

Abstract
Background and aims:
While short-term kidney graft survival has gradually improved over time, improvements in long-term graft survival have been more modest. One key clinical factor limiting improved longer-term outcomes is antibody-mediated rejection (AbMR), the incidence of which appears to be higher in patients who are non-adherent to immunosuppressants. Recent data show that adherence can be improved by reducing pill burden. The aim of the present study was to model the incidence and economic consequences of graft loss and AbMR in patients taking once- vs twice-daily tacrolimus in the UK.
Methods:
A combined decision tree and Markov model was developed to estimate the incidence of graft failure, AbMR and mortality in renal transplant recipients taking once- vs twice-daily tacrolimus. Underlying rates of graft failure and mortality were derived from UK-specific sources. Proportions of patients adherent to once- vs twice-daily tacrolimus were taken from a recent randomized clinical trial and relative risks of graft failure and AbMR were taken from a prospective, multi-center analysis of 315 patients. Cost data were taken from the British National Formulary and National Health Service reference costs and reported in 2014 pounds sterling.
Results:
Modeling results showed that improved adherence would be associated with reduced incidence of AbMR and graft failure in renal transplant recipients. Based on improvements in adherence resulting from switching from twice-daily to once-daily tacrolimus, the modeling analysis projected cost savings of GBP 4862 per patient over 5 years with Advagraf relative to Prograf, on absolute costs of GBP 40,974 and GBP 45,836, respectively.
Conclusions:
Using Advagraf in place of Prograf in renal transplant recipients was predicted to be associated with lower pharmacy, dialysis and AbMR treatment costs, with the reduction in AbMR and dialysis costs being driven by improved adherence to the Advagraf regimen and consequent reductions in graft failure and onset of AbMR.
Background and aims
Graft survival after renal transplantation has improved substantially over the past few decades. In 2000, Hariharan et al.Citation1 reported that both short- and long-term graft survival were improving in the US, suggesting that targeting improvements in short-term outcomes would result in consequent improvements in long-term outcomes and that acute rejection and short-term graft survival were, therefore, useful surrogate end-points for longer-term outcomesCitation2. However, subsequent studies have shown that long-term survival rates were not improving at the same rate as short-term survival, and, more recently, it has become apparent that short-term and long-term graft attrition are driven by distinct processes, with little correlation between the twoCitation3–5.
Key among the processes driving long-term graft failure is antibody-mediated rejection (AbMR). The exact molecular processes underpinning AbMR are still the subject of investigation, but recent studies have shown that donor-specific antibody (DSA) formation is effected by B-cell and plasma cell activation, with DSAs subsequently binding to human leukocyte antigen (HLA) or non-HLA molecules on the graft endothelium, leading to the recruitment of natural killer (NK) cells, polymorphonuclear neutrophils, and macrophages, which bring about capillaritis and tissue injury in the graftCitation6. The endothelial damage then causes platelet aggregation, accumulation of neutrophils, and thrombotic microangiopathy, which ultimately result in cellular necrosis and a rapid decline in graft functionCitation6. AbMR can be divided into two classifications, chronic and acute, the latter of which is further divided into two distinct phenotypes. The 2011 Banff meeting report emphasized the importance of correctly defining the two principal acute AbMR phenotypes: AbMR phenotype 1 in pre-sensitized patients, occurring soon after transplantation; and AbMR phenotype 2, which develops from the emergence of de novo DSA in the late post-transplant periodCitation7.
The second AbMR phenotype identified in the 2011 Banff meeting is thought to arise in patients who are non-adherent or otherwise inadequately immunosuppressedCitation6. For instance, in a review of outcomes in renal transplantation, Halloran et al.Citation8 estimated that 20% of all late graft failures were driven by non-adherence to the prescribed regimen, with the failures caused predominantly by AbMR. Similarly, a 2012 study by Sellarés et al.Citation9 suggested that the incidence of AbMR mediated by de novo DSA is much higher in patients who are non-adherent to their immunosuppressive regimens. Specifically, Sellarés et al. reported that, of 26 patients in whom concerns around adherence were raised, 19 (73%) subsequently experienced graft failure, compared with 41 graft failures (14%) in 289 adherent patients.
