
Abstract
Background:
Regionally or distantly metastatic melanoma (stages IIIB/C and IV) place a high burden on society. To quantify this burden, this study estimated years of life lost (YLL) per patient for adults with metastatic melanoma in 12 countries in 2014.
Methods:
General population growth and life expectancy were estimated from the Organization for Economic Co-operation and Development data and life tables for each country. Incidence of melanoma and mortality rates for the disease were based on GLOBOCAN and US registry data. The prevalence of metastatic melanoma was calculated using mortality rates and survival data from patients with melanoma. YLL per patient was estimated by the difference between the disease-free life expectancy and the life expectancy with metastatic melanoma.
Results:
YLL per patient were as follows: Australia, men = 19.9 years, women = 22.7 years; Brazil, 16.3, 19.8; Canada, 19.4, 22.3; France, 18.8, 23.1; Germany, 18.3, 20.8; Italy, 19.3, 22.7; Mexico, 17.2, 19.0; the Netherlands, 18.5, 21.5; Spain, 19.2, 23.1; Sweden 19.4, 22.0; the UK, 18.7, 21.2; and the US, 17.9, 20.6.
Conclusions:
The burden of metastatic melanoma as measured by YLL is substantial in all 12 countries; although there is variation across countries and between men and women.
Introduction
Regionally or distantly metastatic melanoma (stages IIIB/C and IV) is a life threatening malignant tumorCitation1–4. Median overall survival (OS) varies by stage, ranging from ∼24 months for patients with stages IIIB/C to 5–10 months for patients with stage IV M1cCitation5. Compared with other cancers, a relatively high proportion of people diagnosed with melanoma are younger adults and this age distribution is generally consistent across countries. Thirty-four per cent of all melanomas diagnosed in 2012 worldwide were in people younger than 55 years of ageCitation6,Citation7.
Little has been published to date on the burden of metastatic melanoma and in particular on the number of years of life lost (YLL) due to metastatic melanomaCitation4,Citation8–10. Mortality rates have been reported;, however, crude mortality rates are not a sufficient indicator of the burden to society, particularly for diseases that affect younger people and result in premature death, and years of lost work productivity. YLL provides a more useful measure of disease burden by combining life expectancy and mortality data to estimate the average number of years that are lost because of premature death.
The aim of this study was to estimate YLL in patients with metastatic melanoma in 2014 in Australia, Brazil, Canada, France, Germany, Italy, Spain, Mexico, the Netherlands, Sweden, the UK, and the US. These 12 countries were selected to represent different regions and climates, and to include areas of significant disease prevalence.
Materials and methods
YLL is calculated by the difference in life expectancy with and without a given disease. At the population level, this is multiplied also by prevalence and population growth. All assumptions in this study were validated with clinical experts at several stages of the study.
Data sources
Data on general population growth, melanoma incidence, and mortality specific to each country were obtained using GLOBOCAN 2008Citation11. Disease-free life expectancy was obtained from statistical agencies in each countryCitation12–23. Survival by stage and the age distribution at melanoma diagnosis were based on a US database because no data could be identified specific to each country with the equivalent required level of detail. The only source of data on the stage distribution of melanoma at a detailed level was the American Joint Committee on Cancer (AJCC) reported by Balch et al.Citation24; we were able to determine stage III and stage IV proportions using country-specific publications, but we assumed that the sub-stage distribution reported by Balch et al. was the same for all countries in order to proceed with the calculations. The age distribution at diagnosis of melanoma was obtained from the 2006–2010 estimates from the Surveillance, Epidemiology, and End Results Program (SEER)Citation25. Therefore, the estimates here are more a reflection of general life expectancy with advanced melanoma rather than characteristics of life expectancy with advanced melanoma in each country.
The GLOBOCAN data were selected to ensure consistency of measurement across all countries; the SEER estimates and the work by Balch et al. represent the most up-to-date data on age distribution and survival by stage, respectively. Definition of adults was in accordance with the definitions used in the Organization for Economic Co-operation and Development (OECD) and GLOBOCAN 2008 databases, which was defined as individuals 15 years of age and over.
