
Abstract
Objectives:
To conduct a cost-minimization analysis of landiolol for CT diagnosis of coronary heart diseases in patients with tachycardia in Japan.
Methods:
A decision-tree model was constructed to analyze costs from the healthcare payer’s perspective. Drug costs and diagnosis costs, computer tomography coronary angiography (CTCA), and coronary angiography (CAG), are adopted to the model. Landiolol is administered only to slow the heart rate to take CT images appropriately. Since some trials proved that there was no difference between landiolol and placebo in terms of efficacy and safety, this study conducted cost-minimization analysis. Of those suspected of coronary heart diseases, 22.5% are thought to be taking beta-blockers. The success rates for CT scanning for landiolol and placebo, derived from domestic trial data, were 81.4% (96/118, 77.8–84.9%) and 54.2% (64/118, 49.7–58.8%). Patients who failed to take a CT image were thought to take CAG. The healthcare cost was derived from a Japanese fee schedule. Costs of landiolol, CT imaging, and CAG are JPY2634 (USD1 = JPY100, as of November 20, 2013), JPY38,116, and JPY101,322, respectively. The positive rate for CAG, derived from domestic trial data, was 37.1% (33/89, 32.0–42.2%). Various sensitivity analyses, both univariate and probabilistic ones, were conducted.
Results:
In the base case analysis, expected costs per patient for landiolol and placebo were JPY78,956 and JPY82,232, respectively. In budget impact analysis, 81,062 patients are eligible for landiolol and it can save JPY266million for whole patients. Sensitivity analyses suggested the robustness of the results.
Limitations:
This study did not consider any adverse effects in the decision-tree model. This model was developed especially for measuring the cost-saving effect of landiolol, through decreasing the number of patients who require CAG, due to imaging failure.
Conclusions:
Landiolol for CTCA diagnosis in patients suspected of coronary heart disease with tachycardia is thought to be cost saving.
Introduction
In 2009, total healthcare expenditure for ischemic heart disease in Japan was JPY777 billion (USD1 = JPY100, as of November 20, 2013), which is 2.14% of overall healthcareCitation1. Ischemic heart disease affects nursing care as well. According to a survey for care-giving conducted in 2007, it is the 6th leading cause of needing nursing care, or 4.3% of all causesCitation1,Citation2.
The age-adjusted mortality rate of ischemic heart disease in Japan is especially low at approximately one fourth of the US or EuropeCitation2, and an increase of the rate is not yet observed. However, there is increasing concern for the rise of heart disease mortality, due to the Westernization of people’s lifestyles. From the economic aspects in both healthcare and nursing-care, in general, we should focus more on primary prevention of heart diseases, rather than on treatment of them. In clinical practice, computed tomography coronary angiography (CTCA) is used for patients suspected of ischemic heart disease with elevated heart rate. The annual number of CTCA performed in Japan was estimated to be 156,336, based on the 2009 Survey of Medical Care Activities in Public Health Insurance by the Ministry of Health, Labor and WelfareCitation3.
The main purpose of CTCA is the diagnosis of coronary stenosis, while there remains the risk of failing to obtain images. In such cases, we are unable to obtain any information from CTCA. Therefore, all patients will undergo coronary angiography (CAG). On the condition that we have appropriate images, we can evaluate coronary stenosis for them and we only have to perform CAG on those who are positive. The critical pathway is illustrated in .
Figure 1. Critical pathway for the diagnosis of coronary stenosis.
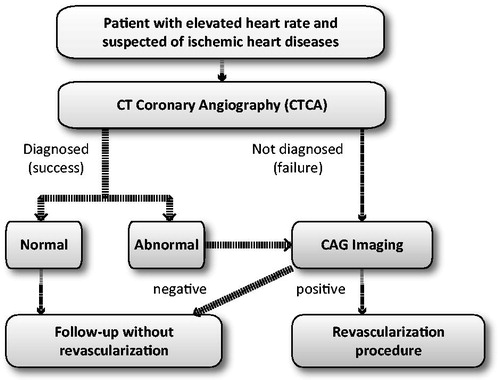
According to Lesser JR et al.Citation4, patients with heart rates above 65 are at risk of imaging failures due to tachycardia and eligible for beta-blocker administration. Landiolol hydrochloride (Corebeta, Onoact), a short-acting beta-blocker, can reduce that risk via its bradicardic effectCitation5,Citation6. It can also save costs of diagnoses, by avoiding unnecessary CAGs due to imaging failures. Moreover, landiolol was thought to be better than other beta-blockers, since its bradicardic effect would shortly be diminished after CTCAs. In addition, it may give some pharmacoeconomic advantages through reducing the number of patients indicated for CAG due to the imaging failure.