The role of non-adherence in driving AbMR is particularly relevant in renal transplant recipients, in whom non-adherence to immunosuppressive regimens is higher than recipients of other solid organ transplantsCitation10. Numerous studies have investigated the factors influencing adherence in transplant recipients, including a 2012 study which reported a strong inverse association between the number of immunosuppressive medications used by a transplant recipient and the proportion of patients who are adherent to therapyCitation11. Furthermore, increased dosing frequency and regimen complexity have also been associated with reduced adherenceCitation12. Given that twice-daily, immediate-release formulations still constitute the majority of UK tacrolimus prescriptions (typically as part of a more complex regimen including steroids and mycophenolate mofetil), there is still a great unmet need in allograft recipients for reduced pill burdenCitation13.
While not all episodes of AbMR result in poor outcomes, patients with acute AbMR are exposed to a higher risk of subsequent rejection, chronic AbMR, or graft failureCitation6. Indeed, graft loss outcomes are significantly worse in patients with AbMR than those with cellular rejectionCitation14. Not only is the longer-term prognosis of patients with AbMR worse, but the initial treatment of AbMR also leads to greatly increased healthcare resource use and cost. The choice of AbMR treatment is complicated by the wide array of available treatment options, around which there is still little consensusCitation15. The lack of consensus is driven in part by the fact that, in contrast to cell-mediated rejection, the US Food and Drug Administration does not yet recognize AbMR as an approvable indicationCitation15. Similarly, the European Medicines Agency (EMA) does not recognize antibody-mediated rejection as a specific indication. The EMA Committee for Orphan Medicinal Products (COMP), under whose remit the prophylaxis and treatment of graft rejection falls, recently convened to discuss the use of eculizumab for prevention of AbMR after solid organ transplantation, but fell short of recognizing AbMR as distinct from other graft rejection mechanisms, instead describing the indication simply as ‘prevention of graft rejection following solid organ transplantation’ (p. 10)Citation16. This has had a material effect on the treatments available for AbMR, presenting a practical barrier to using new medications and leading to a relatively small evidence base. Current AbMR treatment options include therapies targeting DSA, the complement system, antigen-presenting, B, T, and plasma cells, in addition to splenectomy as a last resort to deplete the B-cell and plasma cell poolsCitation15.
Using recent data on the proportion of patients adherent to once- vs twice-daily tacrolimus regimens (Advagraf and Prograf, respectively)Citation17, the relative risks of graft failure and AbMR in non-adherent vs adherent patientsCitation9, and AbMR treatment protocols as described in recent guidelines, retrospective studies, randomized clinical trials and single-center UK treatment regimens, the aims of the present study were two-fold: to evaluate the budget impact of using Advagraf in place of Prograf (thereby reducing the pill burden) in renal transplant recipients in the UK setting, and to evaluate the costs associated with different AbMR treatment modalities.
Methods
A budget impact model was developed in Microsoft Excel (Microsoft Corporation, Redmond, WA) to evaluate the costs associated with immunosuppressive medications, antibody-mediated rejection (AbMR), and graft failure in patients using Prograf or Advagraf as their primary immunosuppressive medication. The model was structured as a decision tree followed by a four-state Markov process (). The decision tree portion of the model divided patients into adherent and non-adherent, based on data from the Adherence Measurement in Stable Renal Transplant Patients Following Conversion from Prograf to Advagraf (ADMIRAD) study published by Kuypers et al.Citation17, which reported the findings of a randomized clinical trial investigating adherence in renal transplant recipients on once- vs twice-daily tacrolimus conducted in Belgium in 2008–2009. In the Prograf arm, 78.8% of patients were adherent to the prescribed tacrolimus regimen, compared with 88.2% of patients in the Advagraf arm (p = 0.0009).
Figure 1. Decision tree, Markov states and possible transitions.
