
Abstract
Aims/hypothesis:
Continuous subcutaneous insulin infusion (CSII) is an important treatment option for type 1 diabetes patients unable to achieve adequate glycemic control with multiple daily injections (MDI). Combining CSII with continuous glucose monitoring (CGM) in sensor-augmented pump therapy (SAP) with a low glucose-suspend (LGS) feature may further improve glycemic control and reduce the frequency of hypoglycemia. A cost-effectiveness analysis of SAP + LGS vs CSII plus self-monitoring of blood glucose (SMBG) was performed to determine the health economic benefits of SAP + LGS in type 1 diabetes patients using CSII in the UK.
Methods:
Cost-effectiveness analysis was performed using the CORE diabetes model. Treatment effects were sourced from the literature, where SAP + LGS was associated with a projected HbA1c reduction of −1.49% vs −0.62% for CSII, and a reduced frequency of severe hypoglycemia. The time horizon was that of patient lifetimes; future costs and clinical outcomes were discounted at 3.5% and 1.5% per annum, respectively.
Results:
Projected outcomes showed that SAP + LGS was associated with higher mean quality-adjusted life expectancy (17.9 vs 14.9 quality-adjusted life years [QALYs], SAP + LGS vs CSII), and higher life expectancy (23.8 vs 21.9 years), but higher mean lifetime direct costs (GBP 125,559 vs GBP 88,991), leading to an incremental cost-effectiveness ratio (ICER) of GBP 12,233 per QALY gained for SAP + LGS vs CSII. Findings of the base-case analysis remained robust in sensitivity analyses.
Conclusions/interpretation:
For UK-based type 1 diabetes patients with poor glycemic control, the use of SAP + LGS is likely to be cost-effective compared with CSII plus SMBG.
Introduction
Recent estimates suggest that in the UK there are just under a quarter of a million people living with type 1 diabetesCitation1, with the annual direct costs of treatment in 2010/2011 estimated at ∼GBP 1 billionCitation2. An estimated 70% of total direct costs are due to long-term complications of the disease, which include cardiovascular disease, renal disease, and ophthalmic problemsCitation2. The chronic nature of the disease, combined with high direct costs, make long-term cost-effectiveness analyses pivotal in informing payer decisions regarding the reimbursement/funding of new therapeutic technologies.
Patients with type 1 diabetes require lifetime treatment with exogenous insulin for survival, and landmark studies such as the Diabetes Control and Complications Trial have shown that good glycemic control is fundamental in reducing the risk of developing long-term diabetes-related complicationsCitation3. Current optimized or intensive insulin administration regimens that aim to achieve strict glycemic control are multiple daily injections (MDI) and continuous subcutaneous insulin infusion (CSII, insulin pump therapy). Guidance from the UK National Institute for Health and Care Excellence (NICE) states the CSII is indicated for patients with type 1 diabetes (adults and children aged ≥12 years) if, despite optimization of MDI, HbA1c remains ≥8.5% (69 mmol/mol), or when reaching HbA1c targets with MDI results in disabling hypoglycemiaCitation4. NICE also recommends CSII in children younger than 12 years if MDI is considered impractical or inappropriate. In the UK, insulin pumps were used by an estimated 6% of adult and 19% of pediatric type 1 diabetes patients in a survey performed in 2012Citation5. As such, the usage of insulin pumps in the UK is considerably below that reported in many other European settings and in the US, where an estimated 40% of people with type 1 diabetes use an insulin pumpCitation6.
Insulin pumps have been used in type 1 diabetes since the 1970sCitation7; however, a more recent advance in insulin pump technology and its clinical use is sensor-augmented pump (SAP) therapy, where CSII is used in conjunction with data from continuous glucose monitoring (CGM), either with the signal from a subcutaneously implanted glucose sensor wirelessly transmitted to a wearable or hand-held receiver or to a compatible insulin pump. This allows patients themselves to use CGM data as an aid to further improve glycemic control with CSII. Some SAP systems also employ pumps with a low-glucose insulin-suspend (LGS) feature, whereby the delivery of basal insulin is suspended for up to 2 h when CGM-measured low glucose levels are detected. SAP with LGS have been shown to reduce both HbA1cCitation8–10 and the frequency of hypoglycemiaCitation10–14 in patients with type 1 diabetes.
