
Abstract
Objective:
To estimate the costs of adverse events (AEs) in patients aged ≥65 years with metastatic renal cell carcinoma (mRCC).
Methods:
Retrospective study using the linked Surveillance, Epidemiology and End Results (SEER) Medicare database. Study subjects consisted of persons in SEER-Medicare, aged ≥65 years, with evidence of newly diagnosed mRCC between January 1, 2007 and December 31, 2007. Adverse events of interest consisted of Grade 3 or 4 toxicities that have been reported with frequency ≥5% in randomized controlled trials of sunitinib, sorafenib, bevacizumab, and pazopanib (i.e., targeted therapies for mRCC), and included abdominal pain, back pain, diarrhea, dyspnea, extremity pain, fatigue/asthenia, hand-foot syndrome, hypertension, lymphopenia, nausea/vomiting, neutropenia, proteinuria, and thrombocytopenia. Patients in SEER-Medicare with these events were identified based on ICD-9-CM diagnosis codes on Medicare claims. For each AE of interest, costs were tallied among evented patients over 30 days, beginning with the date of each patient’s first mention of the AE, and were compared with those of non-evented patients over a similar 30-day period beginning with an identical ‘shadow’ index date. Total costs were compared on an unadjusted basis and with adjustment for differences in baseline characteristics using a generalized linear model.
Results:
A total of 881 patients with mRCC met study entry criteria; 60% of these patients had Medicare claims with mention of one or more AEs of interest. Events occurring with frequency >20% included abdominal pain, dyspnea, and fatigue/asthenia; 10–20% of study subjects had encounters for back pain, extremity pain, and nausea/vomiting. Mean (standard deviation) total cost of care over 30 days was substantially higher among patients with AEs ($13,944 [$14,529]) compared with those without mention of these events ($1878 [$5264]). Adjusting for differences in baseline characteristics, the mean (95% confidence interval) difference in costs between evented and non-evented patients was $12,410 ($9217–$16,522). Study limitations include problems in event ascertainment due to inaccuracies in ICD-9-CM coding on Medicare claims data, and restriction of the study population to patients with metastatic involvement at initial diagnosis of RCC.
Conclusions:
Costs of care are substantially higher in patients aged ≥65 years with mRCC who experience AEs commonly associated with sunitinib, sorafenib, bevacizumab, and pazopanib. Efforts to prevent and/or better manage these events potentially can reduce healthcare costs.
Introduction
Kidney cancer accounts for ∼2% of all incident malignancies worldwideCitation1. In 2012, there were an estimated 64,770 cases of newly diagnosed kidney cancer in the US, and 13,570 deaths due to the diseaseCitation2. Renal cell carcinoma (RCC) accounts for ∼85% of all kidney cancers; the remainder is comprised mainly of carcinoma of the renal pelvis (transitional cell carcinoma)Citation3. Mean age at diagnosis of RCC is 64 years. Since RCC is often asymptomatic in its early stages, there is frequently metastatic involvement at initial diagnosisCitation4,Citation5.
Metastatic RCC (mRCC) is a deadly disease with a very poor prognosis. Historically, 5-year survival has been no more than ∼10%Citation6. Nephrectomy, metastectomy, and cytotoxic chemotherapy have limited or no effectivenessCitation7. Standard first-line therapy for mRCC traditionally has been cytokine therapy (interleukin-2 [IL-2] and/or interferon-α [IFN]); however, it is of limited benefit in selected patients onlyCitation7. Advances in understanding of the biology and genetics of RCC have led to novel targeted approaches to treatment, including: tyrosine kinase inhibitors (e.g., sorafenib, sunitinib, pazopanib, axitinib); the monoclonal antibody (mAb), bevacizumab; and the mammalian target of rapamycin (mTOR) inhibitors, temsirolimus and everolimusCitation8.
While these targeted therapies are more effective than prior treatment and, therefore, have become the standard of care in patients with mRCCCitation3, they are not without their shortcomings. In particular, a number of adverse events (AEs) have been reported in clinical trials of these agents, including fatigue, diarrhea, hypertension, hand-foot syndrome, stomatitis, bleeding, and gastrointestinal perforationCitation9–12. There is limited information on the economic costs associated of these events, especially among patients aged ≥65 years.