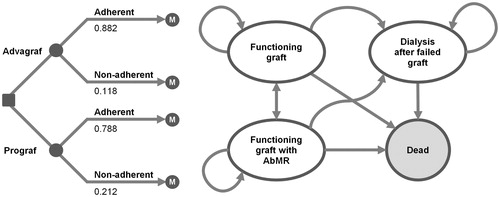
In the subsequent Markov process, transition probabilities modeling the underlying incidence of graft failure and patient mortality were derived from data from the 2013–2014 National Health Service Blood and Transplant (NHSBT) Organ Donation and Transplantation Activity Report (Appendices 1–4). Specifically, data from 2148 UK patients who underwent first kidney transplantation (from donors after brain death) in 2006–2008 were used to establish the ‘baseline’ proportion of grafts and patients surviving at years 1, 2, and 5 after transplant. The probability of transition to death was handled separately from transitions between living states owing to its dependence on time since graft (Appendix 5). Specifically, transitions to the dead state were captured in each cycle prior to transitioning patients between living states, and the probabilities were converted from monthly rates derived from the NHSBT Kaplan-Meier curves. As the model was developed in Microsoft Excel (rather than dedicated Markov modeling software), checksums were used to ensure that all outbound transition probabilities summed to 1 and the model was internally validated against the mortality data on which it was based (i.e., first-order validation). Furthermore, the Markov model was independently implemented using the ‘expm’ matrix exponential package in R, and state distributions were compared over timeCitation18,Citation19.
A relative risk of graft failure in patients not adherent to their prescribed immunosuppressive regimen (relative to those adherent to the prescribed regimen) was derived from the 2011 study by Sellarés et al.Citation9. Specifically, 19 of 26 patients in whom concerns around non-adherence were raised by investigators (or who reported non-adherence directly) experienced graft failure over the median follow-up time of 31.4 months, compared to 41 graft failures in 289 adherent patients, giving a relative risk of 5.15 assuming equivalent mean time at risk for patients in each group. DSA formation occurred in 20 of the 26 non-adherent patients, compared with 84 of the 289 patients with no recorded concerns regarding adherenceCitation9. These data were used to model the probability of onset of AbMR in the adherent and non-adherent patient groups. In the base case analysis, resource use associated with the treatment of AbMR was estimated based on guidelines from the Edinburgh Renal Unit ()Citation20. Specifically, the base case analysis assumed 500 mg of intravenous methylprednisolone given every day for 3 days, five plasma exchanges, and five intravenous immunoglobulin infusions per plasma exchange, for a total of 25 infusions at a dose of 100 mg/kg. Additional DSA monitoring and renal biopsy costs associated with diagnosis were conservatively excluded from the analysis on the grounds that the incremental effects of diagnostic costs would likely be negligible and the sensitivity and specificity of the full AbMR diagnostic protocol is not well characterized. All pharmacy costs were taken from the British National Formulary (BNF) 68th edition, while costs associated with peritoneal and hemodialysis were taken from 2013–2014 National Health Service reference costs ()Citation21. Assumptions around dialysis were informed by an NHS fact sheet on the cost-effectiveness of transplantation and Renal Association guidelines on hemodialysisCitation22,Citation23. Specifically, in patients undergoing dialysis, 24% were assumed to be undergoing peritoneal dialysis, with the remaining 76% of patients attending hemodialysis 3 times weekly.
Table 1. Resource use associated with AbMR.
Table 2. Costs used in the base case analysis.
Cohort
The cohort was assumed to have a mean body weight of 70.3 kg, based on a multi-center randomized trial of Advagraf and Prograf in 667 de novo renal transplant recipients published in 2010 by Krämer; et al.Citation24. The model used mean body weight to calculate the mean daily dose of tacrolimus and the concomitant medications mycophenolate mofetil (MMF) and corticosteroids (prednisolone) based on data from the Krämer et al. study. Tacrolimus doses in the Advagraf and Prograf arms were based on the dose at study day 365 (0.075 mg/kg/day) and were taken to be equivalent, since patients in the Krämer et al. study were initiated on the same dose (of 0.2 mg/kg/day) and subsequent differences (arising from titration to a pre-specified serum trough concentration) were not reported as significant. In the base case, mean MMF doses were taken to be 1450 mg/day in year 1 (based on the mean of the doses at baseline and day 365) and 960 mg/day in subsequent years (based on the dose at day 365 in the Krämer et al. study). All patients were assumed to continue taking MMF for the duration of the modeling analysis. Corticosteroid doses were calculated on the same basis as MMF, and were 16.6 mg/day in year 1 and 4.9 mg/day in subsequent years. However, in contrast to MMF, the proportion of patients taking corticosteroids was taken to be 94.7% in the first year, dropping to 89.3% in subsequent years, also based on the Krämer et al. study.