Prevalence of metastatic melanoma
Prevalence of melanoma was calculated by adding the estimated incident cases of melanoma in the current year and the number of patients surviving from melanoma from previous yearsCitation24. Then, the distribution of stages for the incident cases was applied to the estimate of the prevalence of melanoma to estimate the number of patients with stage IIIB/C or IV melanoma.
To determine the estimated prevalence in 2014, we applied country-specific, age-adjusted mean annual population growth between 2000–2010 and assumed that incidence remained a constant proportion of the total populationCitation11.
Distribution of age at diagnosis
SEER data from 2006–2010Citation25 were used to estimate the distribution of patients with metastatic melanoma across the 5 year age groups that were used by GLOBOCAN. We assumed that the distribution of patients across age groups was similar for all stages of metastatic disease (IIIB–IV).
Disease-free life expectancy calculation
Estimates of disease-free life expectancy were obtained from life tables for each countryCitation12–23. Some life tables reported life-expectancy for exact ages, whereas others did so for various age ranges; we, therefore, aggregated the data into age groups that matched those for the prevalence of metastatic melanoma, using a published algorithm for interpolating life expectancy based on intervals between the mismatched thresholdsCitation26. We assumed that the maximum life expectancy was 100 years of age (i.e., life tables displaying 100 and above years of age were truncated at 100 years of age).
Life expectancy with metastatic melanoma
Life expectancy with metastatic melanoma was calculated by estimating an annualized mortality rate for disease-free life expectancy and then applying that mortality rate to calculate life expectancy with the disease.
Specifically, life expectancy with metastatic melanoma was calculated by the following three steps:
A weighted average (WA) annualized mortality rate for people with advanced melanoma was calculated for each of the following periods after diagnosis: 0–1 years, 1–2 years, 2–5 years, and 5–10 years. Estimates of 1, 2, 5, and 10 year survivalCitation24 for stages IIIB–IV were used for this.
Disease-free life expectancy (DFLE) was extracted from life tables for each country.
To estimate life expectancy with metastatic melanoma (LEMM) in each age group, their future life expectancy was reduced in line with the WA annualized mortality rate with advanced melanoma using the following formula:
YLL per patient calculation
YLL per patient was estimated by calculating the difference between the disease-free life expectancy and the life expectancy with metastatic melanoma. This was done for both men and women and for each age group; the values were age-weighted using SEER data, taking into account the distribution of patients diagnosed with melanoma in each age group. YLL per patient was calculated for men and women, respectively. YLL per patient for all patients was calculated by using the ratios of men and women in each countryCitation21, using the following formula:
Results
The projected prevalence of metastatic melanoma in each country is shown in . The projected prevalence rate was highest in Australia (23.18 per 100,000 people) and lowest in Brazil (1.04 per 100,000).
Table 1. Projected prevalence of metastatic melanoma in 2014.
reports the distribution of age at melanoma diagnosis across the 5 year age groups used by GLOBOCAN (which were also used to estimate prevalence), which was estimated using SEER data from 2006–2010Citation25.
Table 2. Distribution of age at diagnosis, SEER, 2006–2010Citation13.
The estimated average survival rates, annualized mortality rates and the weighted and unweighted average annualized mortality rates are reported in .
Table 3. Average survival rates for metastatic melanoma.
Table 4. Annualized mortality rates.
Table 5. Average annualized mortality rates.
YLL per patient
shows the estimates of YLL per patient with metastatic melanoma for men, women, and all patients by country. Across all countries, those with metastatic melanoma are estimated to die between 18.1 years (Brazil and Mexico) and 21.3 years (Australia) prematurely.
Table 6. YLL per patient for metastatic melanoma across 12 countries, 2014.
YLL per patient also differed between the sexes: women lose more years of life from metastatic melanoma than men, which is explained by the longer natural life expectancy for women.
Note that, although there is inherently variation or uncertainty in these estimates, confidence intervals (CIs) were not part of the available data, and so 95% CIs could not be included in these results ( and , ).
Figure 1. YLL per patient due to metastatic melanoma, 2014.