Patients and methods
Overview
This study employed a retrospective cohort design to estimate the economic burden of selected AEs in patients aged ≥65 years with newly diagnosed mRCC, based on analyses of the linked Surveillance, Epidemiology and End Results (SEER) Medicare database. Study subjects consisted of all persons in SEER-Medicare, aged ≥65 years, with evidence of newly diagnosed mRCC between January 1, 2007 and December 31, 2007. AEs of interest consisted of Grade 3 or 4 toxicities that have been reported with frequency ≥5% in randomized controlled trials of sunitinib, sorafenib, bevacizumab, and pazopanib (i.e., targeted therapies for mRCC). The economic burden of these AEs was estimated by comparing healthcare costs between patients with and without these events. All analyses were descriptive in nature, as there were no a priori study hypotheses.
Data source
Data for this study were obtained from the linked SEER-Medicare database. SEER is an epidemiologic surveillance system of the National Cancer Institute (NCI) that is comprised of population-based tumor registries; the system is designed to track cancer incidence and survival in the US. The SEER tumor registries routinely collect information from multiple reporting sources, including hospitals, outpatient clinics, laboratories, private medical practitioners, nursing, convalescent homes, hospices, autopsy reports, and death certificates on all persons in geographically defined areas who have newly received diagnoses of cancer. About 28% of the US population is represented in SEERCitation13. By combining information from both SEER and Medicare files, the linked dataset provides information on cancer diagnosis and treatment, as well as downstream medical care. This combined data source offers the opportunity to link service utilization over time to stage at diagnosis as well as time from diagnosis to death. The source population for this study consisted of all persons in the January 2011 release of the SEER-Medicare database who met the selection criteria described below.
Study subjects
We selected all persons in SEER-Medicare, aged ≥65 years, with newly diagnosed mRCC between January 1, 2007 and December 31, 2007, as reported in SEER; the study population, therefore, was limited to patients with metastatic disease at initial clinical presentation, as reflected in cancer staging information in SEER. All study subjects were tracked from their date of diagnosis of mRCC, as reported in SEER (‘index date’), to death, the end of the study period (i.e., December 31, 2009), or date of initial diagnosis of another primary cancer (if applicable), whichever came first. We excluded all persons with gaps in eligibility for Medicare benefits over the 365-day period preceding the index date.
Adverse events
We limited our attention to Grade 3 or 4 toxicities (i.e., moderate or severe in severity) that have been reported with frequency ≥5% in randomized controlled trials of sunitinib, sorafenib, bevacizumab, and pazopanib (i.e., targeted therapies for mRCC), as noted in package labeling information for these agentsCitation9–12, and that could be identified using ICD-9-CM diagnosis codes in healthcare claims data. AEs that met these criteria for one or more targeted therapies for mRCC are listed in . Patients were deemed to have been ‘evented’ if they had any evidence of any of these events during follow-up, based on a scan of all inpatient and outpatient medical claims.
Table 1. Grade 3 or 4 adverse events included in the study*.
Patient characteristics
Patients were characterized in terms of gender, age as of index date, race, US census region, Charlson comorbidity index at index date, total cost during pre-index period, and duration of follow-up.
Outcome measures and analysis
We estimated the number of patients with evidence of each of the AEs of interest following diagnosis of mRCC, based on a scan of all Medicare claims, on an overall basis and by time since index date. Patients were counted once only for each event, and time to first event was measured in relation to the index date.
We examined the impact of AEs on total direct healthcare costs, excluding the costs of targeted therapy from the analyses. Costs were estimated as the sum of Medicare reimbursements and patient co-insurance and liability. Since it is possible for patients to experience more than one AE, and since attribution of care to specific causes can be problematic, we examined each AE separately. In particular, for each AE of interest, we tallied healthcare costs over a period of 30 days following first mention of the event (‘post-event period’), and compared costs over this period between patients with evidence of the event to patients without such evidence; for non-evented patients, costs were tallied over a similar 30-day period, starting on a ‘shadow’ index date that was assigned based on mean time-to-event among evented patients. Time from diagnosis of mRCC to the post-event periods therefore was similar between evented and non-evented patients. A 30-day follow-up was used to tally costs, since most of the AEs of interest are transient and would be expected to resolve within a short time frame.