Time horizon, perspective, and discounting
The base case analysis was run over a 5-year time horizon from the perspective of a UK healthcare payer and the model adopted a monthly cycle length. Future costs were not discounted, in line with International Society for Pharmacoeconomic and Outcomes Research (ISPOR) guidelines for budget impact analysesCitation25.
Sensitivity analyses
A series of sensitivity analyses were performed around the base case to establish the magnitude of effect of various drivers on the absolute and incremental outcomes. Two sensitivity analyses were conducted in which the discount rate was set to 3.5%, in line with the recommendations for discounting the cost component of cost-effectiveness analyses laid out in the National Institute for Health and Care Excellence (NICE) Guide to the Methods of Technology AppraisalCitation26.
Four analyses were performed around the relative risk of graft failure in non-adherent patients compared with adherent patients. Two of the relative risk analyses were based on data from a 2009 study by Pinsky et al.Citation27, in which the relative risks of graft failure were taken from patients categorized as having ‘fair’ and ‘poor’ adherence (based on their adherence quartile within the whole study population), with relative risks of 1.63 and 1.8 compared with the ‘excellent’ group, respectively. The final sensitivity analysis was based on a 2004 meta-analysis by Butler et al.Citation28, in which the graft failure odds ratio of 7.1 in non-adherent relative to adherent patients was converted to a relative risk of 3.47 using the Zhang and YuCitation29 method (based on underlying graft failure rates of 1.3–40% in adherent patients vs 6.1–100% in non-adherent patients).
A series of analyses were conducted around the AbMR treatment modality employed. Additional treatment modalities were investigated based on recent retrospective analyses and case reports of rituximab, bortezomib and eculizumab ()Citation30–32. While there is little consensus around the optimal administration timing and frequency of each AbMR treatment option, the regimens investigated in sensitivity analyses represent relatively conservative use of the respective treatments, namely rituximab infusions, four doses of bortezomib at 1.3 mg/m2, or two 600 mg doses of eculizmabCitation28–30.
Finally, a sensitivity analysis was conducted in which the risk of mortality was increased in patients on dialysis relative to those with a functioning graft. A mortality rate ratio was derived from a 1999 study by Wolfe et al.Citation33 in which patients with a cadaveric renal transplant died at a rate of 3.8 patients/100 patient-years, while patients on dialysis on the transplant waiting list died at a rate of 6.3 patients/100 patient-years.
Results
The base case analysis showed that, over 5 years, patients using Prograf as their primary immunosuppressive medication incurred costs of GBP 45,836, compared with costs of GBP 40,974 in patients with Advagraf, representing a 5-year cost saving of GBP 4862 per patient (, and ). Cost savings were driven by the increased cost of dialysis and AbMR treatment in the Prograf arm, arising from the higher proportion of patients not adherent to the primary immunosuppressive regimen and the associated higher incidence of graft failure (). These cost savings would translate to absolute savings of GBP 486,200 over 5 years in a hypothetical 100-patient cohort.
Figure 2. Projected state distribution in adherent vs non-adherent patients over time.
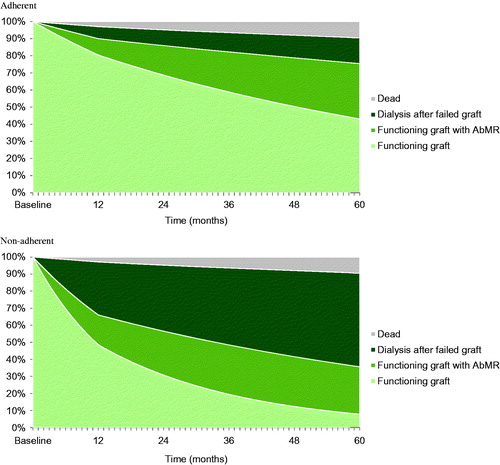
Figure 3. Cumulative per-patient costs with Advagraf vs Prograf over 5 years.
