

Abstract
Objective:
We reported recently that early use of inhaled nitric oxide therapy (iNO) for term and late preterm infants with hypoxic respiratory failure (HRF) at an oxygenation index (OI) of ≥15 and <20 is associated with earlier discharge from the hospital, relative to babies treated at OI ≥25. The objective of the present analysis is to determine whether earlier use of iNO in this cohort leads to lower cost of medical care.
Methods:
We used a decision-analytic model, which was developed to compare hospital resource use and costs associated with early versus standard use of iNO in HRF. The model population included infants with moderate HRF caused by primary pulmonary hypertension with an OI ≥15 and <20. A hypothetical case population of 1000 patients was assumed and probabilistic sensitivity analyses were completed where all the clinical inputs into the model were varied. Two deterministic sensitivity analyses were also completed, one surrounding the hospital cost inputs and another surrounding the cost of iNO.
Results:
Early iNO was associated with fewer hospital days, fewer days of ventilation and fewer hours on extracorporeal membrane oxygenation (ECMO). In probabilistic sensitivity analyses, total costs per patient were $88,518 ± $7574 and $92,581 ± $9664 for early iNO and standard iNO, respectively. The probability of early iNO being cost-effective was approximately 72%, based on a willingness to pay $100,000 or less to prevent ECMO therapy and/or death. In both deterministic sensitivity analyses, early iNO was cost-saving.
Conclusion:
Our analysis shows that early use of iNO at an OI of ≥15 and <20 may be associated with shorter hospitalizations and a decreased cost of care for term/late preterm infants with HRF associated with pulmonary hypertension. Our results are based on clinical data from a single trial; future research using data from real-world practice is warranted.
Keywords::
Introduction
Hypoxic respiratory failure (HRF) in term and late preterm newborn infants is associated with an increased risk of death, need for intensive care support and risk of long-term impairmentsCitation1,Citation2. Inhaled nitric oxide therapy (iNO) decreases the risk of ECMO/death in HRF associated with pulmonary hypertensionCitation2–4. In randomized controlled trials (RCT) that included neonates with severe HRF, iNO was commonly used at an oxygenation index (OI) threshold of ≥25.
The potential benefit of using iNO therapy earlier in the course of HRF was investigated by Konduri et al. in an RCTCitation1. This RCT compared the administration of iNO at an OI of ≥15 and <25 to a control group that received standard iNO therapy if neonates deteriorated to an OI ≥25. The trial showed improvement in oxygenation and decreased rate of progression of HRF when iNO was given at an OI of 15–25; however, the rate of extracorporeal membrane oxygenation therapy (ECMO)/death was not significantly different between early iNO and control groups. The lack of treatment effect may have been a result of little to no separation in severity between early iNO and control groups, as measured by OI at randomization (approximately 20 in both groups).
A recent post-hoc analysis of data from this RCT assessed additional parameters and subgroups. Early iNO was associated with a significantly lower risk of progression of HRF, defined as either progression to OI >30 (P = 0.002) or the composite of OI >30 or ECMO/death (P = 0.02)Citation5. The post-hoc analysis also showed that a subgroup of infants who were enrolled at an OI of ≥15 and <20 (60% of the full population) had a 41% relative reduction in the rate of ECMO/death (10.2% versus 17.4%) with iNO use, although the difference was not significant (P = 0.16). The subgroup that received iNO earlier had a decrease in length of hospital stay, with half of the infants in the early iNO arm enrolled at an OI ≥15 and <20 being discharged after 18 days versus 27 days for control infants treated at higher OI (log rank P = 0.02). Whether the earlier discharge (and presumably lower cost of hospital stay) justifies the added expense of treating larger numbers of infants with earlier iNO application remains unclear. Although potential medical benefits may override the cost considerations in using iNO therapy earlier, it will be useful to estimate whether earlier application of iNO at an OI ≥15 and <20 decreases the cost of care for infants in HRF.