In spite of these expected advantages, there is no study from either Japan or other countries that conducts pharmacoeconomic analysis into the administering of beta-blockers to coronary disease patients for the purpose of temporary bradycardia.
The prevalence of those who need revascularization would be unchanged, even with CTCA implementation. CTCA could not reduce prevalence rate, but only decrease numbers of patients requiring CAG imaging, due to imaging failure, and save costs of diagnoses. From this point, our analysis could be regarded as ‘cost-minimization analysis’, in which medical costs differed while the prevalence rate of patients requiring revascularization was the same. We did not assume that introduction of a beta-blocker could reduce the number of patients that were CAG positive, rather the number of patients receiving CAG, through decreasing the probability of imaging failures of CTCA, which would be followed by unnecessary CAG.
Methods
Decision-tree model
A decision-tree model was constructed to analyze costs from a healthcare payer’s perspective. The model was terminated when patients got their final diagnosis for CHD. The model was constructed with special software (TreeAge Pro 2013, Williamstown, MA). While landiolol could contribute to reducing the number of CAG, the proportion of CHD positive patients would be unchanged.
From the healthcare payer’s perspective, medicinal costs and diagnosis costs (CTCA and CAG imaging) are incorporated into the decision-tree model ().
Figure 2. Decision tree model for administering beta-blockers to patients suspected of ischemic heart disease.

Utilization rate of landiolol
According to Lesser JR et al.Citation4 in 2007, among those patients suspected of coronary disease, 22.5% (232/1033, 95% CI = 21.3–23.8%) received an injectable beta-blocker for the purpose of bradycardia. Based on this study report, we assumed that patients with the same background are receiving beta-blockers at the same rate as in Japan. That is, among those who are eligible for CTCA imaging, 22.5% of patients are thought to be probable high-risk groups for imaging failure and administrated with a beta-blocker. Note that beta-blocker introduction can only increase the success rate of CTCA imaging, while it cannot alter the general prevalence rate of CAG-positive patients.
Efficacy of landiolol
As was mentioned in the previous section, landiolol could only contribute to increase the success probability of CTCA imaging itself, while numbers of CAG positive patients were the same. Success rates for CTCA imaging with/without a beta-blocker were derived from a phase III clinical trial conducted in Japan. They were: 81.4% (96/118, 95% CI = 77.8–84.9%) in beta-blocker arm, and 54.2% (64/118, 95% CI = 49.7–58.8%) in the placebo arm. Patients whose heart rate was 70 or more were eligible for that trial. In our model, those whose heart rate was no less than 65, instead of 70, were assessed. Although patients with a lower heart rate, or between 65–70, were more likely to have a higher success rate, we did not modify success rates for clinical trials to make conservative estimation. When the CTCA imaging was not successful, all the patients will be subjected to CAG imaging. The rate of positive results from CTCA imaging, that is those needing CAG imaging for the purpose of making definitive diagnosis, was based on the results from the same data, which was 37.1% (33/89, 95% CI = 32.0–42.2%).
Cost data
We collected drug costs and costs for diagnosis from the healthcare payers’ perspective. Since no other medicines had been approved for the same purpose, we referred to the reimbursement price of Corebeta, JPY2634 as of September 2011, as the cost for landiolol in base case analysis; Corebeta is approved for the improvement of image quality of coronary arteries for CTCA in patients with increased heart rate. The drug is already available and its dose is 0.125 mg/kg/min. Landiolol has also been approved for a different indication, of tachycardia during the intra-operative and post-operative period, with a different reimbursement price, JPY6486 (as of April 2011, Onoact). The price of Onoact was used for the upper limit of medicine prices in the sensitivity analysis.
For the cost of CTCA or CAG imaging, we compiled the medical service fee from the table of medical care service fee points based on the standard therapy. As a result, the cost for CTCA is JPY38,116, and the cost for CAG imaging is JPY101,322 ()Citation7.
Table 1. Cost comparison of Computed Tomography Coronary Angiography (CTCA) and coronary angiography Coronary Angiography (CAG) imaging.
Sensitivity analysis
We conducted one-way sensitivity analyses of efficacy rate, drug cost, and examination cost. Ranges for analyses were obtained from 95% CI for the efficacy rate, and a hypothetical scenario for drug and diagnosis costs, respectively. For the probabilistic sensitivity analysis, we have applied the beta distribution for efficacy parameters.
Results
Base case analysis
The expected per-patient cost for landiolol is JPY78,945 and JPY82,237 for the placebo arm. Thus, landiolol can reduce the cost by JPY3292 per one patient.