Non-evented patients who disenrolled prior to the ‘shadow’ index date were excluded from the analyses. Patients who disenrolled during the post-event period were not censored. While it would be possible for both evented and non-evented patients to experience other AEs within the post-event period for any given AE, we assumed that there was no obvious reason for a patient with abdominal pain, for example, to experience other AEs more (or less) frequently than a patient who did not have abdominal pain.
To control for differences in baseline characteristics between patients with and without evidence of AEs, healthcare costs during the 30-day post-event period were analyzed using multivariate generalized linear (GLM) models with a log-link function and gamma response probability distribution. A separate model was estimated for each AE. Independent variables in each model included a binary variable indicating presence/absence of the event in question and the following covariates: gender, age as of index date, race, US census region, Charlson comorbidity index at index date, and total cost during pre-index period. Using the estimated parameter (β) for the binary (i.e., 0/1 dummy) variable for the event in question and mean total costs among patients who did not experience the AE of interest (X), the increase in total costs of medical-care services among patients who experienced the event was estimated as X*[exp(β) − 1].
All analyses were conducted using SAS® Proprietary Software, Release 9.2 (SAS Institute Inc., Cary, NC).
Results
Study sample
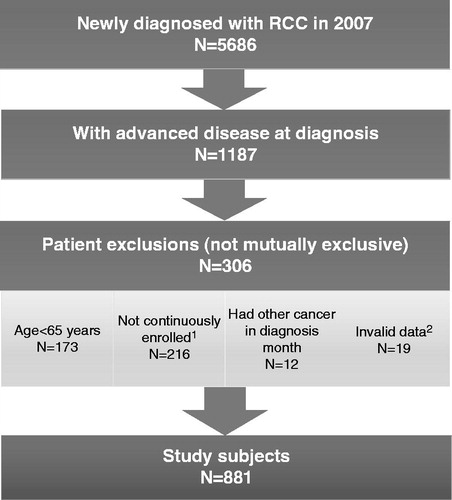
We identified 5686 patients with newly diagnosed RCC in 2007, 1187 of whom had metastatic involvement at diagnosis (i.e., mRCC) (). A total of 306 (26%) patients with mRCC were excluded from the study sample; principal reasons for exclusion (not mutually exclusive) included lack of continuous eligibility for Medicare Part A and B during the 12-month period preceding the index date (18%), and age <65 years at diagnosis (15%). A total of 881 patients met all study entry criteria.
Adverse events
Characteristics of mRCC patients who experienced AEs and the characteristics of those who did not are presented in . A total of 526 (60%) patients had Medicare claims for one or more AEs during follow-up. Baseline characteristics were generally similar between patients with evidence of AEs vs those without evidence of these events. Patients with claims for AEs, however, were less likely to reside in the West (44% vs 62% for those without evidence of AEs), had higher median total healthcare costs during their pre-index period ($4044 vs $1467, respectively), and had a longer mean (SD) duration of follow-up (357 [334] days vs 217 [310] days).
Table 2. Characteristics of patients with metastatic renal cell carcinoma, by evidence of treatment-related adverse events (n = 881).
The numbers of patients who experienced the AEs of interest are reported in , by time since index date. During the first 3 months following diagnosis of mRCC, >20% of patients had one or more Medicare claims for abdominal pain and fatigue/asthenia, and 14% had claims for dyspnea; other frequently observed events included back pain (11%), extremity pain (8%), nausea/vomiting (8%), and diarrhea (3%). During months 4–12 following diagnosis, the same AEs were observed, but at somewhat lower rates.
Table 3. Incidence of selected treatment-related adverse events among patients with metastatic renal cell carcinoma, by time since index date (n = 881)*.
Total medical-care costs during the 30-day post-event period, excluding the cost of targeted therapies, are reported in and . Mean time to event among patients with AEs ranged from 88 days for abdominal pain to 211 days for proteinuria; across all events of interest, it was 65 days (). Mean (SD) cost among patients with evidence of AEs was $13,944 ($14,529); it was $1878 ($5264) among patients without any evidence of AEs (95% CIs were non-overlapping). For all AEs examined, mean total cost was higher among evented patients than those without evidence of the event.
Table 4. Mean total cost of medical-care services (excluding cost of targeted therapies) during 30-day post-event period* among patients with metastatic renal cell carcinoma (n = 881).