Two previous studies have addressed the cost-effectiveness of iNO therapy for HRF in term and late preterm infantsCitation6,Citation7. Angus et al. used the data from two RCTs that demonstrated the efficacy of iNO in decreasing the ECMO rate and found that use of iNO therapy in these trials was cost-effective, with a decrease in per patient cost of $1880 at the time of publicationCitation6. Armstrong and Dhanda performed a cost-effectiveness analysis on early versus late iNO in an RCT conducted by Gonzalez et al.Citation7 which compared initiation of iNO at OI <30 vs delayed use for infants who deteriorated to OI >40Citation8. This analysis, using a decision-analytic model, found that early iNO was cost-effective and in 87% of scenarios dominated over late iNO by being more effective and less costly. However the RCT by Gonzalez et al.Citation7 was done in a setting where ECMO was not available and used a crossover design for infants failing the assigned treatment group. Treatment failures were treated with a combination of high frequency ventilation and iNO therapy. While a 2003 analysis of iNO found it money saving in selected infants eligible to receive ECMOCitation9, the cost-effectiveness of early iNO therapy in a setting where ECMO is routinely used for HRF resistant to medical management is unknown.
The objective of our present study is to compare the economic implications of initiating early iNO therapy at an OI ≥15 and <20 versus standard therapy at an OI ≥25. Specifically, we developed an economic model based on custom analysis of clinical trial data to evaluate whether the reduction in resource use, as measured by length of stay, compensates for the additional cost associated with earlier initiation of an expensive therapy (iNO).
Methods
Overview
A decision-analytic model was developed to compare the costs associated with early versus standard use of inhaled nitric oxide (iNO) in neonates with hypoxic respiratory failure (HRF). The model population and clinical inputs were based on a single clinical trial first published in 2004, with a focus on the sub-population of infants included in a 2013 post-hoc analysis of the same trial dataCitation1,Citation5. Clinical outcomes included the occurrence of death within 120 days of birth and the use of ECMO therapy. Economic outcomes were evaluated from a hospital cost perspective over the time period from birth through hospital discharge, and included costs of hospital days and costs of therapy (iNO and ECMO, when applicable). The measure of effectiveness was the cost per additional patient alive without ECMO.
Model structure
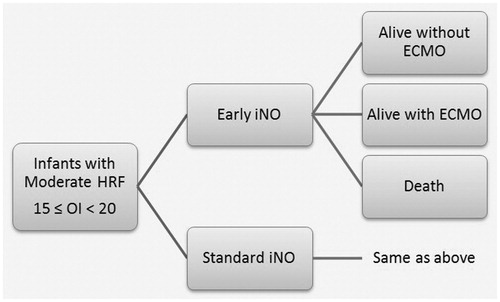
The model population included infants with moderate HRF associated with pulmonary hypertension with a baseline oxygenation index (OI) greater than or equal to 15 and below 20. At randomization, all infants were treated with mechanical ventilation. Infants in the early iNO group were additionally treated with iNO at randomization, while infants in the standard iNO group were only treated with iNO if their OI reached 25 or above. Infants randomized to early INO were started on a 5 parts per million (ppm) dose, which was increased to 20 ppm if the increase in PaO2 from baseline was ≤20 torr, 30 min after the initiation of INO. If the increase in PaO2 at 20 ppm was ≥10 torr, the higher dose was continued, otherwise the dose was decreased back to 5 ppm, which was continued until the infant weaned off, exited to standard INO therapy at 20 ppm for progression of OI or until the infant met the primary outcomeCitation1. The proportion of patients experiencing death (regardless of ECMO use), surviving with receipt of ECMO, and surviving without receipt of ECMO were evaluated for each group, representing the three clinical outcomes of the model. Resource use and costs for each group were evaluated by outcome and then aggregated for each group. The structure of the model is summarized in .
Figure 1. Model structure. ECMO: extracorporeal membrane oxygenation; HRF: hypoxic respiratory failure; iNO: inhaled nitric oxide; OI: oxygenation index.
Model inputs
A hypothetical base case population size of 1000 infants was assumed. All clinical inputs and economic inputs related to resource use were derived through a custom analysis of data from a single trial (Konduri et al.), as summarized in . For resource use inputs among patients who experienced death and patients alive with ECMO, medians over means were used due to small sample sizes (i.e., N < 20) and 10% of the median was assumed for the standard deviation. For resource use inputs among patients alive without ECMO, observed means and standard deviations from the trial were used. Costs of hospital days with and without ventilation as well as costs of ECMO were derived from an analysis of a similar population of neonates, which separated costs between survivors and non-survivorsCitation6. The cost of days without ventilation was assumed to be an average of the estimated cost of ICU days and floor days in the study. All costs were inflated to 2013 US dollars using the medical care component of the US Consumer Price Index. The average hourly cost of iNO (Inomax) was provided by the manufacturer, based on average sales price data. All cost inputs are provided in .
