Abstract
Depression is both clinically and biologically a heterogeneous entity Despite advances in psychopharmacology a significant proportion of depressed patients either continue to have residual symptoms or do not respond to antidepressants, It has therefore become essential to determine parameters (or predictors) that would rationalize the therapeutic choice, taking into account not only the clinical features, but also the “biological state, ” which is a major determinant in the antidepressant response. Such predictors can derive from bioclinical correlates and, in this context, the neuroendocrine strategy appears particularly suited. Numerous studies have investigated neuroendocrine parameters - derived mainly from dynamic challenge tests - in order to (i) determine the predictive profiles of good clinical responders to given anti-depressants; (ii) monitor the progression of markers in parallel with the clinical outcome; and (Hi) evaluate “in vivo” in humans the mechanisms of action of antidepressant compounds (before, during, and after treatment). This article does not attempt to be exhaustive, but rather uses selected examples to illustrate the usefulness of the investigation of the adrenal and thyroid axes and the assessment of central serotonergic, noradrenergic, and dopaminergic systems by means of neuroendocrine tests. Given methodological constraints, most of these investigations - except for baseline hormone values and the dexamethasone suppression test - cannot be used routinely in psychiatry Despite these limitations, the neuroendocrine strategy still offers new insights in biology and the treatment of depression. Its possible expansion depends mainly on the development of specific agonists or antagonists for better investigation of the receptors supposedly involved in the pathophysiology of depression. These investigations will help define more homogeneous subgroups from a bioclinical and therapeutic viewpoint.
La depresión es una entidad heterogénea tanto desde un punto de vista clínico como fisiopatológico. A pesar de los progresos de la psicofarmacología, una proporción significante de pacientes deprimidos o continúan con síntomas residuales o no responden a los antidepresivos. El poder determinar predictores que permitan racionalizar la elección de los fármacos teniendo en cuenta no solamente el estado clínico, sino también el “estado biológico” -puesto que influye en la respuesta terapéutica- parece constituir una necesidad. Tales predictores pueden ser el resultado de correlatos biológico-clínicos y es en este contexto que las estrategias neuroendocrinas se pueden aplicar de manera adecuada. El estudio de parámetros neuroendocrinos esencialmente resultados de pruebas dinámicas ha permitido (1) establecer perfiles de predicción de buena respuesta a ciertos tratamientos antidepresivos, (2) seguir la evolución de los marcadores en paralelo con la clínica y (3) estudiar los mecanismos de acción de los antidepresivos “in vivo” en el hombre (mediante estudios antes, durante y después del tratamiento). Este artículo, que no intenta ser exhaustivo, considera principalmente el interés en psiquiatría de la exploración de los ejes corticotropo y tiroideo y de los sistemas centrales serotoninérgico, noradrenérgico y dopaminérgico mediante pruebas neuroendocrinas. Mientras tanto, teniendo en cuenta las restricciones metodológicas de la mayor parte de estas investigaciones -con excepción de los niveles hormonales básales y la prueba de supresión con dexametasona- es ilusorio considerar las pruebas neuroendocrinas dentro del conjunto de los exámenes de rutina. A pesar de estas limitaciones, la estrategia neuroendocrina ofrece innegablemente nuevas posibilidades de modelos biológicos y terapéuticos en la depresión. Su expansión futura depende en gran medida del desarrollo de agonistas o antagonistas más específicos que permitan explorar de manera más precisa los diferentes receptores supuestamente implicados en la fisiopatología de la depresión. Es razonable pensar que a futuro este tipo de investigaciones permitirá delimitar subgrupos más homogéneos desde una perspectiva tanto biológico-clínica como terapéutica.
La dépression est une entité hétérogène tant d'un point de vue clinique que physiopathologique. Malgré les progrès de la psychopharmacologief environ un tiers des patients ne répondent pas au traitement antidépresseur de première intention. Déterminer des paramètres permettant de rationaliser le choix des chimiothérapies en tenant compte non seulement de l'état clinique mais aussi de «l'état biologique» - puisque celui-ci influe sur la réponse thérapeutique - apparaît par conséquent une nécessité. De tels paramètres (ou marqueurs de prédictivité) peuvent être issus de corrélats biologico-cliniques et c'est dans ce contexte que les stratégies neuroendocriniennes peuvent être appliquées de façon pertinente. De nombreuses études ont déjà permis (1) d'établir à partir de paramètres neuroendocriniens - essentiellement issus de tests dynamiques - des profils prédictifs de bonne réponse à certains traitements antidépresseurs, (2) de suivre révolution des marqueurs parallèlement à la clinique, et (3) d'étudier les mécanismes d'action «in vivo» chez l'homme d'antidépresseurs (par des études avant pendant et après traitement). Cet article, qui ne vise pas à être exhaustif, envisage principalement l'intérêt en psychiatrie de l'exploration des axes corticotrope et thyroïdien et des systèmes sérotoninergique, noradrénergique et dopaminergique centraux à l'aide de réponses hormonales à des tests spécifiques. Cependant, compte tenu des contraintes méthodologiques de la plupart de ces investigations - hormis les prélèvements basaux et le test à la dexamé-thasone - Il est illusoire d'envisager les tests neuroendocriniens dans le cadre d'examens de routine. En dépit de ces limitations, la stratégie neuroendocrinienne offre indéniablement de nouvelles possibilités de modélisation biologique et thérapeutique. Son essor futur dépend pour une grande part du développement d'agonistes ou d'antagonistes plus spécifiques afin d'explorer de manière plus précise la fonctionnalité des différents récepteurs supposés impliqués dans la physiopathologie de la dépression. Il est raisonnable de penser qu'à terme ce type d'investigations permettra de délimiter des sous-groupes plus homogènes tant sur le plan biologico-clinique que thérapeutique.