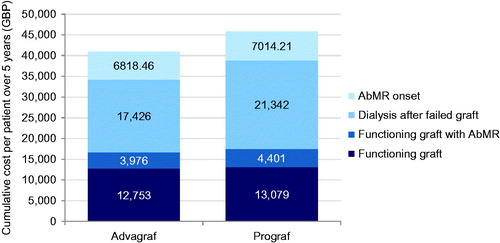
Table 3. Base case results expressed as mean per-patient state and transition costs over a 5-year time horizon.
Table 4. Base case results expressed as mean per-patient drug, antibody-mediated rejection and dialysis costs over a 5-year time horizon.
Sensitivity analysis showed that incidence of AbMR had a large effect on the absolute cost outcomes (). When AbMR costs were removed from the analysis, projected costs dropped by GBP 6818 in the Advagraf arm and GBP 7014 in the Prograf arm. However, the effect on incremental outcomes was smaller, with removal of AbMR costs reducing the incremental costs to a saving of GBP 4666 with Advagraf relative to Prograf. With the exception of eculizumab, choice of AbMR therapy had a relatively small effect on absolute costs. Adding 3.61 rituximab infusions (at 375 mg/m2) to the base case AbMR treatment assumptions increased costs from GBP 40,974 in the Advagraf arm in the base case to GBP 42,528 (an increase of GBP 1554 per patient over 5 years relative to the base case). Switching rituximab for four 1.3 mg/m2 doses of bortezomib increased costs to GBP 41,719, corresponding to an increase of GBP 745 per patient (across all patients) over 5 years. Eculizumab had a much greater effect on costs, increasing costs in the Advagraf arm to GBP 45,763, an increase of GBP 4789 over the base case analysis. Finally, the inclusion of increased mortality rates from the dialysis state had a relatively small impact on costs, reducing overall per-patient costs by GBP 461 and GBP 570 in the Advagraf and Prograf arms, respectively, thereby reducing the cost savings from the base case analysis by GBP 110.
Table 5. One-way sensitivity analysis results.
Discussion
The modeling analysis showed that, when compared with a twice-daily tacrolimus regimen, using a once-daily tacrolimus regimen would result in cost savings in renal transplant recipients in the UK setting over a 5-year time horizon. Cost savings were projected to be driven by reduced pharmacy costs. The strengths of the analysis are the transparent modeling approach, use of recent UK-specific data on underlying graft rejection and mortality rates, and the use of up-to-date UK cost data and resource-use assumptions around AbMR treatment. However, as with all health economic modeling analyses, there are a number of limitations that should be considered when interpreting the results. The analysis made use of data from heterogeneous populations, including data from the NHSBT for the underlying rate of graft failure and patient mortality, data from the ADMIRAD study for the proportion of patients adherent to once-daily vs twice-daily tacrolimus formulations, and data from Sellarés et al.Citation9 for the relative risk of graft failure and AbMR in non-adherent patients relative to adherent patients. For instance, the Sellarés et al. data are derived from patients between 6 days and 32 years after transplantation, with a wide range of etiologies, while randomization in the ADMIRAD study took place on average 3 years after the last renal transplantation (11% of patients had received a second kidney transplant at baseline).
In the ADMIRAD study, which informed the decision tree portion of the model dividing patients into adherent and non-adherent, 219 patients who had previously been on a twice-daily tacrolimus regimen for at least 3 months were randomly assigned to either once-daily or twice-daily tacrolimus and followed using an electronic drug monitor for 6 months. The estimated proportion of patients implementing the respective regimens was 88.2% with once-daily vs 78.8% with twice-daily tacrolimus (p = 0.0009). We consider the ADMIRAD study to represent the most robust available source of evidence regarding adherence to post-transplant immunosuppression in renal transplant recipients, but non-randomized, observational data that corroborate the findings have been published since the ADMIRAD study concludedCitation34. Adherence studies in recipients of other solid organs also support the finding of improved adherence with reduced pill burden. For instance, Eberlin et al.Citation35 reported the findings of a 12-month study of 63 liver transplant recipients converted from twice-daily to once-daily tacrolimus after 6 months. At the end of the conversion period, 3% of patients were classified as non-compliant, compared with 10% immediately prior to conversion (p = 0.008). Similarly, Beckebaum et al.Citation36 published the findings of a conversion study in 125 stable liver transplant recipients in which patients were converted from twice-daily to once-daily tacrolimus. Adherence was assessed using the Basel Assessment of Adherence to Immunosuppressive Medication (BAASIS) scale at 12 months, at which point overall non-adherence had decreased significantly from 66.4% at baseline to 30.9% (p < 0.0001).