Table 1. Clinical and resource use inputs.
Table 2. Cost inputs.
Sensitivity analyses
Two deterministic sensitivity analyses were completed, including one regarding the hospital cost inputs and another for the cost of iNO. As the original source for hospital costs did not provide standard deviations or confidence intervals surrounding the cost estimates, the mean costs were halved and doubled for lower and upper bounds, respectively. A range of $100 to $130 per hour was used for the cost of iNO, based on expected variations in pricing across hospitals.
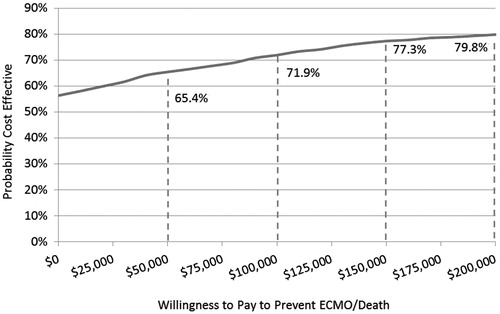
A probabilistic sensitivity analysis (PSA) was also completed where all clinical inputs to the model were varied. Clinical outcomes were varied using a uniform distribution within the 95% confidence interval (CI) surrounding the proportion of patients alive without ECMO, while preserving the ratio of patients experiencing the other two outcomes. The resource use inputs were varied in accordance with a gamma distribution. A Monte Carlo simulation was completed with 1000 simulations. Results were summarized with means, medians, and 95% CIs around total costs and total hospital days per patient as well as with two figures ( and ): (1) an incremental cost-effectiveness scatterplot of the additional patients alive without ECMO versus the difference in total costs; and (2) a cost-effectiveness plane representing the likelihood that iNO would be cost-effective at various thresholds for willingness-to-pay (WTP) to prevent death or ECMO.
Figure 2. Incremental cost-effectiveness scatterplot. ECMO: extracorporeal membrane oxygenation; iNO: inhaled nitric oxide.
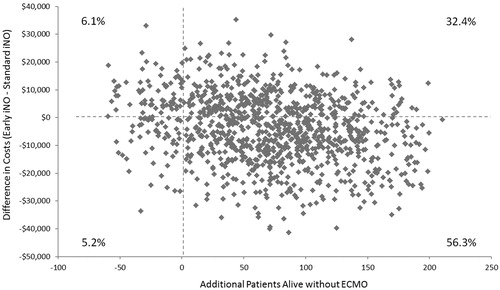
Figure 3. Willingness to pay and cost-effectiveness. ECMO: extracorporeal membrane oxygenation.
Results
Base case analysis
Clinical and economic outputs of the base case model are presented in . A total of 898 patients treated with early iNO would be expected to survive without ECMO, compared with 826 patients treated with standard iNO, due to fewer patients experiencing death (34 vs. 87) and fewer surviving patients requiring ECMO (68 vs. 87). Early iNO would also be associated with fewer hospital days (28.8 vs. 34.6), specifically days without ventilation (17.3 vs. 23.5), and fewer hours on ECMO therapy (15.8 vs. 24.4). Such benefits outweighed the costs of additional hours with iNO therapy (114.1 vs. 60.1). Consequently, early treatment with iNO was associated with net savings of approximately $4000 per infant at a cost of $115 per hour of iNO.
Table 3. Base case model outputs.
Sensitivity analyses
In both deterministic sensitivity analyses, early iNO treatment was cost saving (). For the analysis of hospital costs, the per-infant cost difference ranged from about $2000 to $14,000. The model results were less sensitive to the assumed range for the hourly cost of iNO, with the difference in total per patient costs between treatment groups ranging between $3000 and $5000, in favor of early iNO (). As more infants are treated with iNO in the early iNO group, it follows that lower hospital costs are associated with earlier improvement and hospital discharge of the early iNO group.
Figure 4. Cost savings. iNO: inhaled nitric oxide.
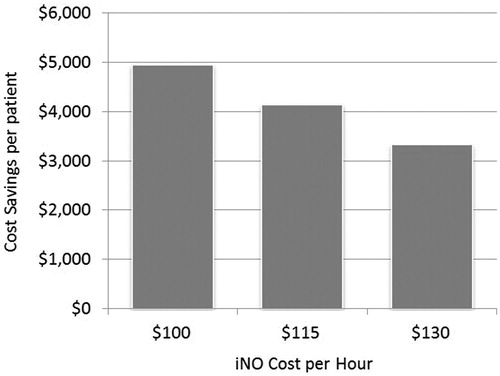
Table 4. Deterministic sensitivity analysis results.