Table 5. Estimated increase in mean total cost of medical-care services (excluding cost of targeted therapies) associated with evidence of treatment-related adverse events during 30-day post-event period* in patients with metastatic renal cell carcinoma (estimates adjusted for differences in baseline characteristics) (n = 881).
In the GLM models, costs associated with each AE during the 30-day post-event period were estimated based on the parameter estimate for the binary event flag and mean total cost among patients without evidence of the AE (). The estimated increase (95% CI) in costs during the 30-day post-event period among patients with evidence of any AEs (vs none) was $12,410 (95% CI = $9217–$16,522). For all types of AEs reported, the estimated difference was positive, and the 95% CI did not include zero.
Discussion
Using the linked SEER-Medicare database, we estimated the costs of AEs associated with treatment of mRCC in patients aged 65 years and older, limiting our attention to moderate-to-severe (i.e., Grade 3 or 4) AEs that have been reported with a frequency ≥5% in randomized controlled trials of sunitinib, sorafenib, bevacizumab or pazopanib (as reported in the product label).
More than one-half of the study population (60%) had evidence of one or more AEs associated with targeted therapies for mRCC. The AEs occurring with frequency ≥20% (abdominal pain, dyspnea, and fatigue/asthenia), as well as those occurring less frequently, were transient in nature, suggesting that a 30-day period of follow-up was probably appropriate. Two per cent of study subjects had Medicare claims for proteinuria, and fewer than 1% had claims for hand-foot syndrome, hypertension, lymphopenia, neutropenia, or thrombocytopenia. Although the difference in the duration of follow-up was statistically different between patients with evidence of AEs and those without such evidence (357 days vs 217 days), we believe this did not impart a bias to our estimates, since mean time to AEs (65 days) was well within the mean duration of follow-up among non-evented patients.
Mean (SD) total costs of medical-care services (excluding costs of targeted therapies) during the 30-day post-event period were considerably higher among patients with AEs—$13,944 ($14,529) vs $1878 ($5264) for those without evidence of these events. When adjusted for differences in patient baseline characteristics, the estimated increase in cost (95% CI) was $12,410 ($9217–$16,522). We note that we limited our attention to the direct cost of AEs alone. A comprehensive assessment of the impact of AEs in elderly patients with mRCC also would need to consider effects on health-related quality-of-life.
There are three retrospective studies of AEs in patients with metastatic RCC receiving angiogenesis inhibitorsCitation14–16. Choueiri et al.Citation14 reviewed the medical charts of 144 patients with mRCC at two US oncology centers to assess the costs of AEs experienced by those receiving sunitinib, sorafenib, or bevacizumab. The cost of treatment of AEs was $729 for sunitinib, $636 for sorafenib, and $291 for bevacizumab. Our study did not assess AEs by individual therapy nor the cost of treatment of AEs for each drug. Feinberg et al.Citation15 examined the medical records of 250 patients with mRCC who received sunitinib or sorafenib and reported that the mean duration of therapy with these agents was ∼5–6 months. The overall incidence of AEs (all grades) was 86–87%, and the incidence of Grade 3/4 events was 28–30%. In our study, 60% of study subjects had evidence of Medicare claims for at least one type of adverse event.
Although it is not a retrospective study, Miskisch et al.Citation16 estimated the costs of managing Grade 3/4 toxicities among mRCC patients receiving bevacizumab in combination with interferon-α2a vs sunitinib in four European countries. Using a linear decision analytical model, they reported average AE management costs per patient that ranged from €400–€2600.
Several limitations of our study should be noted. Our study population was limited to patients with mRCC at initial clinical presentation, as evidenced by cancer staging information in SEER. Therefore, patients who did not have metastatic disease at initial clinical presentation but progressed later were not included in our study.
As with all studies based on health insurance claims data, errors of commission and omission are always a concern, especially as they may affect case-finding methods that rely on ICD-9-CM diagnosis codes—in the case of our study, the identification of subjects with AEs of interest. The impact of such errors in coding on our findings is unknown.
Moreover, since unique ICD-9-CM diagnosis codes do not exist for some of the AEs of interest, we do not know the sensitivity and specificity of the methods we employed to identify patients who were evented. Fewer than 1% of patients had Medicare claims for hypertension, while rates reported in package inserts (Grade 3/4 severity) were 13% for sunitinib, 6% for bevacizumab, and for 3% sorafenib. This difference probably reflects errors deriving from the use of ICD-9-CM coding.