In spite of evidence for its clinical efficacy, SAP is not widely used, and one barrier to uptake may be cost. Previous analyses have shown that, in several settings, CSII is cost-effective relative to MDI in type 1 diabetesCitation15–17. The cost-effectiveness of SAP is not well studied, although recent reports showed SAP to be cost-effective relative to CSII alone in the SwedishCitation18 and Australian settingCitation19. Given the clinical benefits associated with SAP + LGS, a long-term cost-effectiveness analysis of SAP + LGS vs CSII plus self-monitoring of blood glucose (SMBG) was performed to establish if SAP + LGS is cost-effective in the UK setting for type 1 diabetes patients.
Methods
Simulation cohort and treatment effects
A summary of baseline characteristics of the simulation cohort is provided in . The mean age of the cohort was 27 years, mean duration of diabetes 13 years, and mean HbA1c at baseline 10% (86 mmol/mol). The additional glycemic (HbA1c lowering) effect of CGM with CSII vs CSII with SMBG was sourced from an individual patient data meta-analysisCitation20. From this, everyday use of SAP was projected to lead to an HbA1c reduction of −1.49% vs −0.62% for CSII alone. Use of SMBG strips in the SAP + LGS arm was assumed to be lower than for CSII alone, based on findings from an observational study conducted in SwedenCitation21, where CGM reduced SMBG use from a mean 7.11 SMBG strips and lancets per day to 4.35 per day. SAP + LGS vs CSII alone was also projected to lead to a reduction in the frequency of severe hypoglycemic events, based on a randomized controlled trial of SAP with LGS vs CSII conducted in type 1 diabetes patients in AustraliaCitation14. In this study, the rate of severe hypoglycemic events in the SAP + LGS group was 0 per 100 patient months compared with 2.2 per 100 patient months in the CSII-alone group.
Table 1. Baseline cohort characteristics and treatment effects.
The impact of reduced fear of hypoglycemia in the SAP + LGS group was also included in the analysis, based on the findings of Nørgaard et al.Citation22, who reported that the use of SAP vs CSII alone was associated with a reduction of 6.9 units in the Hypoglycemia Fear Survey (HFS) score. A 1-unit increase in HFS score has been shown to correspond to a 0.008 unit decrease in the EQ-5D index score, a measure of health-related quality-of-lifeCitation23; the 6.9 unit difference in HFS score between the two arms was, therefore, translated into a utility benefit of 0.0552, which was applied to the SAP + LGS arm.
Model description
The analysis was performed using the CORE Diabetes Model (CDM; IMS Health, Basel, Switzerland). The CDM is a validated non-product-specific policy analysis tool for cost-effectiveness analysis in both type 1 and type 2 diabetes; a detailed description of the model architecture (including schematic diagrams) and validation is available in publications by Palmer et al.Citation24,Citation25 and, more recently, McEwan et al.Citation26. In summary, the model is based on a series of inter-dependent sub-models that simulate both acute and long-term diabetes-related complications (angina, myocardial infarction, congestive heart failure, stroke, peripheral vascular disease, diabetic retinopathy, macula edema, cataract, hypoglycemia, ketoacidosis, lactic acidosis, depression, edema, nephropathy and end-stage renal disease, neuropathy, foot ulcer and amputation, and non-specific mortality). The sub-models have a semi-Markov structure and use time, state, time-in-state, and diabetes type-dependent probabilities derived from published sources to simulate disease progression. Monte Carlo simulation using tracker variables is used to overcome the memory-less properties of the standard Markov model and allows for interconnectivity and interaction between individual sub-models.
Costs and utilities
The base-case analysis was performed from the perspective of the UK National Health Service (a secondary analysis was also performed using a societal perspective). Direct costs were sourced from published literature and, where necessary, were inflated to 2013 GBPCitation27–37. In the sensitivity analysis using the societal perspective, indirect costs were calculated based on the human capital approach, using average annual salaries for the UK. Days off work were sourced from a study conducted in the Netherlands (Medtronic International Trading Sarl, Tolochenaz, Switzerland; data on file, available on request).