Within the PSA, the mean number of patients alive without ECMO was 898 with early iNO and 827 with standard iNO (). Corresponding mean (SD) costs for the two groups were $88,518 ($7574) and $92,581 ($9664). presents an incremental cost-effectiveness scatterplot obtained from the PSA, reflecting the difference in costs associated with gains in patients alive without ECMO. Early iNO dominated standard iNO in 56.3% of simulations (more effective and less costly), and was dominated by standard iNO in only 6.1% of simulations (less effective and more costly). Early iNO was more effective and more costly in 32.4% of simulations, and less effective and less costly in 5.2% of simulations. With regards to willingness to pay to avoid ECMO/death, the probability of early iNO being cost-effective was 71.9% at $100,000 and 79.8% at $200,000 ().
Table 5. Probabilistic sensitivity analysis results.
Discussion
Our findings suggest that iNO initiated at earlier OI levels (OI ≥ 15 and <20) may be associated with hospital cost savings and likely represents a cost-effective use of healthcare resources compared with standard use of iNO (≥25) in the studied population. Thus, clinicians can use iNO earlier in HRF associated with pulmonary hypertension when indicated with less concern about the escalation in the costs of care from potential increase in the use of iNO therapy for this disease.
We used two types of sensitivity analyses to assess the impact of uncertainty in economic models. They involve varying key model parameters and observing the effect on model results. Parameters can be varied one at a time while holding others constant, as in our deterministic sensitivity analysis, or multiple parameters can be varied simultaneously, as in our probabilistic sensitivity analysis. Sensitivity analyses help to explore potential limitations or uncertainty surrounding the data used for inputs. Using both sensitivity analyses, we found that iNO therapy can be cost saving with early use, as defined by OI of ≥15 and <20.
Several previous studies have evaluated the cost-effectiveness of using iNO (at varying OI thresholds) versus standard treatment. The study by Angus et al. found that there was a 60% probability that iNO was dominant (cost saving and better outcomes), and an 85% probability that iNO had a cost of less than $100,000 per quality-adjusted life-year (QALY), a level that represents good value for moneyCitation6. Similarly, Lorch et al. also assessed the cost-effectiveness of iNO versus standard therapy in treating persistent pulmonary hypertension of the newbornCitation10. They estimated a cost per QALY of around $33,000 suggesting that iNO use is cost-effective, with a similar probability that iNO has a cost per QALY under $100,000 (81%) as the Angus study. More recently, Armstrong and Dhanda evaluated the cost-effectiveness of delayed (OI ≥ 40) versus early use (OI 10 to 30) of iNOCitation7. They found a high (89%) probability that early use of iNO would be cost-saving. Our study is not directly comparable to the others in that it evaluated early use of iNO at a different threshold from prior evaluations (iNO administered with OI 15 to 20 vs. OI ≥ 25). Nevertheless, despite the prolonged duration of iNO use based on the lower OI threshold used in our analysis, we found a 56.3% probability that early iNO would be cost-saving, and a 71.9% probability that it would be cost-effective at a threshold of $100,000 per death/ECMO case averted.
This study is subject to a number of limitations. The majority of data inputs are from a post-hoc analysis of data from a single trial and results for the difference in rates of ECMO/death between the early and standard iNO groups were not statistically significant. While results pertaining to differences in hospital days and hours receiving ECMO therapy were based directly on trial data, the inputs used were not subjected to statistical analysis and, in some cases, were based on small sample sizes (i.e., N < 20). Moreover, while the hospital cost data are from a similar patient population to that included in this analysisCitation6, the estimates are dated. Our results are also based on a single study that recruited patients between 1998 and 2001. It is possible that the morbidities and length of hospital stay may have changed in the current era. However, data from more recent population based studies indicate that the prevalence of persistent pulmonary hypertension of the newborn (PPHN) remains consistent between 1.23/1000 and 2.7/1000Citation11,Citation12. Recent long term follow-up studies also show that 22% to 26% of survivors of PPHN show impairments at 2 years of age or school ageCitation13,Citation14. These data suggest that HRF continues to be a significant clinical problem in the current era. Additionally, our data are based on the experience of neonatal intensive care units (NICUs) in North America and findings may not be generalizable outside of this region. Finally, the time horizon is limited to hospital admission-to-discharge. Longer term outcomes could not be assessed given available data, and thus, QALYs were not captured in our study.