A key focus of the sensitivity analyses was around the costs associated with treatment of AbMR. A broad array of treatment modalities have been used for AbMR targeting B, T, and plasma cells, and the complement systemCitation37. The Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group clinical practice guidelines suggest treating acute AbMR with one or more of plasma exchange, IVIG, anti-CD20 antibody, or lymphocyte-depleting antibody, with or without corticosteroidsCitation38. However, the KDIGO group noted that the suggestion is based on a low quality of evidence, and should not be enacted in policy without debate and stakeholder involvement. The base case analysis in the present study used treatment assumptions based on the Edinburgh Renal Unit, which recommends plasmapheresis, intravenous immunoglobulin, and corticosteroidsCitation18. However, sensitivity analyses showed that the addition of rituximab or bortezomib to the base case treatment assumptions had a relatively small effect on the absolute projected cost per patient over 5 years.
One final potential shortcoming of the present analysis centers around the range of clinical outcomes and resource use captured. For instance, Pinsky et al.Citation27 reported significant variations in the incidence of mortality up to 3 years after transplant across patients divided into quartiles by first-year adherence to their immunosuppressive regimen. Patient mortality in the ‘excellent’ adherence group was 3.0% compared with 5.4% in the ‘fair’ compliance group (p < 0.0001). In the base case, the present analysis assumed no difference in mortality either between Prograf and Advagraf (in line with the findings of the Kraümer et al.Citation24 study on which the dosing assumptions were based) or between adherent and non-adherent patients. Budget impact analyses are not well-suited to demonstrating differences in terms of life expectancy, and any such differences would be better evaluated in a cost-effectiveness analysis, in which incremental costs are balanced with incremental effectiveness outcomes (such as life expectancy). Nevertheless, a single sensitivity analysis was conducted in which patients in the dialysis state were at increased risk of mortality relative to patients with a functioning graft. The sensitivity analysis had only a relatively small effect on the overall and incremental costs, owing primarily to the modest proportion of patients on dialysis and the relatively low baseline risk of mortality.
In terms of resource use, costs associated with the diagnosis of AbMR were not captured in the model. Diagnosing AbMR is relatively resource intensive, requiring histologic evidence of acute tissue injury, evidence of antibody interaction with the vascular endothelium (such as a peritubular C4d stain), and serologic evidence of DSACitation6. However, while data are available on the sensitivity and specificity of C4d staining as a predictor of microvascular inflammation, we were unable to identify similar data for the full AbMR diagnostic protocolCitation39. In the absence of these data, the model assumed that AbMR diagnosis costs would be the same, regardless of tacrolimus formulation. While the omission of these costs should not affect the projected cost difference between once- and twice-daily tacrolimus, the absolute cost projections may represent an under-estimate.
The present modeling analysis has demonstrated that Advagraf would be cost-saving relative to Prograf in renal transplant recipients in the UK setting, with cost savings driven by reduced costs associated with dialysis, treatment of AbMR, and primary immunosuppressive medication. As previous studies have shown Advagraf to have a well-characterized efficacy and safety profile in the prophylaxis of graft rejection, this study provides evidence that it may also result in substantial cost savings in the UK setting. These findings, combined with the previously-reported patient preference for once-daily over twice-daily immunosuppressive medicationCitation40, suggest that Advagraf is not only preferred by patients, but may also reduce the incidence of AbMR in UK renal transplant recipients and represent a clinically and economically prudent choice for immunosuppression in renal transplant recipients in the UK.
Transparency
Declaration of funding
This study was supported by funding from Astellas Pharma EMEA Limited.