For treatment costs, only the incremental costs between the two arms were considered, namely the different frequency of use of SMBG strips and lancets between CSII alone and SAP + LGS therapy, and use of the CGM transmitter and glucose sensors. Average UK costs for glucose sensors and sensor transmitters were taken to be costs of Enlite sensors and MiniLink transmitters (Medtronic) and the costs of SMBG strips and lancets were sourced from the British National Formulary 63 (March 2012)Citation38.
Health state utility values were taken from published literatureCitation39 and references therein.
Statistical approach and other model settings
For each simulation, a simulated cohort of 1000 patients was run through the model 1000 times using first-order Monte Carlo simulation. Long-term outcomes included total direct costs, life expectancy, quality-adjusted life expectancy, and time to onset of complications. Future costs were discounted at a rate of 3.5% per annum and clinical outcomes were discounted at a rate of 1.5% per annum in line with NICE guidance on long-term conditions, where treatment effects are sustained over a prolonged period of timeCitation40. The mean values from the simulation (a total of 1000 mean values, each from a cohort of 1000 patients run through the model) were then used to generate scatterplots of incremental costs vs incremental effectiveness (quality-adjusted life years [QALYs]) for SAP + LGS vs CSII. Data from the scatterplot were then used to generate a cost-effectiveness acceptability curve.
Sensitivity analysis
In order to explore the robustness of the base-case findings and establish the key drivers of results, a series of one-way and two-way sensitivity analyses were performed around key input parameters: the utility benefit associated with SAP + LGS due to reduced fear of hypoglycemia was negated; the SAP + LGS -associated benefit from reduced severe hypoglycemia was negated (an event rate of 2.6 events per 100 patient years was applied in both treatment arms); the baseline HbA1c was set to 9.0% (75 mmol/mol) and 8.1% (65 mmol/mol); a discount rate of 3.5% per annum was applied to both future costs and clinical outcomes; and an analysis was conducted from the societal perspective. A two-way sensitivity analyses was also performed in which both the benefits from reduced fear of hypoglycemia and reduced frequency of severe hypoglycemia with SAP + LGS therapy were negated.
Results
Cost-effectiveness of SAP vs CSII in the base case
In the base-case analysis (payer perspective) the use of SAP + LGS therapy was associated with an improvement in life expectancy of 1.9 years (23.8 years vs 21.9 years) and an improvement in quality-adjusted life expectancy of 3.0 QALYs) (17.9 QALYs vs 14.9 QALYs), compared with CSII alone (). Total direct lifetime costs were GBP 36,568 higher for the SAP + LGS group than for the CSII group (GBP 125,559 vs GBP 88,991), resulting in an incremental cost-effectiveness ratio (ICER) of GBP 12,233 per QALY gained for SAP + LGS vs CSII alone.
Table 2. Summary of base-case results.
The use of SAP + LGS relative to CSII was also projected to delay the mean onset of diabetes-related complications (). The most pronounced delays were seen in the projected onset of first ulcer and gross proteinuria, the onset of which was delayed by an average of over 3.5 years in the SAP + LGS group compared with the CSII-alone group.
Table 3. Delay in onset of diabetes-related complications with SAP + LGS vs CSII alone.
Sensitivity analyses
In the sensitivity analysis conducted from the societal perspective, which captures indirect costs due to lost productivity, the ICER was lower at GBP 3359 per QALY gained for SAP + LGS vs CSII. The higher overall direct costs were driven mainly by the higher incremental treatment costs for SAP + LGS (GBP 59,561 for SAP vs GBP 14,238 for CSII); however, this was partially offset by lower complication costs, particularly renal and ulcer/amputation/nephropathy-related costs, due to improved glycemic control. Indeed, total mean per patient lifetime costs for ulcer/amputation/nephropathy were GBP 4951 lower with SAP + LGS than with CSII (). It is important to note that, as projected life expectancy was 1.9 years higher in the SAP group than the CSII group, the time spent at risk for complications was higher for the SAP group, which will be a contributing factor in the higher overall lifetime costs in the SAP group.