The assertion that the clinical efficacy of antide-pressants is comparable between - and within - the classesCitation1 may be true from a statistical viewpoint, but is of limited value in practice. Indeed, depression is, clinically and biologically, a heterogeneous illness and several lines of evidence suggest that the response to a pharmacological treatment depends on the patient's biological state.Citation2 Despite advances in psychopharmacology, more than one-third of patients do not respond to the drug of first choice.Citation3 Therefore, a major issue is not only to have efficacious drugs, but also to optimize their use.
During the past years, there has been Increasing Interest In the Identification of predictors of outcome in depression. However, there is little consensus regarding which clinical and biological variables influence the therapeutic response to antidepressants.Citation4,Citation5 Among the possible predictors, those derived from neuroendocrine investigations have been extensively studied. These predictors can be measured at baseline (ie, after a sufficient drugwithdrawal period) and/or during the course of treatment. It is beyond the scope of this article to detail the numerous endocrine indicators that can be used as potential biological predictors of outcome. Rather, this paper illustrates, through selected examples, the usefulness of some pertinent neuroendocrine investigations.
HPA axis
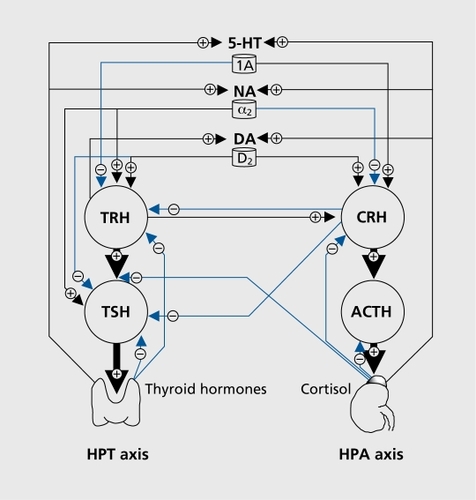
Considerable research findings have accumulated over the last four decades regarding the role of the hypothalamicpituitary-adrenal (HPA) axis in the psychobiology of depression.Citation6 Increased Cortisol secretion and failure to suppress Cortisol in response to dexamethasone, a glucocorticoid agonist, have been consistently associated with severe, melancholic, and psychotic depression.Citation7-Citation9 It has been hypothesized that this stress axis overdrive is primarily a reflection of abnormal limbic-hypothalamic activation, with increased secretion of hypothalamic corticotropin-releasing hormone (CRH) and consequent excessive adrenal Cortisol secretion. However, it remains uncertain whether the hypercortisolism is an epiphenomenon or directly contributes to depressive symptomatology and to the biochemical alterations seen in major depression ().Citation10
The dexamethasone suppression test
Although the exact pathophysiology underlying dexamethasone suppression test (DST) nonsuppression remains unclear, it has been suggested that abnormal Cortisol response reflects impaired negative feedback at the level of the pituitary corticotroph (ie, decreased type II glucocorticoid receptor function) on endogenous HPA axis hyperactivity (ie, increase in hypothalamic CRH drive that overrides the action of dexamethasone).Citation11-Citation13
However, (i) Cortisol nonsuppression following DST is not specific for the diagnosis of major depression; and (ii) the sensitivity of the DST in depression is low. Indeed, only 15% to 25% of major depressed patients are nonsuppressors, while the rate of positive DST increases in severe depression (about 40% to 70% ).Citation14 Despite these limitations, the use of DST in psychiatric research still has considerable merit. For example, serial DST monitoring of depressed patients undergoing drug treatment showed that DST gradually turned into suppression in treatment responders.Citation15,Citation16 Patients whose DST remained abnormal or who were initially suppressors, but became nonsuppressors during an observation period, had a poorer prognosis.Citation6,Citation17 In addition, over a long-term follow-up, DST suppressors at baseline have a better outcome than nonsuppressors.Citation18 Although conflicting results on the predictive value of the DST have been reported, it is generally accepted that (i) the presence of an abnormal DST indicates the need for a biological treatment, while (ii) the initial DST status has no predictive value in the choice of prescription of antidepressants.Citation19
The combined DEX/CRH test
After CRH became available for clinical studies, a more sensitive test than the DST was developed: the combined dexamethasone/corticotropin-releasing hormone test (DEX/CRH test)Citation20 in which dexamethasone-pretreated subjects receive a single dose of CRH during the afternoon of the next day. In healthy control subjects, owing to the normal inhibiting activity of the glucocorticoid receptors at the pituitary level, CRH administration induces only a small amount of corticotropin (adenocorticotropic hormone [ACTH]) and Cortisol secretion. In depressed patients, the ACTH/cortisol response to the combined DEX/CRH test is significantly increased compared with controls. This phenomenon suggests an altered glucocorticoid feedback regulation (ie, decreased glucocorticoid receptor sensitivity), possibly associated with hypothalamic CRH and vasopressin overdrive.Citation21
The combined DEX/CRH test identifies HPA axis dysfunction with high sensitivity in severe major depression (about 80% ).Citation20 Furthermore, DEX/CRH test normalization typically precedes or coincides with - rather than follows - clinical recovery, and failure to normalize portends poorly for clinical outcome.Citation22 Patients with persistent severe HPA dysregulation are more prone to relapse within 6 months than those with low Cortisol response to the DEX/CRH test at discharge.Citation23 Moreover, early improvement (after 1 or 2 weeks of therapy) and beneficial treatment outcome after 6 weeks are associated with a lower HPA system activity.Citation21
Taken together, these studies suggest that lowering HPA activity and clinical response are related. However, in a recent study, Watson et alCitation24 have found that the DEX/CRH remains abnormal in remitted bipolar patients, suggesting that HPA axis dysfunction is a potential “trait” marker in bipolar disorder.