Declaration of financial/other relationships
GM and IO are full-time employees of Astellas Pharma EMEA Limited, the manufacturer of Prograf and Advagraf. RP is a full-time employee of Ossian Health Economics and Communications GmbH, which received consultancy fees from Astellas Pharma EMEA Limited to perform the modeling analysis and prepare the manuscript. JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
References
- Hariharan S, Johnson CP, Bresnahan BA, et al. Improved graft survival after renal transplantation in the United States, 1988 to 1996. N Engl J Med 2000;342:605-12
- Lodhi SA, Lamb KE, Meier-Kriesche HU. Solid organ allograft survival improvement in the United States: the long-term does not mirror the dramatic short-term success. Am J Transplant 2011;11:1226-35
- Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant 2004;4:378-83
- Lamb KEL, Sundus A, Meier-Kriesche, et al. Long-term renal allograft survival in the United States: a critical reappraisal. Am J Transplant 2011;11:450-62
- Meier-Kriesche HU, Schold JD, Kaplan B. Long-term renal allograft survival: have we made significant progress or is it time to rethink our analytic and therapeutic strategies? Am J Transplant 2004;4:1289-95
- Djamali A, Kaufman DB, Ellis TM, et al. Diagnosis and management of antibody-mediated rejection: current status and novel approaches. Am J Transplant 2014;14:255-71
- Mengel M, Sis B, Haas M, et al; Banff meeting report writing committee. Banff 2011 meeting report: new concepts in antibody-mediated rejection. Am J Transplant 2012;12:563-70
- Halloran PF, de Freitas DG, Einecke G, et al. An integrated view of molecular changes, histopathology and outcomes in kidney transplants. Am J Transplant 2010;10:2223-30
- Sellarés J, de Freitas DG, Mengel M, et al. Understanding the causes of kidney transplant failure: the dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 2012;12:388-99
- Dew MA, DiMartini AF, De Vito Dabbs A, et al. Rates and risk factors for nonadherence to the medical regimen after adult solid organ transplantation. Transplantation 2007;83:858-73
- Dharancy S, Giral M, Tetaz R, et al. Adherence with immunosuppressive treatment after transplantation: results from the French trial PREDICT. Clin Transplant 2012;26:E293-9
- Weng FL, Israni AK, Joffe MM, et al. Race and electronically measured adherence to immunosuppressive medications after deceased donor renal transplantation. J Am Soc Nephrol 2005;16:1839-48
- National Health Service Business Services Authority. Prescription Cost Analysis (PCA) Data. Newcastle upon Tyne: National Health Service Business Services Authority, 2013. http://www.nhsbsa.nhs.uk/PrescriptionServices/3494.aspx. Accessed March 19, 2015
- Everly MJ, Everly JJ, Arend LJ, et al. Reducing de novo donor-specific antibody levels during acute rejection diminishes renal allograft loss. Am J Transplant 2009;9:1063-71
- Kim M, Martin ST, Townsend KR, et al Antibody-mediated rejection in kidney transplantation: a review of pathophysiology, diagnosis, and treatment options. Pharmacotherapy 2014;34:733-44
- European Medicines Agency Committee for Orphan Medicinal Products. Minutes of the 4 – 6 February 2014 meeting. London: European Medicines Agency, 2014. http://www.ema.europa.eu/docs/en_GB/document_library/Minutes/2014/04/WC500165700.pdf. Accessed March 19, 2015
- Kuypers DR, Peeters PC, Sennesael JJ, et al; ADMIRAD Study Team. Improved adherence to tacrolimus once-daily formulation in renal recipients: a randomized controlled trial using electronic monitoring. Transplantation 2013;95:333-40
- R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. 2012. ISBN 3-900051-07-0. http://www.R-project.org/. Accessed June 19, 2015
- Goulet V, Dutang C, Maechler M, et al. [email protected]. expm: Matrix exponential. R package version 0.99-1.1. Zürich: expm Developers, 2014. http://CRAN.R-project.org/package=expm. Accessed June 19, 2015