According to the survey conducted by the Japanese Circulation Society, 360,275 patients undertook CTCA in 2011.
Out of 360,275 patients, 81,062 (22.5%) patients would be regarded as ‘high-risk’ patients and eligible for landiolol.
Per-patient cost of landiolol was JPY2634. Then, it would cost JPY213million, 2634 times 81,062. However, CAG imaging cost will be reduced to JPY267million, 3292 times 81,062. Overall medical cost saving would be JPY54million, JPY267million minus JPY213million.
In addition, results suggested that the number of patients who require CAG could be reduced to 4943, 81,062 times 0.225 times 0.271.
Sensitivity analysis
Results of one-way sensitivity analyses are summarized as shown in . For all the cases, landiolol administration was the lower cost strategy compared to placebo, of which savings ranged from JPY2638 to JPY3941. The drug cost (JPY6486) and the cost of CTCA imaging (JPY38,116) did not affect the cost difference in two groups, despite being varied based on the scenario; therefore, these results are eliminated from .
Table 2. Results of one-way sensitivity analyses.
We conducted the threshold analysis for the drug cost. As a result, until the drug cost reached JPY17,289, landiolol was cost-saving. In the base-case analysis, the drug cost was set to JPY6486, which was much lower than the threshold.
As a probabilistic sensitivity analysis, we repeated the simulations 10,000 times based on the 95% CI obtained from a clinical trial. As a result, the cost was reduced in the landiolol group in all cases. Therefore, we did not show the acceptability curve.
Discussion
In this study, we performed economic assessments of the drug by administering a beta-blocker for the patients suspected of coronary heart disease when imaging by CTCA. As the representative for beta-blocker, we used landiolol. This selection is based on the clinical trials in Japan conducted by Isobe S et al.Citation5,Citation6 in 2010 that reported that pre-medication using landiolol when imaging by coronary CTCA assures the effect, is practical, and safe. As an analogous drug, no injectable or oral administrable drug other than landiolol is approved for CTCA in Japan as of September 2013.
Currently, the articles on the efficacy of beta-blocker during CTCA imaging can be found globally. As another clinical study aimed at bradycardia while CTCA imaging, De Graaf FR et al.Citation8, in 2010, indicated that a single oral dose of metoprolol, 1 hour prior to the CTCA imaging, is effective in bradycardia. In 2008, Shapiro MD et al.Citation9 showed that a similar effect could be obtained by intravenous injection of metoprolol immediately before CTCA imaging.
However, in Japan, metoprorol is only approved with oral administration. Although metoprolol has similar actions to landiolol, no clinical trial of metoprolol has been conducted in Japan as a pre-medication for CTCA imaging.
A few economic analyses of CTCA itself for chest pain patients have already been reportedCitation10,Citation11. However, economic impacts of beta-blockers with CTCA have never been assessed.
From this research, administering beta-blocker regardless of the case at the time of CTCA imaging for those suspected with coronary heart disease was shown to be cost saving. Due to aging and other reasons, the number of patient with CHD is considered likely to increase. The higher the number of patients, the more CTCA imaging will be needed. Therefore, the budget impact of landiolol implementation will rise in the future.
In this study, we focused only on the reduction of diagnostic cost through the reduced number of CAG as the benefit of increasing the success rate of CTCA imaging. However, in clinical practice, despite the probability of AE with CAG being ∼1/1000Citation12, some patients are scared of the procedure and hesitate to take CAG imaging. This is partly due to the fact that CAG has a certain level of invasiveness. Decreasing the number of CAG tests with a high level of invasiveness with a beta-blocker would lead to an improved patient adherence to treatments. Moreover, by not making any confirmatory diagnosis, we may be able to reduce the number of patients who live with the insecurity of thinking they have suspected ischemic heart disease.
In this analysis, we did not adopt the probabilities of false positive/false negative of CAG and CTCA to our model. In CAG diagnosis, whether or not patients administered landiolol, the probability of misclassification would be the same. In CTCA, since landiolol has a bradycardia effect, those who are landiolol arms are less likely to be false negative. Therefore, removing the false positive/negative arm from our model would be a conservative estimation for landiolol.
In addition, we considered those suspected of having ischemic heart disease were actually healthy, without heart disease. From the aspect of pharmacokinetics, there are reports on a population pharmacokinetics method for healthy adult males when landiolol was administeredCitation13. By conducting clinical studies based on pharmacokinetics, it is considered possible to assess the drug in more detail, paying attention to more specific safety information.
In conclusion, the use of beta-blocker for CTCA coronary angiogram gives assurance to the patients that accident risk from receiving CAG imaging test can be avoided, and in no small part contribute to reduce the increase of medical expenses in the future.