Effects of antidepressants on the HPA axis
Recent research suggests that antidepressants could exert their clinical action in depression via the restoration of type II glucocorticoid receptor function with a subsequent reestablishment of HPA axis negative feedback.Citation25 Indeed, animal studiesCitation26 have consistently shown that antidepressants (ie, tricyclics, selective serotonin reuptake inhibitors [SSRIs], moclobemide, tianeptine) increase type II and type I (or mineralocorticoid) receptor exprèssion and function (ie, increased efficiency of signal transduction by increasing mRNA levels and hormone-binding activities). This, in turn, is associated with enhanced negative feedback by endogenous glucocorticoids, and thus with reduced HPA axis activity. Downstream consequences of lowered Cortisol secretion is a lessening of expression of genes that are under corticosteroid regulatory control, among them those related to biogenic amine neurotransmission.
Additional evidence indicates that cortisollowering treatments (ie, “antiglucocorticoids”) may be of clinical benefit in depressed patients. Indeed, open and controlled trials suggest that blockers of Cortisol synthesis (ie, metyrapone, ketoconazole, aminoglutethimide), or type II glucocorticoid receptor antagonists, including mifepristone (RU-486) and ORG 34517, may exert anti-depressant effects.Citation27 Although clinical usage of the currently available antiglucocorticoids is limited by significant side effects, the development of drugs that specifically target the glucocorticoid receptor may lead to innovative strategies in the treatment of depressive states. In the same way, development of effective CRH blockersCitation28 will provide an important tool for further study of the role of CRH hypersecretion in severe depression and other stress-related illnesses.
HPT axis
It is well established that major depression may be accompanied by a dysfunction of the hypothalamic-pituitary-thyroid (HPT) axis, including a slight elevation of serum thyroxine (T4), subnormal (or “blunted”) thyrotropin (thyroid-stimulating hormone [TSH]) response to morning injection of protirelin (thryotropin-releasing hormone [TRH]), and a loss of the nocturnal rise in TSH.Citation29 Usually, this phenomenon is not secondary to hypercortisolism.Citation30,Citation31 Investigation of the HPT axis by means of the TSH response to morning administration of TRH (at 8 am or 9 am) has limited clinical value because of modest diagnostic sensitivity (about 25 %).Citation30 Owing to the circadian activity of the thyrotroph, which is maximal between 11 pm and 1 am pituitary TSH secretion is more sensitive to TRH stimulation in the evening than in the morning, both in normal controlsCitation31,Citation36 and in depressed patients.Citation31,Citation37 In 1990, our groupCitation31 reported that the 11 pm TRH-TSH test was more sensitive than the 8 am TRH-TSH test, and that the difference in TSH response between 11 pm and 8 am TRH tests (ΔTSH) was an even more sensitive measure. Consistent with our original observation, this chronobiological index is reduced in about 80% of major depressed inpatients.Citation37-Citation39
It has been suggestedCitation30 that blunted TRH-induced TSH stimulation might reflect downregulation of the TRH receptors in the pituitary gland secondary to a prolonged increase in hypothalamic TRH stimulation. Furthermore, the shift to higher iodothyronine levels in euthyroid depressed inpatients, both in the morningCitation40 and in the evening,Citation37 may contribute to the blunting of TSH response to TRH.Citation41,Citation42
Predictive value of the TRH test
So far, studies of the therapeutic predictive value of the TSH response to TRH test have yielded conflicting results.Citation30,Citation43 Some studies have found that the normalization of the test is associated with remission, in which case the blunted TSH response - and more obviously the reduced ΔTSH values- may be considered as a “state” marker of depression.Citation38 Conversely, persistence of blunted responses during remission could represent a “vulnerability” marker to depression.
Some investigatorsCitation43 have found no link between the initial status of the TRH test and the subsequent response to a particular antidepressant treatment defined according to its biochemical mechanism of action. OthersCitation44 have found an association between the blunted TSH response and the response to desipramine (which shows a predominant “noradrenergic” action). On the other hand, it has been observed that patients with the lowest pretreatment evening TSH secretion (basal and after 11 pm TRH stimulation) have the lowest rate of antidepressant response, and this may contribute to antidepressant treatment resistance.Citation38 In such cases, it has been speculated that adjunction of thyroid hormones,Citation45 could be particularly beneficial to amplify antidepressant effects, since, by increasing the negative feedback on the hypothalamus, thyroid hormones may decrease TRH overproduction at this level.
