sustained injection cessation among chronic drug users: the interface with social factors and service utilization. Addiction 2004;99:727-37
- Sergeev B, Karpets A, Sarang A, et al. Prevalence and circumstances of opiate overdose among injection drug users in the Russian Federation. J Urban Health 2003;80:212-9
- Grau LE, Green TC, Torban M, et al. Psychosocial and contextual correlates of opioid overdose risk among drug users in St. Petersburg, Russia. Harm Reduct J 2009;6:17-28
- Green TC, Grau LE, Blinnikova KN, et al. Social and structural aspects of the overdose risk environment in St. Petersburg, Russia. Int J Drug Policy 2009;20:270-6
- Kwon JA, Iversen J, Maher L, et al. The impact of needle and syringe programs on HIV and HCV transmissions in injecting drug users in Australia: a model-based analysis. J Acquir Immune Defic Syndr 2009;51:462-9
- Ochoa KC, Davidson PJ, Evans JL, et al. Heroin overdose among young injection drug users in San Francisco. Drug Alcohol Depend 2005;80:297-302
- Jenkins LM, Banta-Green CJ, Maynard C, et al. Risk factors for nonfatal overdose at Seattle-area syringe exchanges. J Urban Health 2011;88:118-28
- Galea S, Coffin PO. Drug overdose: new insights, innovative surveillance, and promising interventions. J Urban Health 2003;80:186-8
- Zador D, Sunjic S, Darke S. Heroin-related deaths in New South Wales, 1992: toxicological findings and circumstances. Med J Aust 1996;164:204-7
- Wu LT, Woody GE, Yang C, et al. Differences in onset and abuse/dependence episodes between prescription opioids and heroin: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Subst Abuse Rehabil 2011;2011:77-88
- Open Health Institute. Harm reduction programs in the civilian and prison sectors of the Russian Federation: assessment of best practices. Moscow: World Bank, 2006
- Musatov VA. Abstinence from drugs vs reducing harm. Sixth School for Journalists Writing on Health Issues. Pushkino School for Journalism: Pushkino, Russia, 2006
- Cohen J. No opiate substitutes for the masses of IDUs. Science 2010;329:165-7
- Hser YI. Drug use careers: recovery and mortality. In Substance Abuse and Mental Health Services Administration, Office of Applied Studies. Substance use by older adults: estimates of future impact on the treatment system. OAS Analytic Series #A-21, DHHS Publication No. (SMA) 03-3763. Rockville, MD: SAMHSA 2002
- Evans JL, Hahn JA, Lum PJ, et al. Predictors of injection drug use cessation and relapse in a prospective cohort of young injection drug users in San Francisco, CA (UFO Study). Drug Alcohol Depend 2009;101:152-7
- Pollini RA, McCall L, Mehta SH, et al. Non-fatal overdose and subsequent drug treatment among injection drug users. Drug Alcohol Depend 2006;83:104-10
- Darke S, Williamson A, Ross J, et al. Patterns of nonfatal heroin overdose over a 3-year period: findings from the Australian treatment outcome study. J Urban Health 2007;84:283-91
- Abdala N, Grund JP, Tolstov Y, et al. Can home-made injectable opiates contribute to the HIV epidemic among injection drug users in the countries of the former Soviet Union? Addiction 2006;101:731-7
- Darke S, Mills KL, Ross J, et al. Rates and correlates of mortality amongst heroin users: findings from the Australian Treatment Outcome Study (ATOS), 2001–2009. Drug Alcohol Depend 2011;115:190-5
- Stoove MA, Dietze PM, Jolley D. Overdose deaths following previous non-fatal heroin overdose: record linkage of ambulance attendance and death registry data. Drug Alcohol Rev 2009;28:347-52
- Milloy MJ, Kerr T, Mathias R, et al. Non-fatal overdose among a cohort of active injection drug users recruited from a supervised injection facility. Am J Drug Alcohol Abuse 2008;34:499-509
- Gossop M, Griffiths P, Powis B, et al. Frequency of non-fatal heroin overdose: survey of heroin users recruited in non-clinical settings. BMJ 1996;313:402
- Davidson PJ, McLean RL, Kral AH, et al. Fatal heroin-related overdose in San Francisco, 1997-2000: a case for targeted intervention. J Urban Health 2003;80:261-73
- Coffin PO. Overdose and femoral injection among Seattle-area injection drug users. In: National Institute on Drug Abuse, ed. Epidemiologic trends in drug abuse. Proceedings of the Community Epidemiology Work Group. Rockville, MD, June 2011
- Coffin PO, Galea S, Ahern J, et al. Opiates, cocaine and alcohol combinations in accidental drug overdose deaths in New York City, 1990–98. Addiction 2003;98:739-47
- Avksentieva MV, Antonova NV, Arutyunov GP, et al. Procedure for clinical and economic evaluation of drug lists that are submitted for reimbursement coverage from public health care budget. Russia: Research center for clinical and economic evaluation and pharmacoeconomics of the Russian State Medical University; 2010
- Tsarev SA. Annual Report: preventing opiate overdose among injecting drug users in Chapayevsk. Chapayevsk, Russian Federation: Open Society Institute, 2010
- Gorbunova Y. Summary of naloxone distribution activities. Naberezhnye: Tamur Islamov Charitable Fund, 2010
- Tufts G. Return of the ambulance. Moscow, Russia: Rossijskaya Gazeta, 2011
- Russian Federation Ministry of Health and Social Development. Health/Medical Insurance; Information Letter on the formation and economic justification of territorial programs providing government guarantees for free healthcare for Russian citizens in 2011. Moscow, Russia: Russian Federation Ministry of Health and Social Development; 2012