The robustness of the base-case results was also explored using a series of one-way and two-way sensitivity analyses (), where the results of the analyses remained robust despite changes in key input parameters. In the analysis where both SAP-related benefits associated with reduced fear of hypoglycemia and reduced incidence of severe hypoglycemia were negated, the ICER increased to GBP 26,600 per QALY gained. In one-way sensitivity analyses in which baseline HbA1c was decreased to 9.0% (75 mmol/mol) and 8.1% (65 mmol/mol) (compared with 10.0% [86 mmol/mol] in the base case), the ICER increased to GBP 13,840 and GBP 15,392 per QALY gained, respectively. Sensitivity analysis around discount rates influenced the ICER as expected (use of undiscounted results led to an increased ICER; data not shown). A sensitivity analysis was also performed using a discount rate of 3.5% per annum for both future costs and clinical outcomes. In this scenario the ICER was increased to GBP 18,371 per QALY gained.
Table 4. Summary findings of sensitivity analyses.
Cost-effectiveness and willingness-to-pay
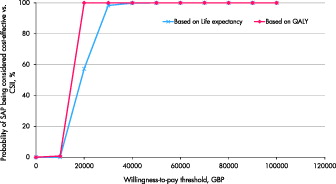
Analysis of the cost-effectiveness acceptability curve showed that, at a willingness-to-pay threshold of between GBP 20,000–30,000 per QALY gained, SAP + LGS is likely to be considered cost-effective compared with CSII alone in the UK ().
Figure 1. Cost-effectiveness acceptability curve for SAP + LGS vs CSII. CSII, continuous subcutaneous insulin infusion; QALY, quality-adjusted life year; SAP, sensor-augmented pump.
Discussion
Our long-term cost-effectiveness analysis suggests that, with the commonly used willingness-to-pay threshold of between GBP 20,000–30,000 per QALY gained, SAP + LGS is likely to be cost-effective vs CSII alone for patients with poorly-controlled type 1 diabetes in the UK. The ICER was GBP 12,233 per QALY gained with a baseline HbA1c of 10% (86 mmol/mol), GBP 13,840 per QALY gained for an HbA1c of 9% (75 mmol/mol), and GBP 15,392 per QALY gained at an HbA1c of 8.1% (65 mmol/mol).
From the perspective of the payer, although SAP + LGS was associated with higher direct treatment costs vs CSII alone, this is at least partially offset by reduced long-term complication costs due to improved glycemic control, as well as a reduction in the incidence of severe hypoglycemic events. Indeed, the improved glycemic control resulting from the use of SAP + LGS delayed the onset of all complications considered in the analysis by at least 2 years. From the perspective of the patient, SAP + LGS is associated with improved quality-of-life due to reduced risk of tissue complications, reduced frequency of severe hypoglycemic events, and a reduced fear of hypoglycemia.
The present analysis is among the first to capture the health economic benefits of SAP + LGS in terms of reduced fear of hypoglycemia. A substantial proportion of type 1 diabetes patients, particularly those with past severe hypoglycemic events, report having fear of hypoglycemia. This can negatively impact health-related quality-of-lifeCitation41,Citation42, and can result in detrimental behavior patterns such as deliberately decreasing insulin dose to maintain a “safety net” in terms of blood glucose levels and thereby reducing the likelihood of a hypoglycemic eventCitation41,Citation42. The security provided by SAP, and in particular the LGS feature, may give patients the confidence to try to achieve lower glycemic targets than they would otherwise, and this improved glycemic control would in turn reduce the risk of progressing to late stage diabetes-related complications. However, sensitivity analysis showed that, even when the benefit of reduced fear of hypoglycemia was negated, SAP + LGS is likely to remain cost-effective relative to CSII alone in patients with poorly controlled disease. In addition to a quality-of-life benefit associated with reduced fear of hypoglycaemia, a recent study by McQueen et al.Citation43 showed that, in type 1 diabetes, improved HbA1c was also associated with improved quality-of-life, independent of other factors, with a 1% increase in HbA1c corresponding to a −0.027 (95% CI = −0.049–0.006) decrease in utility. This potential benefit was not captured in the current analysis, thereby potentially making the findings of the analysis conservative.