To date, only one study has examined the relationship between morning and evening TSH and prolactin (PRL) response to TRH tests prior to antidepressant treatment and 12-month outcome.Citation46 In this study, dissociation between 11 pm TRH-induced TSH and PRL stimulation (ie, blunted TSH response associated with normal PRL response) was indicative of poor clinical outcome. Thus, normal PRL response to TRH, despite decreased TRH receptor responsiveness, might reflect a decrease in dopaminergic tone, since dopamine (DA) inhibits PRL secretion. In such patients, one may hypothesize that adjunctive therapy with DA agonists might be useful to amplify antidepressant effects.
Effects of antidepressants on the HPT axis
A number of reports suggest that treatment with antidepressant drugs leads to changes in thyroid function tests: either decreased peripheral thyroid hormone levels and/or increased TSH levels (basal or post-TRH stimulation).Citation47-Citation52 However, these results have not always been confirmed,Citation53-Citation58 owing in part to methodological limitations, eg, small sample sizes, variable definitions of depression, hospitalization status, and technical factors, such as differences in the sensitivity of the assays used in the measurement of thyroid hormones and TSH. Furthermore, it remains unclear whether changes in thyroid function are a direct effect of an antidepressant on the thyroid axis or a correlate of clinical improvement.
Animal studiesCitation58,Citation59 suggest that chronic antidepressant treatment decreases thyroid function. However, data from healthy volunteers support the notion that tricyclic antidepressants have no consistent effect on TSH secretion.Citation60,Citation61 In depressed patients, most studies have shown that antidepressant treatment with tricyclics,Citation49,Citation55,Citation61 SSRIs,Citation58 or monoamine oxidase inhibitors (MAOIs)Citation62 does not induce significant changes in TSH levels. Moreover, it has been reported,Citation45,Citation47 but not consistently,Citation63 that response to tricyclic antidepressants is associated with (i) higher pretreatment T4 levels; and (ii) decreased measures (within the normal range) of T4 and free thyroxine (FT4) without changes in triiodothyronine (T3) or TSH levels. Thus, although this is not supported by all studies, changes in thyroid function appear to be related to clinical recovery rather than to a direct effect of the antidepressant drug. This is further supported by the fact that normalization of the ΔΔTSH test is related to clinical recovery, while, irrespective of outcome, ΔΔTSH values are not significantly changed by 4 weeks of treatment with amitriptyline, fluoxetine, toloxatone, venlafaxine, or tianeptine.Citation38,Citation64
Neuroendocrine investigations of the noradrenergic system
The original catecholamine depletion hypothesis of depression has been reformulated into the “noradrenergic dysregulation hypothesis,”Citation65 which emphasizes a primary subsensitivity or downregulation in nerve terminal α2-adrenoreceptors, leading to impaired negative feedback on presynaptic neurons, which in turn may induce a disinhibition of noradrenaline (NA) output and exaggerated NA release in response to any activation of the catecholaminergic system. One of the most consistently reported abnormal findings in depression is a blunted growth hormone (GH) response to acute administration of clonidine, a partial α2-adrenoreceptor agonist. This suggests subsensitive postsynaptic α2-adrenoreceptors at the hypothalamic level. A dysregulation of the NA systern may lead to increased anxiety in depressive patients.Citation66,Citation67 More generally, blunted GH response to clonidine does not appear specific to depression, but rather to the “anxiety spectrum,” since this blunting has also been observed in generalized anxiety disorder,Citation68 panic disorder,Citation69,Citation70 and social phobia.Citation71 The link between anxiety and NA dysregulation in depressed patients is further supported by the negative correlation between GH response to clonidine and the severity of anxiety as evaluated by the Hamilton Anxiety Scale scores.Citation72
Predictive value of the clonidine test
Some studies have shown that remitted depressive patients show reduced GH responses to clonidine,Citation73,Citation74 suggesting that decreased sensitivity of α2-adrenergic receptors may represent a vulnerability marker for depression. This is further supported by the fact that, despite having differing mechanisms of action, antidepressants such as desipramine, mianserin, clorgyline, amitriptyline, and fluoxetine do not restore clonidine's effect on GH secretion in responders or nonresponders to treatment.Citation75,Citation76
It has also been argued that deficiencies in NA function could lead to differential response to noradrenaline and serotonin reuptake inhibitors.Citation77 In a study by Coote et al,Citation78 the decreased GH response before treatment was correlated with subsequent good clinical response to desipramine (a “noradrenergic” antidepressant). In a recent study, Correa et alCitation79 reported that amitriptyline, which primarily increases NA function, was more efficacious than fluoxetine in depressed patients showing at baseline blunted GH to clonidine (amitriptyline is at least 100 times more potent than fluoxetine in the inhibition of the noradrenaline transporterCitation80). Taken together, these results suggest that the NA function might influence response to antidepressant treatment.