Our analyses of costs associated with AEs were limited to the 30-day period following first mention of each event. While we believe this period was sufficiently long to capture most of the important economic consequences associated with these events, we do not know this for certain. To the extent that costs remain elevated beyond 30 days, we may have under-estimated the costs of AEs. We also did not distinguish between the costs of diagnosis and those of treatment, since it is infeasible from a practical standpoint to do so using health insurance claims data.
Finally, we note that our study sample was limited to patients aged 65 years and older. The generalizability of our findings to patients who are younger is unknown.
Conclusion
In our study in a Medicare population, we found that more than one-half of patients with mRCC experienced one or more AEs that have been associated with targeted therapies for this disease, and that the costs associated with these events are substantial. Efforts to prevent and/or better manage these events may potentially reduce the economic burden of treating this disease. Additional research is also needed to substantiate our findings.
Transparency
Declaration of funding
This study was funded by GlaxoSmithKline, Philadelphia, PA.
Declaration of financial/other relationships
MH and GO are employees of Policy Analysis Inc. and have received funding for the research from GlaxoSmithKline. MDH is an employee of GlaxoSmithKline and owns stock options in GlaxoSmithKline.
Acknowledgment
No assistance in the preparation of this article is to be declared.
References
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893–917
- American Cancer Society. Cancer Facts & Figures 2012. Atlanta, GA: American Cancer Society, 2012. http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-031941.pdf. Accessed November, 2012
- SEER Program Public Use Tapes 1973--2002, November 2004 Submission. Bethesda, MD: National Cancer Institute, Division of Cancer Control and Population Science, Surveillance Research Program, Cancer Statistics Branch, 2005
- American Cancer Society. Kidney Cancer (Adult) -- Renal Cell Carcinoma. Atlanta, GA: American Cancer Society, 2013. http://www.cancer.org/acs/groups/cid/documents/webcontent/003052-pdf.pdf. Accessed July, 2013
- Gupta K, Miller JD, Li JZ, et al. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): a literature review. Cancer Treat Rev 2008;34:193–205
- Motzer RJ, Bander NH, Nanus DM. Renal-cell carcinoma. N Engl J Med 1996;335:865–75
- Motzer RJ, Russo P. Systemic therapy for renal cell carcinoma. J Urol 2000;163:408–17
- Chowdhury S, Larkin JM, Gore ME. Recent advances in the treatment of renal cell carcinoma and the role of targeted therapies. Eur J Cancer 2008;44:2152–61
- Highlights of prescribing information: Avastin (bevacizumab), Solution for intravenous infusion. Genentech, Inc., 2011. http://www.gene.com/gene/products/information/pdf/avastin-prescribing.pdf. Accessed April, 2011
- Highlights of prescribing information: Nexavar (sorafenib) tablets, oral. Bayer HealthCare Pharmaceuticals Inc., 2011. http://www.univgraph.com/bayer/inserts/nexavar.pdf. Accessed April, 2011
- Highlights of prescribing information: Sutent (sunitinib malate) capsules, oral. Pfizer Inc., 2010. http://labeling.pfizer.com/ShowLabeling.aspx?id=607. Accessed April, 2011
- Highlights of prescribing information: Votrient (pazopanib) tablets. GlaxoSmithKline, 2009. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022465lbl.pdf. Accessed April, 2011
- National Cancer Institute. SEER Surveillance, Epidemiology, and End Results Program. NIH Publication No. 05-4772. September 2005. http://seer.cancer.gov/about/. Accessed October, 2011
- Choueiri TK, McDermott D, Sheng Duh M, et al. Costs associated with angiogenesis inhibitor therapies for metastatic renal cell carcinoma in clinical practice: results from a medical chart review study. J Urol Oncol 2012;30:848–55
- Feinberg BA, Jolly P, Wang ST, et al. Safety and treatment patterns of angiogenesis inhibitors in patients with metastatic renal cell carcinoma: evidence from US community oncology clinics. Med Oncol 2012;29:786–94
- Mickisch G, Gore M, Escudier B, et al. Costs of managing adverse events in the treatment of first-line metastatic renal cell carcinoma: Bevacizumab in combination with interferon-α2a compared with sunitinib. Br J Cancer 2010;102:80–6