Limitations
This study has limitations. We did not consider any adverse effects in our decision-tree model. This was due to the result of a clinical study in Japan in which no significant difference was found between the beta-blocker arm and placebo arm. In addition, even in the real-world situation after its market approval in September 2011, the prevalence rate of severe adverse effects was fairly low, thus we could say that temporarily we did not need the revision of the model, especially for adverse effects. However, further research will be needed after long-term data become available.
Our model is developed especially for measuring the cost-saving effect of landiolol, through decreasing the number of patients who require CAG, due to imaging failure. That is, neither the cost-effectiveness of CTCA nor CAG itself was evaluated in this model. From a broader scope, further analysis would be required in which overall cost-effectiveness of diagnosis strategies is assessed.
Conclusion
Landiolol for the patients suspected of CTCA diagnosis of cardiovascular diseases (CVD) with tachycardia is considered cost saving.
Transparency
Declaration of funding
The analyses for this manuscript were partly funded by Ono Phamaceutical Co., Ltd. The publication of this result was not contingent on its approval or censorship of this manuscript.
Declaration of financial/other relationships
The authors on this manuscript have disclosed that they received sponsorship from Ono Pharmaceuticals for support in the development of this manuscript.
Notes
*Corebeta and Onoact are landiolol formulations manufactured by Ono Pharmaceuticals, Osaka, Japan.
References
- Kosei-tokei-kyokai. Kokumin eisei no doko 2012/2013, Health and welfare statistics association foundation, Tokyo. 2012, [in Japanese]. (Health and Welfare Statistics Association Foundation: Current Public Health 2012/2013).
- Kosei-tokei-kyokai. Zuhyo kokumin eisei no doko 2010/2011, Health and welfare statistics association foundation, Tokyo. 2011, [in Japanese]. Health and Welfare Statistics Association Foundation: Figures and illustrations of current status of public health 2010/2011.
- Kosei-rodo-syo, Heisei 21 nendo syakai iryo sinryokoibetsu chosa: seifu tokei no sogo madoguchi. Survey of medical care activities in Public Health Insurance: information from government statistics. Ministry of Health, Labor and Welfare, Tokyo. 2011. http://www.e-stat.go.jp/SG1/estat/NewList.do?tid=000001029602. Accessed January 5, 2011. [in Japanese]
- Lesser JR, Flygenring B, Knickelbine T, et al. Clinical utility of coronary CT angiography: coronary stenosis detection and prognosis in ambulatory patients. Catheter Cardiovasc Interv 2007;69:64-72
- Isobe S, Sato K, Sugiura K, et al. Use of landiolol hydrpchloride, a new β-blocker, in coronary computed tomography angiography. Int J Cardiol 2010;132:196-8
- Isobe S, Ando H, Takeuchi T, et al. Landiolol Hydrohloride: a new premedication for multislice computed tomography coronary angiography. Circulation 2010;122:A13659
- Shakai-hoken-kenkyujyo. Ika Shinryo hoshu tensu hyo Heisei-24-nen-4-gatsu-ban. Shakai-hoken-kenkyujyo, Institute of social insurance, Tokyo. 2012 [in Japanese]. Institute of social insurance. National tariff of medical fees 2012. Tokyo, Japan: Institute of Social Insurance, 2012
- De Graaf FR, Schuijf JD, van Velzen JE, et al. Evaluation of contraindications and efficacy of oral beta blockade before computed tomographic coronary angiography. Am J Cardiol 2010;105:767-72
- Shapiro MD, Pena AJ, Nichols JH, et al. Efficacy of pre-scan beta-blockade and impact of heart rate on image quality in patients undergoing coronary multidetector computed tomography angiography. Eur J Radiol 2008;66:37-41
- Ladapo JA, Jaffer FA, Hoffmann U, et al. Clinical outcomes and cost-effectiveness of coronary computed tomography angiography in the evaluation of patients with chest pain. J Am Coll Cardiol 2009;54:2409-22
- Min JK, Gilmore A, Budoff MJ, et al. Cost-effectiveness of coronary CT angiography versus myocardial perfusion SPECT for evaluation of patients with chest pain and no known coronary artery disease. Radiology 2010;254:801-8
- Lavi R, Lavi S, Daghini E, et al. New frontiers in the evaluation of cardiac patients fot noncardiac surgery. Anesthesiology 2007;107:1018-28
- Honda N, Nakade S, Kasai H, et al. Population pharmacokinetics of landiolol hydrochloride in helthy subjects. Drug Metab Pharmacokinet 2008;23:447-55