Neuroendocrine investigations of the DA system
It is known that the mesolimbic DA system plays a key role in goal-directed and motivational behavior. In depression, it has been suggested that hypofunction in mesolimbic DA system may be involved in anhedonia and amotivational apathy.Citation81 DA agonists can facilitate the action of antidepressant drugs in certain animal models of depression and in some depressed patients.Citation82
According to the neuroendocrine challenge paradigm, hormone responses to DA agonists may provide an indirect assessment of central DA neurotransmission at the post-synaptic receptor level within the limbic-hypothalamicpituitary axis in humans.Citation83,Citation84 Apomorphine, a direct-acting DA agonist with high affinities for D2 and D3 receptorsCitation85 and a partial agonist at the Dj receptor,Citation86 decreases PRL and stimulates GH,Citation84 ACTH, and Cortisol secretion.Citation87-Citation89 In major depression, discrepant findings have been reported: unaltered responsesCitation76,Citation88-Citation90 or decreased GH responseCitation77,Citation91 to apomorphine have been found. Some of these divergences may be explained by the diversity of factors that influence the hormonal response to apomorphine, and by the heterogeneity of the populations studied. Indeed, when depressed patients are classified according to their clinical features, differences in the apomorphine response are observed between subtypes. For example, it has been found,Citation88,Citation92,Citation93 but not by all,Citation90 that apomorphine produces a lesser decrease in serum PRL levels in bipolar patients than in normals and in unipolar patients. On the other hand, unipolar patients with melancholic and psychotic features often show reduced ACTH/cortisol responses especially when hypercortisolism coexists.Citation94
From a pathophysiological viewpoint (i) blunted PRL response to apomorphine may reflect decreased D2 receptor function in the pituitary (ie, lactotrophs); and (ii) blunted ACTH/cortisol response may reflect decreased DA receptor function (ie, D2 receptor-like or T>i receptor, or both) connected with the regulation of the HPA axis at the hypothalamic level.
Predictive value of the apomorphine test
Some preclinical studies suggest that long-term antidepressants upregulate and/or hypersensitize postsynaptic DA receptors (ie, D2 and D3)Citation95 - as reflected by increased apomorphine responses in animals treated with several classes of antidepressants. However, in depressed patients, changes in DA function (ie, increased ACTH/cortisol, but not GH and PRL, responses to apomorphine) following antidepressants appear to be transient (ie, after 2 weeks' treatment, but not after 4 weeks). These changes are not correlated with clinical efficacy and are independent of the compound administered (venlafaxine, tianeptine).Citation64
On the other hand, it has been found that greater DA postsynaptic sensitivity (assessed by greater GH response to apomorphine) is associated with greater resistance to paroxetine treatment. This finding has lead to the hypothesis that pretreatment low DA receptor responsivity could predict antidepressant response to SSRIs.Citation96
Endocrine disorders
Endocrine disorders are among the factors that should be routinely searched for in the management of depressed individuals. Rare cases of endocrine disorder-related depression can be identified through the systematic measurement of some parameters, eg,TSH/FT4/FT3, PRL, cortisol/ACTH, parathyroid hormone/calcium, and glucose. Moreover, it has been well documented that endocrine disorders are factors that may contribute to treatment resistance.Citation14 The dexamethasone test is also used by endocrinologists and this test can be used routinely in psychiatry because it is simple and has decent sensitivity and predictive value in clinical evolution and response to treatment.
Conclusions
The findings reviewed in this article add further to the body of data pointing to the utility of neuroendocrine measurement in discriminating among subtypes of depressive disorders. Depression is characterized by a complex configuration of disturbances in a number of neurotransmitter and hormonal systems. Given the multiple reciprocal relationships between these systems, it is not appropriate at the present to consider one system as primary in an etiological sense.
Moreover, the biological changes that can be studied (“biological states of depression”) not only result from the pathophysiological process involved in the etiology of depression, but also from adaptive processes that maintain the homeostasis of the systems. This is why, in basal conditions, it is rare to find significant biological abnormalities in depressive states. In contrast, dynamic challenges destabilize the homeostatic balance and may therefore be used to better characterize heterogeneous biological states. Moreover, this characterization may lead to different therapeutic strategies.
According to many studies, the presence of positive (or abnormal) neuroendocrine test suggests a need for antidepressant somatic therapy of depression, but the predictive value of these tests need further clarification. Unfortunately, for methodological, ethical, and economic reasons, the neuroendocrine tests are rarely performed in battery (ie, several tests for each patient) and this limits their application from a pathophysiological and therapeutic viewpoint. For instance, in depression, the absence of chronobiological dysfunction of the thyroid axis (ie, normal ΔΔTSH) is significantly associated with decreased serotonergic function, and vice versa.Citation39 Therefore, the response to ΔΔTSH test may be of great value since a normal ΔΔTSH test could orientate the clinician towards antidepressants that increase “serotonergic” transmission; while a blunted ΔΔTSH test, which is often associated with a blunted clonidine test,Citation97 could orientate the clinician toward antidepressants that increase “noradrenergic” transmission.
The relationship between neuroendocrine test results and clinical outcome has mostly been described in retrospective study protocols. On the basis of our observations, and those of others, one may propose the following strategies, which could be the theme of prospective clinical trials of antidepressants (strategies marked with an asterisk have not yet been evaluated in depressed patients):
SSRI appear to be perfectly suitable for the first-line treatment for depression, especially when there is no evidence for chronobiological dysfunction of the thyroid axis (normal ΔTSH).
“Noradrenergic” antidepressants appear to be suitable when the GH response to clonidine is blunted and/or when there is evidence for chronobiological dysfunction of the thyroid axis (blunted ΔTSH).
“Dopaminergic” antidepressants appear to be suitable in case of normal TRH-PRL response associated with blunted TRH-TSH response (performed at 11 pm) and/or in case of blunted PRL response to apomorphine test (which is often observed in bipolar depression).*
In case of a positive DST, frequently associated with severe depression, antidepressant treatment alone will probably not suffice and therefore calls for a different approach (ie, adjunction of “antiglucocorticoids” to antidepressants, or antipsychotics, since in some melancholic/psychotic depressed patients DST is associated with blunted ACTH/cortisol response to apomorphine, reflecting a possible presynaptic DA hypersecretion at the hypothalamic level).