Despite these limitations, our study suggests that earlier use of iNO (at an OI 15 to 20) may be cost-effective in neonates suffering from HRF associated with pulmonary hypertension. Further research using more recent cost data and clinical data from real-world practice is warranted.
Transparency
Declaration of funding
This study was sponsored by Ikaria Inc.
Declaration of financial/other relationships
M.F. and J.M. have disclosed that they are employees of Boston Health Economics Inc., who were paid consultants to Ikaria Inc. in connection with the study and development of this research article. J.P. has disclosed that he is an employee of and owns stock in the sponsor, Ikaria Inc. G.G.K. has disclosed that he was also a paid consultant to Ikaria Inc. in connection with the study and development of this research article. He received an unrestricted grant (awarded to Medical College of Wisconsin) from Ikaria Inc. for supplemental data analysis of the trial supporting this research article; he also received consulting fees from Actelion Pharmaceuticals Ltd, Switzerland, for serving on the Data Safety Monitoring Board of a randomized clinical trial of bosentan in treating persistent pulmonary hypertension of the newborn (a condition related to that reported in this article). T.L. and J.S. have no financial/other relationships to disclose.
JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Acknowledgments
The authors gratefully acknowledge Dr. John Zupancic of Harvard Medical School/Beth Israel Deaconess Medical Center, Boston, MA, USA for his assistance in model design.
References
- Konduri GG, Solimano A, Sokol GM, et al. A randomized trial of early versus standard inhaled nitric oxide therapy in term and near-term newborn infants with hypoxic respiratory failure. Pediatrics 2004;113(3 Pt 1):559-64
- Neonatal Inhaled Nitric Oxide Study Group. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure. N Engl J Med 1997;336:597-604
- Clark RH, Kueser TJ, Walker MW, et al. Low-dose nitric oxide therapy for persistent pulmonary hypertension of the newborn. Clinical Inhaled Nitric Oxide Research Group. N Engl J Med 2000;342:469-74
- Roberts JD Jr, Fineman JR, Morin FC III, et al. Inhaled nitric oxide and persistent pulmonary hypertension of the newborn. The Inhaled Nitric Oxide Study Group. N Engl J Med 1997;336:605-10
- Konduri GG, Sokol GM, Van Meurs KP, et al. Impact of early surfactant and inhaled nitric oxide therapies on outcomes in term/late preterm neonates with moderate hypoxic respiratory failure. J Perinatol 2013;33:944-9
- Angus DC, Clermont G, Watson RS, et al. Cost-effectiveness of inhaled nitric oxide in the treatment of neonatal respiratory failure in the United States. Pediatrics 2003;112(6 Pt 1):1351-60
- González A, Fabres J, D'apremont I, et al. Randomized controlled trial of early compared with delayed use of inhaled nitric oxide in newborns with a moderate respiratory failure and pulmonary hypertension. J Perinatol 2010;30:420-4
- Armstrong EP, Dhanda R. Cost-effectiveness of early compared to late inhaled nitric oxide therapy in near-term infants. Curr Med Res Opin 2010;26:2795-800
- Truog WE, Castor CA, Sheffield MJ. Neonatal nitric oxide use: predictors of response and financial implications. J Perinatol 2003;23:128-32
- Lorch SA, Cnaan A, Barnhart K. Cost-effectiveness of inhaled nitric oxide for the management of persistent pulmonary hypertension of the newborn. Pediatrics 2004;114:417-26
- Kieler H, Artama M, Engeland A, et al. Selective serotonin reuptake inhibitors during pregnancy and risk of persistent pulmonary hypertension in the newborn: population based cohort study from the five Nordic countries. BMJ 2012;344:d8012
- Andrade SE, McPhillips H, Loren D, et al. Antidepressant medication use and risk of persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf 2009;18:246-52
- Konduri GG, Vohr B, Robertson C, et al. Early inhaled nitric oxide therapy for term and near-term newborn infants with hypoxic respiratory failure: neurodevelopmental follow-up. J Pediatr 2007;150:235-40,240
- Berti A, Janes A, Furlan R, Macagno F. High prevalence of minor neurologic deficits in a long-term neurodevelopmental follow-up of children with severe persistent pulmonary hypertension of the newborn: a cohort study. Ital J Pediatr 2010;36:45