- Edinburgh Renal Unit. Transplant Handbook. Treatment of Acute antibody mediated rejection. Edinburgh: Edinburgh Renal Unit, 2013. http://www.edren.org/pages/handbooks/transplant-handbook/immunosuppression-protocol/treatment-of-acute-antibody-mediated-rejection.php. Accessed March 19, 2015
- Joint Formulary Committee. British National Formulary. 68th ed. London: BMJ Group and Pharmaceutical Press, 2014
- National Health Service. NHS reference costs 2013 to 2014. London: National Health Service, 2014. https://www.gov.uk/government/publications/nhsreference-costs-2013-to-2014. Accessed July 28, 2015
- NHS Blood and Transplant. Cost-effectiveness of transplantation. Watford: National Health Service Blood Transplant, 2009. http://www.organdonation.nhs.uk/newsroom/fact_sheets/cost_effectiveness_of_transplantation.asp. Accessed May 12, 2015
- The Renal Association. Clinical Practice Guidelines Module 2: Haemodialysis. Petersfield: The Renal Association, 2007. http://www.renal.org/docs/default-source/guidelines-resources/Module_3a_-_Haemodialysis_-_4th_Edition.pdf. Accessed May 12, 2015
- Krämer BK, Charpentier B, Bäckman L, et al; Tacrolimus Prolonged Release Renal Study Group. Tacrolimus once daily (Advagraf) versus twice daily (Prograf) in de novo renal transplantation: a randomized phase III study. Am J Transplant 2010;10:2632-43
- Sullivan SD, Mauskopf JA, Augustovski F, et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health 2014;17:5-14
- The National Institute for Health and Care Excellence. Guide to the methods of technology appraisal. London: The National Institute for Health and Care Excellence, 2013. http://www.nice.org.uk/article/PMG9/chapter/Foreword. Accessed March 19, 2015
- Pinsky BW, Takemoto SK, Lentine KL, et al. Transplant outcomes and economic costs associated with patient noncompliance to immunosuppression. Am J Transplant 2009;9:2597-606
- Butler JA, Roderick P, Mullee M, et al. Frequency and impact of nonadherence to immunosuppressants after renal transplantation: a systematic review. Transplantation 2004;77:769-76
- Zhang J, Yu KF. What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998;280:1690-1
- Kaposztas Z, Podder H, Mauiyyedi S, et al. Impact of rituximab therapy for treatment of acute humoral rejection. Clin Transplant 2009;23:63-73
- Everly MJ, Everly JJ, Susskind B, et al. Bortezomib provides effective therapy for antibody- and cell-mediated acute rejection. Transplantation 2008;12:1754-61
- Biglarnia AR, Nilsson B, Nilsson T, et al. Prompt reversal of a severe complement activation by eculizumab in a patient undergoing intentional ABO-incompatible pancreas and kidney transplantation. Transpl Int 2011;8:e61-6
- Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 1999;341:1725-30
- Sabbatini M, Garofalo G, Borrelli S, et al. Efficacy of a reduced pill burden on therapeutic adherence to calcineurin inhibitors in renal transplant recipients: an observational study. Patient Prefer Adherence 2014;8:73-81
- Eberlin M, Otto G, Krämer I. Increased medication compliance of liver transplant patients switched from a twice-daily to a once-daily tacrolimus-based immunosuppressive regimen. Transplant Proc 2013;45:2314-20
- Beckebaum S, Iacob S, Sweid D, et al. Efficacy, safety, and immunosuppressant adherence in stable liver transplant patients converted from a twice-daily tacrolimus-based regimen to once-daily tacrolimus extended-release formulation. Transpl Int 2011;24:666-75
- Puttarajappa C, Shapiro R, Tan HP. Antibody-mediated rejection in kidney transplantation: a review. J Transplant 2012;12:193724
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant 2009;9(3 Suppl):S1-155
- Loupy A, Hill GS, Suberbielle C, et al. Significance of C4d Banff scores in early protocol biopsies of kidney transplant recipients with preformed donor-specific antibodies (DSA). Am J Transplant 2011;11:56-65
- Guirado L, Cantarell C, Franco A, et al; GREAT Study Group. Efficacy and safety of conversion from twice-daily to once-daily tacrolimus in a large cohort of stable kidney transplant recipients. Am J Transplant 2011;11:1965-71
Appendix 5