In case of nonresponse or partial response In patients with pretreatment 11 pm blunted TRH-TSH response, one may propose adjunctive thyroid hormone therapy.* In this Indication, T3 seems to be more efficacious than T4.Citation98 Since TSH blunting could be secondary to hyper-secretion of endogenous TRH, It may be that treatment with exogenous thyroid hormone Increases the negative feedback and, In this way, tends to correct the hypersecretion of endogenous TRH. Speculating further, the return to normal levels of TRH is perhaps part of the physiological normalization, which Is associated with resolution of a depressive episode.
Finally, It would also be Interesting to study the above strategies in conjunction with pharmacogenomic approaches.
Selected abbreviations and acronyms
| ACTH | = | adrenocorticotropic hormone |
| CRH | = | corticotropin-releasing hormone |
| DA | = | dopamine |
| DST | = | dexamethasone suppression test |
| GH | = | growth hormone |
| HPA | = | hypothalamic-pituitary-adrenal (axis) |
| HPT | = | hypothalamic-pituitary-thyroid (axis) |
| NA | = | noradrenaline |
| PRL | = | prolactin |
| SSRI | = | selective serotonin reuptake inhibitor |
| T3 | = | triiodothyronine |
| T4 | = | thyroxine |
| TRH | = | thryotropin-releasing hormone (protirelin) |
| TSH | = | thyroid-stimulating hormone (thyrotropin) |
We would like to thank the nursing staff of Sector VIII and Françoise Fleck and Gabrielle Wagner, pharmacists, for performing the hormone analyses.
REFERENCES
- American Psychiatric Association.Practice Guidelines of Patients with Major Depressive Disorder. Second Edition. Arlington, Va: American Psychiatric Association200087 p
- DelgadoP.MorenoF.Antidepressants and the brain.Int Clin Psychopharmacol.199914(suppl 1)S9S1610468323
- ThaseME.RushAJ.Treatment-resistant depression. In: Bloom FE, Kupfer DJ, eds.Psychopharmacology: the Fourth Generation of Progress. New York, NY: Raven Press.199510811097
- BrotmanAW.FalkWE.GelenbergAJ.Pharmacologic treatment of acute dépressives subtypes. In: Meltzer HY, ed.Psychopharmacology: the Third Generation of Progress. New York, NY: Raven Press.198710311040
- HirschfeldRMA.Psychosocial predictors of outcome in depression. In: Bloom FE, Kupfer DJ, eds.Psychopharmacology: the Fourth Generation of Progress. New York, NY: Raven Press.199511131121
- HatzingerM.Neuropeptides and the hypothalamic-pituitary-adrenocortical (HPA) system: review of recent research strategies in depression.World J Biol Psychiatry.2000110511112607206
- CarrollBJ.FeinbergM.GredenJF.et al.A specific laboratory test for the diagnosis of melancholia: standardisation, validation, and clinical utility.Arch Gen Psychiatry.19813815227458567
- APA Task Force On Laboratory Tests. The dexamethasone suppression test: an overview of its current status in psychiatry.Am J Psychiatry.19871412531262
- NelsonJC.DavisJM.DST studies in psychotic depression: a meta-analysis.Am J Psychiatry.1997154149715039356556
- DinanTG.Noradrenergic and serotonergic abnormalities in depression: stress-induced dysfunction?Clin Psychiatry.1996571418
- KatholRG.JaeckleRS.LopezJF.MellerWH.Pathophysiology of HPA axis abnormalities in patients with major depression: an update.Am J Psychiatry.19891463113172645793
- YoungEA.HaskettRF.GrunhausL.et al.Increased evening activation of the hypothalamic-pituitary-adrenal axis in depressed patients.Arch Gen Psychiatry.1994517017078080346
- ColeMA.KimPJ.KalmanBA.SpencerRL.Dexamethasone suppression of corticosteroid secretion: evaluation of the site of action by receptor measures and functional studies.Psychoneuroendocrinology.20002515116710674279
- DuvalF.Endocrinologie et psychiatrie.Encycl Méd Chir (Elsevier, Paris).200337-640-A-10
- GredenJF.GardnerR.KingD.GrunhausL.CarrollBJ.KronfolZ.Dexamethasone suppression tests in antidepressant treatment of melancholia.Arch Gen Psychiatry.1983404935006340634
- PeselowED.StanleyM.FilippiAM.BaroucheF.GoodnïckP.FieveR.The predictive value of the dexamethasone suppression test: a placebo-controlled study.Br J Psychiatry.19891556676722532946
- DuvalF.MokraniMC.CrocqMA.et al.Predictive bio-clinical profiles of antidepressant responses in major depression. In: Mâcher JP, Crocq MA, Nedelec JF, eds.New Prospects in psychiatry. The Bioclinical Interface. Paris, France: John Libbey Eurotext.199599109
- HolsboerF.Neuroendocrinology of mood disorders. In: Bloom FE, Kupfer DJ, eds.Psychopharmacology: the Fourth Generation of Progress. New York, NY: Raven Press.1995957969
- AnsseauM.PapartP.PïtchotW.Timsit-BerthierM.LegrosJJ.von FrenckellR.Dexamethasone suppression test and the prediction of treatment response to selective antidepressants.Eur Psychiatry.19927191194