A limitation of our study is that evidence for the effectiveness of SAP at reducing severe hypoglycemia is relatively limited: a randomized controlled trialCitation14 used SAP with LGS (not standard SAP) vs CSII, although the marked effectiveness of both standard SAP and SAP plus LGS at reducing severe hypoglycemia was confirmed in an observational study of patients with problematic severe hypoglycemia, despite structured diabetes education and insulin pump therapyCitation12. A further limitation allied to this is that the paucity of clinical data comparing SAP with CSII in type 1 diabetes meant that it was necessary to use multiple input sources for clinical data: Treatment effects relating to HbA1c were sourced from an individual patient level meta-analysisCitation20 and clinical data relating to hypoglycemia event rates were taken from a randomized controlled trial conducted in type 1 diabetes patients in AustraliaCitation14.
In conclusion, the findings of long-term cost-effectiveness analysis suggest that, for patients with poorly controlled type 1 diabetes already using CSII, the switch to SAP + LGS is likely to be cost-effective in the UK setting, largely due to improved glycemic control, which in turn leads to a lower incidence of long-term complications, together with reduced fear of hypoglycemia and a reduced incidence of actual severe hypoglycemic events. Moreover, sensitivity analyses showed that the clinical and economic benefits of SAP + LGS relative to CSII alone are largest in patients with poorer levels of baseline glycemic control.
| Abbreviations | ||
| CDM | = | CORE Diabetes Model |
| CGM | = | Continuous glucose monitoring |
| CSII | = | Continuous subcutaneous insulin infusion |
| GBP | = | Great Britain pound |
| HFS | = | Hypoglycemia Fear Survey |
| ICER | = | Incremental cost-effectiveness ratio |
| LGS | = | Low-glucose insulin suspend |
| MDI | = | Multiple daily injections |
| NICE | = | National Institute for Health and Care Excellence |
| QALY | = | Quality-adjusted life year |
| SAP | = | Sensor augmented pump therapy |
| SMBG | = | Self-monitoring of blood glucose |
Transparency
Declaration of funding
This study was supported by funding from Medtronic International Trading Sàrl.
Declaration of financial/other relationships
SR is a current employee of HEVA HEOR, which has received consulting fees from Medtronic. JSP and WV are current employees of Ossian Health Economics and Communications, which has received consulting fees from Medtronic. MC and MJ are current employees of Medtronic UK. SP is a current employee of Medtronic International Trading Sàrl. JCP has received speaker and/or consultancy fees from Medtronic, Roche, Cequr and Cellnovo, manufacturers of insulin pumps and/or CGM systems. JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Related Research Data
References
- Hammond P. Improving access to insulin pump therapy: the role of the Insulin Pump Network. J Diabetes Nursing 2013;17:175-9
- Hex N, Bartlett C, Wright D, et al. Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet Med 2012;29:855-62
- Diabetes Control and Complications Trial Research Group (1993). The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977-86
- National Institute for Health and Care Excellence. TA151 Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus. London, UK: National Institute for Health and Care Excellence; 2008. http://www.nice.org.uk/guidance/ta151/chapter/1-guidance. Accessed October 28, 2014
- Diabetes UK. The United Kingdom insulin pump audit – service level data. London, UK: Diabetes UK; 2013. http://www.diabetes.org.uk/Documents/News/The_United_Kingdom_Insulin_Pump_Audit_May_2013.pdf. Accessed February 3, 2015
- Pickup J. Insulin pumps. Int J Clin Pract Suppl 2011;170:16-19
- Pickup JC, Keen H, Parsons JA, et al. Continuous subcutaneous insulin infusion: an approach to achieving normoglycaemia. BMJ 1978;i:204-7