- Winter Y, Epifanova-Bertschi N, Sankowski R, et al. Health-related quality of life and its determinants in the urban Russian population with major depressive disorder: a cross-sectional study. Int J Psychiatry Med 2012;43:35-49
- Nosyk B, Sun H, Guh DP, et al. The quality of eight health status measures were compared for chronic opioid dependence. J Clin Epidemiol 2010;63:1132-44
- Pyne JM, Tripathi S, French M, et al. Longitudinal association of preference-weighted health-related quality of life measures and substance use disorder outcomes. Addiction 2011;106:507-15
- Fenwick E, Claxton K, Sculpher M. Representing uncertainty: the role of cost-effectiveness acceptability curves. Health Econ 2001;10:779-87
- Tamatsukuri S, Suzuki T, Kasai K, et al. [A novel RNA capture method for the extraction of HCV-RNA]. Kansenshogaku Zasshi 1996;70:479-84
- United States Agency for International Development. Russia: HIV/AIDS Health Profile. Moscow, Russia: USAID/Russia; 2010. p 4
- Joint United Nations Programme on HIV/AIDS. Global Report: UNAIDS Report on the Global AIDS Epidemic 2010. Geneva: Joint United Nations Programme on HIV/AIDS, 2010
- Williams-Sherlock M. Universal access to HIV prevention, treatment, care, and support: 2011 Progress Report, Europe and Central Asia. Geneva: Joint United Nations Programme on HIV/AIDS, 2012
- Krupitsky EM, Zvartau EE, Lioznov DA, et al. Co-morbidity of infectious and addictive diseases in St. Petersburg and the Leningrad Region, Russia. Eur Addict Res 2006;12:12-19
- World Health Organization. Global Tuberculosis Control: Russian Federation Country Profile. Geneva: World Health Organization, 2011
- Maher L, Jalaludin B, Chant KG, et al. Incidence and risk factors for hepatitis C seroconversion in injecting drug users in Australia. Addiction 2006;101:1499-508
- Galea S, Worthington N, Piper TM, et al. Provision of naloxone to injection drug users as an overdose prevention strategy: early evidence from a pilot study in New York City. Addict Behav 2006;31:907-12
- Coffin PO, Coffin LM, Fitzpatrick T, et al. Drug overdose, lay naloxone, and HIV risk behaviors among persons who inject drugs. XIX International AIDS Conference. Washington, DC, 2012. Abstract#MOPE218
- McAuley A, Best D, Taylor A, et al. From evidence to policy: The Scottish national naloxone programme. Drugs Educ Prev Policy 2012;19:309-19
- Wall M, Schmidt E, Sarang A, et al. Sex, drugs and economic behaviour in Russia: a study of socio-economic characteristics of high risk populations. Int J Drug Policy 2011;22:133-9
- Mackesy-Amiti ME, Ouellet LJ, Golub ET, et al. Predictors and correlates of reduced frequency or cessation of injection drug use during a randomized HIV prevention intervention trial. Addiction 2011;106:601-8
- The future of harm reduction programmes in Russia. Lancet 2009;374:1213
- Wagner KD, Valente TW, Casanova M, et al. Evaluation of an overdose prevention and response training programme for injection drug users in the Skid Row area of Los Angeles, CA. Int J Drug Policy 2010;21:186-93
- Davidson PJ, Ochoa KC, Hahn JA, et al. Witnessing heroin-related overdoses: the experiences of young injectors in San Francisco. Addiction 2002;97:1511-6
- Darke S, Ross J, Hall W. Overdose among heroin users in Sydney, Australia: I. Prevalence and correlates of non-fatal overdose. Addiction 1996;91:405-11
- Bohnert AS, Tracy M, Galea S. Characteristics of drug users who witness many overdoses: implications for overdose prevention. Drug Alcohol Depend 2012;120:168-73
- Wampler DA, Molina DK, McManus J, et al. No deaths associated with patient refusal of transport after naloxone-reversed opioid overdose. Prehosp Emerg Care 2011;15:320-4
- Strang J, Manning V, Mayet S, et al. Overdose training and take-home naloxone for opiate users: prospective cohort study of impact on knowledge and attitudes and subsequent management of overdoses. Addiction 2008;103:1648-57
- Tobin KE, Sherman SG, Beilenson P, et al. Evaluation of the Staying Alive programme: training injection drug users to properly administer naloxone and save lives. Int J Drug Policy 2009;20:131-6
- Teesson M, Mills K, Ross J, et al. The impact of treatment on 3 years' outcome for heroin dependence: findings from the Australian Treatment Outcome Study (ATOS). Addiction 2008;103:80-8
- Zaric GS, Barnett PG, Brandeau ML. HIV transmission and the cost-effectiveness of methadone maintenance. Am J Public Health 2000;90:1100-11
- Vanagas G, Padaiga Z, Bagdonas E. Cost-utility analysis of methadone maintenance treatment in Lithuania. Medicina (Kaunas) 2010;46:286-92
- Koshkina EA. Mortality associated with drug use. Use of Epidemiologic Methods for Drug User Mortality Research. Petrozavodsk, Russia: United Nations Office on Drugs and Crime, 2008
- Goldstein A, Herrera J. Heroin addicts and methadone treatment in Albuquerque: a 22-year follow-up. Drug Alcohol Depend 1995;40:139-50
- Hser YI, Hoffman V, Grella CE, et al. A 33-year follow-up of narcotics addicts. Arch Gen Psychiatry 2001;58:503-8.
- Vlahov D, Wang C, Ompad D, et al. Mortality risk among recent-onset injection drug users in five U.S. cities. Subst Use Misuse 2008;43:413-28