- HeuserI.YassouridisA.HolsboerF.The combined dexamethasone/CRH test: a refined laboratory test for psychiatric disorders.J Psychiatr Res.1994283413567877114
- HatzingerM.HemmeterUM.BaumannK.BrandS.Holsboer-TrachslerE.The combined DEX-CRH test in treatment course and long-term outcome of major depression.J Psychiatr Res.20023628729712127596
- Holsboer-TrachslerE.StohlerR.HatzingerM.Repeated administration of the combined dexamethasone-human corticotropin-releasing hormone stimulation test during treatment of depression.Psychiatry Res.1991381631711661430
- ZobelAW.NickelT.SonntagA.UhrM.HolsboerF.IsingM.Cortisol response in the combined dexamethasone/CRH test as predictor of relapse in patients with remitted depression. A prospective study.J Psychiatr Res.200135839411377437
- WatsonS.GallagherP.RitchieJC.FerrierIN.YoungAH.Hypothalamicpituitary-adrenal axis function in patients with bipolar disorder.Br J Psychiatry.200418449650215172943
- BardenN.Implication of the hypothalamic-pituitary-adrenal axis in the physiopathology of depression.J Psychiatry Neurosci.20042918519315173895
- ParianteCM.ThomasSA.LovestoneS.MakoffA.KerwinRW.Do antidepressants regulate how Cortisol affects the brain?Psychoneuroendocrinology.20042942344714749091
- ReusVI.WolkowitzOM.Antiglucocorticoid drugs in the treatment of depression.Expert Opin Invest Drugs.200110178996
- KunzelHE.IsingM.ZobelAW.et al.Treatment with a CRH-1 -receptor antagonist (R121919) does not affect weight or plasma leptin concentration in patients with major depression.J Psychiatr Res.20053917317715589565
- JacksonIM.The thyroid axis and depression.Thyroid.199889519569827665
- LoosenPT.PrangeAJ.Serum thyrotropin response to thyrotropin-releasing hormone in psychiatric patients: a review.Am J Psychiatry.19821394054166802002
- DuvalF.MâcherJP.MokraniMC.Difference between evening and morning thyrotropin response to protirelin in major depressive episode.Arch Gen Psychiatry.1990474434482109971
- PatelYC.AlfordFP.BurgerHG.The 24-hour plasma thyrotropin profile.Clin Sci.19724371775040762
- WeekeA.The 24-hour pattern of serum TSH in patients with endogenous depression.Acta Psychiatr Scand.19806269747446193
- SouêtreE.SalvatïE.WehrTA.SackDA.KrebsB.DarcourtG.Twenty-four hour profile of body temperature and plasma TSH in bipolar patients during depression and during remission and in normal controls subjects.Am J Psychiatry.1988139282286
- GoichotB.BrandenbergerG.SainiJ.WïttersheimG.FoIIeniusM.Nycthemeral patterns of thyroid hormones and their relationship with thyrotropin variations and sleep structure.J Endocrinol Invest.1994171811878051340
- Perez LopezFR.LegidoA.AbosMD.LafragaL.Human pituitary chronoendocrinology: repetitive stimulation with LRH/TRH at different times of the day.Acta Endocrinol.19831023273316402871
- DuvalF.MokraniMC.CrocqMA.BaileyP.MâcherJP.Influence of thyroid hormones on morning and evening TSH response to TRH in major depression.Biol Psychiatry.1994359269348080892
- DuvalF.MokraniMC.CrocqMA.et al.Effect of antidepressant medication on morning and evening thyroid function tests during a major depressive episode.Arch Gen Psychiatry.1996538338408792760
- DuvalF.MokraniMC.BaileyP.et al.Thyroid axis activity and serotonin function in major depressive episode.Psychoneuroendocrinology.19992469571210451906
- WhybrowPC.BauerMS.Effects of peripheral thyroid hormones on the central nervous system: relevance to disorders of mood.Curr Topics Neuroendocrinol.19888309327
- CallowaySP.DolanRJ.FonagyP.De SouzaVF.WakelingA.Endocrine changes and clinical profiles in depression: II. The thyrotropin-releasing hormone testPsychol Med.1984147597656443618
- KïrkegaardC.FaberJ.Influence of free thyroid hormone levels on the TSH response to TRH in endogenous depression.Psychoneuroendocrinology.1986114914973104947
- VanelleJM.PoirierMF.BenkelfatC.et al.Diagnostic and therapeutic value of testing stimulation of thyroid-stimulating hormone by thyrotropinreleasing hormone in 100 depressed patients.Acta Psychiatr Scand.1990811561612109497
- SullivanPF.WilsonDA.MulderRT.JoycePR.The hypothalamic-pituitarythyroid axis in major depression.Acta Psychiatr Scand.1997953703789197900
- BauerM.HeinzA.WhybrowPC.Thyroid hormones, serotonin and mood: of synergy and significance in the adult brain.Mol Psychiatry.2002714015611840307
- DuvalF.MonrealJ.ValdebenitoM.MâcherJP.Chronobiological thyrotropin and prolactin responses to TRH and prognosis of depression.Eur Neuropsychopharmacol.200414(suppI)S185
- JoffeRT.RoyByrne PP.UdheTW.PostRM.Thyroid function and affective illness: a reappraisal.Biol Psychiatry.198419168516916440600