- O’Connell MA, Donath S, O’Neal DN, et al. Glycaemic impact of patient-led use of sensor-guided pump therapy in type 1 diabetes: a randomised controlled trial. Diabetologia 2009;52:1250
- Raccah D, Sulmont V, Reznik Y, et al. Incremental value of continuous glucose monitoring when starting pump therapy in patients with poorly controlled type 1 diabetes. Diabetes Care 2009;32:2245
- Battelino T, Conget I, Olsen B, et al. The use and efficacy of continuous glucose monitoring in type 1 diabetes treated with insulin pump therapy: a randomised controlled trial. Diabetologia 2012;55:3155-62
- Choudhary P, Shin J, Wang Y, et al. Insulin pump therapy with automated insulin suspension in response to hypoglycemia: reduction in nocturnal hypoglycemia in those at greatest risk. Diabetes Care 2011;34:2023-5
- Choudhary P, Ramasamy S, Green L, et al. Real-time continuous glucose monitoring significantly reduces severe hypoglycemia in hypoglycemia-unaware patients with type 1 diabetes. Diabetes Care 2013;36:4160-2
- Bergenstal RM, Klonoff DC, Garg SK, et al. Threshold-based insulin-pump interruption for reduction of hypoglycemia. N Engl J Med 2013;369: 224-32
- Ly TT, Nicholas JA, Retterath A, et al. Effect of sensor-augmented insulin pump therapy and automated insulin suspension vs standard insulin pump therapy on hypoglycemia in patients with type 1 diabetes: a randomized clinical trial. JAMA 2013;310:1240-7
- St Charles ME, Sadri H, Minshall ME, et al. Health economic comparison between continuous subcutaneous insulin infusion and multiple daily injections of insulin for the treatment of adult type 1 diabetes in Canada. Clin Ther 2009;31:657-67
- St Charles M, Lynch P, Graham C, et al. A cost-effectiveness analysis of continuous subcutaneous insulin injection versus multiple daily injections in type 1 diabetes patients: a third-party US payer perspective. Value Health 2009;12:674-86
- Cohen N, Minshall ME, Sharon-Nash L, et al. Continuous subcutaneous insulin infusion versus multiple daily injections of insulin: economic comparison in adult and adolescent type 1 diabetes mellitus in Australia. Pharmacoeconomics 2007;25:881-97
- Roze S, Saunders R, Brandt A, et al. Health-economic analysis of real-time continuous glucose monitoring in people with Type 1 diabetes. Diabet Med 2015;32:618-26
- Ly T, Brnabic AJM, Eggleston A, et al. A cost-effectiveness analysis of sensor-augmented insulin pump therapy and automated insulin suspension versus standard pump therapy for hypoglycemic unaware patients with type 1 diabetes. Value Health 2014;17:561-9
- Pickup JC, Freeman SC, Sutton AJ. Glycaemic control in type 1 diabetes during real time continuous glucose monitoring compared with self monitoring of blood glucose: meta-analysis of randomised controlled trials using individual patient data. BMJ 2011;343:d3805
- Lynch P, Attvall S, Persson S, et al. Routine use of personal glucose monitoring system with insulin pump use in Sweden. Abstract presented at the 48th annual meeting of the European Association for the Study of Diabetes. 1–5 October 2012, Berlin, Germany. Diabetologia 2012;55(1 Suppl)S432
- Nørgaard K, Scaramuzza A, Bratina N, et al. Routine sensor-augmented pump therapy in type 1 diabetes: the INTERPRET study. Diabetes Technol Ther 2013;15:273-80
- Currie CJ, Morgan CL, Poole CD, et al. Multivariate models of health-related utility and the fear of hypoglycaemia in people with diabetes. Curr Med Res Opin 2006;22:1523-34
- Palmer AJ, Roze S, Valentine WJ, et al. The CORE Diabetes Model: projecting long-term clinical outcomes, costs and cost-effectiveness of interventions in diabetes mellitus (types 1 and 2) to support clinical and reimbursement decision-making. Curr Med Res Opin 2004;20(1 Suppl):S5-26