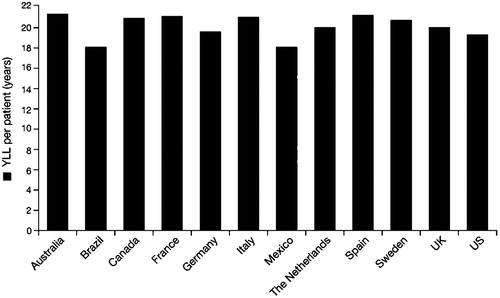
Table 7. Total YLL for metastatic melanoma across 12 countries, 2014.
Total YLL
Additionally, total YLL was calculated for each country. Estimates of total YLL in men with metastatic melanoma ranged from 13,041 in Sweden to 108,164 in Germany, and in women from 14,798 to 123,119 in the same countries. The total YLL values for the US were outliers: 468,140 for men and 540,944 for women (see ), which were mainly driven by the size of patient population.
Regional variations
The estimates of YLL varied across countries (). However, there was relatively small variations in terms of YLL at per patient level (). The variations in total YLL per country were likely due to difference in prevalence rates of metastatic melanoma and population size. Such as, a higher rate in Australia was observed and the US has a substantially larger population.
Discussion
The results show that the burden of metastatic melanoma is high; YLL per patient ranged from 18.1 (Brazil and Mexico) to 21.3 years (Australia). YLL per patient for men ranged from 16.3 (Brazil) to 19.9 years (Australia) and for women from 19.0 (Mexico) to 22.7 years (Australia). Compared to the estimates of YLL per patient due to various other cancers that have been reported in the literatureCitation26,Citation27, melanoma has one of the highest YLL per patients. YLL per patient is generally less than 15 years for breast cancer, lung cancer, colorectal cancer, and pancreatic cancerCitation27,Citation28.
Salama et al.Citation9 have recently reported a value for YLL per patient due to melanoma of 23.8 years in the 1990s in the US, compared with our US estimate for 2014 of 19.3 years, using a similar methodology. The different estimates are likely due to the positive impact of public health programs in earlier detection of melanoma, which have helped limit the progression of melanoma to advanced stages, both before detection and after treatment is initiated.
The methods for estimating YLL have some potential limitations that should be taken into account when considering the results. The distribution of age at diagnosis was based on SEER data for 2006–2010Citation25 relating to melanoma in general, and it was assumed that this age distribution was the same across all disease stages. Assuming that age and disease stage are independent is likely to cause some bias, but the direction of the bias cannot be predicted. Older patients and patients with more advanced disease are likely to be correlated; however, although more advanced disease causes greater mortality, older patients have shorter disease-free life expectancy. The study used the best data sources that were available when the study was being conducted, so the time periods covered by the data sources varied. Age distribution and survival by stage data was only available in the US and, thus, was applied to all other countries. However, no evidence exists to show substantial differences among these measures across countriesCitation7. All assumptions in this study were validated with clinical experts at several stages of the study.
The methodology and results have some strengths. Using life tables and a consistent method across 12 countries allows comparison between countries. The study provides estimates of YLL per patient and total YLL in a consistent way for many countries and, thus, contributes to a more global understanding of the burden of metastatic melanoma.
Conclusion
Measuring the burden of illness is important to policy-makers and administrators to inform decisions about resource allocation and healthcare priorities. The YLL estimates in 12 countries for 2014 show that the burden of metastatic melanoma is substantial. The significant burden of metastatic melanoma shows the need for safer and more effective treatment options for metastatic melanoma, as well as ongoing efforts to save years of life through improved public education and screening to detect melanoma in its earlier, potentially curable phases.
Transparency
Declaration of funding
This study was funded by Amgen Inc.
Declaration of financial/other relationships
AT and CQ consulted for Amgen. ZZ and BB were employed by Amgen. JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Acknowledgments
Writing assistance was provided by PRMA Consulting.