- Palmer AJ, Roze S, Valentine WJ, et al. Validation of the CORE Diabetes Model against epidemiological and clinical studies. Curr Med Res Opin 2004;20(1 Suppl):S27-40
- McEwan P, Foos V, Palmer JL, et al. Validation of the IMS CORE Diabetes Model. Value Health 2014;17:714-24
- National Institute for Health and Care Excellence. NICE clinical guideline 48. London, UK: National Institute for Health and Care Excellence; 2007. http://www.nice.org.uk/guidance/cg48/resources/guidance-mi-secondary-prevention-secondary-prevention-in-primary-and-secondary-care-for-patients-following-a-myocardial-infarction-pdf. Accessed December 19, 2014
- Dyer MT, Goldsmith KA, Khan SN, et al. Clinical and cost-effectiveness analysis of an open label, single-centre, randomised trial of spinal cord stimulation (SCS) versus percutaneous myocardial laser revascularisation (PMR) in patients with refractory angina pectoris: The SPiRiT trial. Trials 2008;9:40
- Cameron CG, Bennett HA. Cost-effectiveness of insulin analogues for diabetes mellitus. CMAJ 2009;180:400-7
- National Institute for Health and Care Excellence. NICE technology appraisal guidance 94. London, UK: NICE; 2006. http://www.nice.org.uk/guidance/ta94/resources/guidance-statins-for-the-prevention-of-cardiovascular-events-pdf. Accessed December 19, 2014
- Youman P, Wilson K, Harraf F, et al. The economic burden of stroke in the United Kingdom. Pharmacoeconomics 2003;21(1 Suppl):43-50
- UK National Institute for Health and Care Excellence. NICE clinical guideline 73. London, UK: UK National Institute for Health and Care Excellence; 2008. http://www. nice.org.uk/guidance/cg73/resources/guidance-chronic-kidney-disease-early-identification-and-management-of-chronic-kidney-disease-in-adults-in-primary-and-secondary-care-pdf. Accessed December 19, 2014
- UK National Institute for Health and Care Excellence. NICE clinical guideline 87. Type 2 diabetes. The management of type 2 diabetes. London, UK: UK National Institute for Health and Care Excellence; 2008. https://www.nice.org.uk/guidance/cg87/resources/guidance-type-2-diabetes-pdf. Accessed December 19, 2014
- Clarke P, Gray A, Legood R, et al. The impact of diabetes-related complications on healthcare costs: results from the United Kingdom Prospective Diabetes Study (UKPDS Study No. 65). Diabet Med 2003;20:442-50
- Meads C, Hyde C. What is the cost of blindness? Br J Ophthalmol 2003;87:1201-4
- Ghatnekar O, Willis M, Persson U. Cost-effectiveness of treating deep diabetic foot ulcers with Promogran in four European countries. J Wound Care 2002;11:70-4
- UK Government Department of Health. UK National Health Service reference costs 2012–2013. London, UK: UK Government Department of Health, 2013. https://www.gov.uk/government/publications/nhs-reference-costs-2012-to-2013. Accessed December 19, 2014
- British National Formulary 63 (March 2012). London, UK; 2012. https://www.medicinescomplete.com/about/publications.htm. Accessed December 19, 2014
- Beaudet A, Clegg J, Thuresson PO, et al. Review of utility values for economic modeling in type 2 diabetes. Value Health 2014;17:462-70
- National Institute for Health and Clinical Excellence. Discounting of health benefits in special circumstances. London, UK: National Institute for Health and Clinical Excellence; 2011. http://www.nice.org.uk/media/955/4F/Clarification_to_section_5.6_of_the_Guide_to_Methods_of_Technology_Appraisals.pdf. Accessed December 14, 2014
- Böhme P, Bertin E, Cosson E, et al., GEODE group. Fear of hypoglycemia in patients with type 1 diabetes: do patients and diabetologists feel the same way? Diabetes Metab 2013;39:63-70
- Fidler C, Elmelund Christensen T, et al. Hypoglycemia: an overview of fear of hypoglycemia, quality-of-life, and impact on costs. J Med Econ 2011;14:646-55
- McQueen RB, Ellis SL, Maahs DM, et al. Association between glycated hemoglobin and health utility for Type 1 diabetes. Patien 2014;7:197-205