References
- Erdmann F, Lortet-Tieulent J, Schuz J, et al. International trends in the incidence of malignant melanoma 1953-2008–are recent generations at higher or lower risk? Int J Cancer 2013;132:385-400
- Arnold M, Holterhues C, Hollestein LM, et al. Trends in incidence and predictions of cutaneous melanoma across Europe up to 2015. J Eur Acad Dermatol Venereol 2014;28:1170-8
- Joshua AM. Melanoma prevention: are we doing enough? A Canadian perspective. Curr Oncol 2012;19:e462-7
- Holterhues C, Hollestein LM, Nijsten T, et al. Burden of disease due to cutaneous melanoma has increased in the Netherlands since 1991. Br J Dermatol 2013;169:389-7
- Song X, Zhao Z, Barber B, et al. Overall survival in patients with metastatic melanoma. Curr Med Res Opin 2015;31:987-91
- American Cancer Society. Melanoma skin cancer. 2014. http://www.cancer.org/cancer/skincancer-melanoma/detailedguide/melanoma-skin-cancer-key-statistics. Accessed March 1, 2015
- Ferlay J, Shin HR, Bray F, et al. GLOBOCAN 2012 v1.2, Cancer incidence and mortality worldwide: IARC CancerBase No. 10 (Internet). 2014. Lyon, France: International Agency for Research on Cancer, 2014
- Ekwueme DU, Guy Jr GP, Li C, et al. The health burden and economic costs of cutaneous melanoma mortality by race/ethnicity-United States, 2000 to 2006. J Am Acad Dermatol 2011;65:S133-43
- Salama AK, Rosa N, Scheri RP, et al. The effect of metastatic site and decade of diagnosis on the individual burden of metastatic melanoma: contemporary estimates of average years of life lost. Cancer Invest 2012;30:637-41
- Bristow BN, Casil J, Sorvillo F, et al. Melanoma-related mortality and productivity losses in the USA, 1990–2008. Melanoma Res 2013;23:331-5
- GLOBOCAN 2008: cancer incidence, mortality and prevalence worldwide in 2008. http://globocan.iarc.fr/. Accessed March 1, 2015
- Australian Bureau of Statistics (ABS). 2012. http://www.abs.gov.au/. Accessed March 1, 2015
- Destatis: Statistiches Bundesamt. 2012. https://www.destatitis.de. Accessed March 1, 2015
- Statistics Canada. Government of Canada, Government of Canada. 2013. http://www.statcan.gc.ca/. Accessed March 1, 2015
- Instituto Brasileiro de Geografiae Estatica (IBGE). 2013. http://www.ibge.gov.br/english/. Accessed March 1, 2015
- Institut national d’etudes démographiques (INED). 2011. www.ined.fr. Accessed March 1, 2015
- ISTAT: Demografia in Cifre. 2012. http://demo.istat.it/index.html.
- Statistiska centralbyran (SCB). 2012. http://www.scb.se. Accessed March 1, 2015
- Sociedad Mexicana de demografia (SOMEDE). 2010. http://www.somede.org/. Accessed March 1, 2015
- Office for National Statistics. UK National Statistics. 2012. http://www.statistics.gov.uk/hub/index.html. Accessed March 1, 2015
- Central Intelligence Agency. The World Factbook. 2014. https://www.cia.gov/library/publications/the-world-factbook/fields/2018.html. Accessed March 1, 2015
- Instituto Nacional de Estadistica. 2011. www.ine.es. Accessed March 1, 2015
- The Department of Demography at the University of California. BUaatMPIfDRiR. The Human Life-table Database. 2007. http://www.mortality.org/ Accessed March 1, 2015
- Balch CM, Buzaid AC, Soong SJ, et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol 2001;19:3635-48
- SEER Stat Fact Sheets: Melanoma of the Skin. 2011. http://seer.cancer.gov/statfacts/html/melan.html. Accessed March 1, 2015
- Shkolnikov VM. Methodology note on the human life-table database (HLD). 2014. http://www.lifetable.de/methodology.pdf. Accessed March 1, 2015
- Burnet NG, Jefferies SJ, Benson RJ, et al. Years of life lost (YLL) from cancer is an important measure of population burden – and should be considered when allocating research funds. Br J Cancer 2005;92:241-5
- Brustugun OT, Møller B and Helland Å. Years of life lost as a measure of cancer burden on a national level. Br J Cancer 2014;111:1014-20