- BaumgartnerA.GràfKJ.KürtenI.MeinholdH.The hypothalamic-pituitary-thyroid axis in psychiatric patients and healthy subjects. Part II. Repeated measurements of thyroxine, free thyroxine, triiodothyronine, free triiodothyronine, and reverse triiodothyronine in patients with major depressive disorders and schizophrenia and healthy subjects.Psychiatry Res.198824283305
- WinokurA.AmsterdamJD.BerwishN.PhillipsJL.MaislinG.The relationship between the change in thyrotropin response to TRH and therapeutic response to desipramine in depressed patients.Biol Psychiatry.198925207A2649157
- JoffeRT.SingerW.Effect of tricyclic antidepressants on thyroid hormone levels in depressed patients.Pharmacopsychiatry.19902367692339180
- SteinMB.UhdeTW.Thyrotropin and prolactin responses to protirelin (TRH) prior to and during chronic imipramine treatment in patients with panic disorder.Psychoneuroendocrinology.1990153813892129312
- LoosenPT.The thyroid state of depressed patients.Clin Neuropharmacol.199215382A383A
- LeichterSB.KirsteinL.MartinND.Thyroid function and growth hormone secretion in amitriptyline-treated depression.Am J Psychiatry.197713412701272910982
- GrégoireF.BraumanH.de BruckR.CorvilaïnJ.Hormone release in depressed patients before and after recovery.Psychoneuroendocrinology.19772303312410051
- LangerG.SchoenbeckG.KônïgG.Evidence for neuroendocrine involvement in the therapeutic effects of antidepressant drugs. In: Brambilla F, Racagni G, de Wied D, eds.Progress in Psychoneuroendocrinology. New York, NY: Elsevier North Holland Biochemical Press.1980197208
- LinnoilaM.GoldP.PotterWZ.WehrTA.Tricyclic antidepressants do not alter the thyroid hormone levels in patients suffering from major affective disorder.Psychiatry Res.198143573606943598
- BrambillaF.ScaroneS.MassironiR.NobïleP.PugnettiL.Abnormal anterior pituitary responsiveness to hypothalamic hormones in primary affective disorder.Neuropsychobiology.198282692756813760
- RosenbaumJF.FavaM.PavaJA.McCarthyMK.SteingardRJ.BouffidesE.Anger attacks in unipolar depression, Part 2: Neuroendocrine correlates and changes following fluoxetine treatment.Am J Psychiatry.1993150116411688328558
- AtterwillCK.CattoLC.HealDJ.HollandCW.DickensTA.JonesCA.The effects of desipramine (DMI) and electroconvulsive shock (ECS) on the function of the hypothalamo-pituitary-thyroid axis in the rat.Psychoneuroendocrinology.1989403393462813657
- LaakmannG.BïnzA.VoderholzerU.et al.The influence of psychotropic drugs and releasing hormones on anterior pituitary hormone secretion in healthy subjects and depressed patients.Pharmacopsychiatry.19902318262179970
- LaakmanG.Neuroendocrinological findings in affective disorders after administration of antidepressants. Advances in Biological Psychiatry. Basel, Switzerland: KargerS;198056784
- JoffeRT.SingerW.Effect of phenelzine on thyroid function in depressed patients.Biol Psychiatry.198722103310343607128
- LinnoilaM.GoldP.PotterWZ.GoldPW.GoodwinFK.Tricyclic antidepressants do not alter the thyroid hormone levels in patients suffering from a major affective disorder.Psychiatry Res.198262712766955817
- DuvalF.MonrealJ.MokraniMC.CrocqMA.MâcherJP.Effect of antidepressant medication on response to TRH and apomorphine tests in depression.Biol Psychiatry.200251123S
- SieverLH.UhdeTW.New studies and perspectives on the noradrenergic receptor system in depression: effects of the α-adrenergic agonist clonidine.Biol Psychiatry.1984191311566324896
- ValdiviesoS.DuvalF.MokraniMC.et al.Growth hormone response to clonidine and the Cortisol response to dexamethasone in depressive patients.Psychiatry Res.19966023328852865
- PostRM.LakeCR.JimmersonDC.et al.Cerebrospinal fluid norepinephrine in affective illness.Am J Psychiatry.1978135907912665831
- AbelsonJL.GlitzD.CameronOG.et al.Blunted growth hormone response to clonidine in patients with generalized anxiety disorder.Arch Gen Psychiatry.1991481571621989571
- UhdeTW.SteinMB.VïttoneBJ.et al.Behavioral and physiolologic effect of short-term and long-term administration of clonidine in panic disorder.Arch Gen Psychiatry.1989461701772643934
- BrambillaF.PernaG.Garberïet al.α-Adrenergic receptor sensitivity in panic disorder: I. GH response to GHRH and clonidine stimulation in panic disorder.Psychoneuroendocrinology.199520197838898
- TancerME.SteinMB.UhdeTW.Growth hormone response to intravenous clonidine in social phobia: comparison to patients with panic disorder and healthy volunteers.Biol Psychiatry.1993345915958292687
- DuvalF.MokraniMC.MonréalJ.BaileyP.MacherJP.Serotonergic and noradrenergic function in depression: clinical correlates.Dialogues Clin Neurosci.2000229930822033550
- MitchellPB.BarnJA.CornTH.CheckleySA.Growth hormone response to clonidine after recovery in patients with endogenous depression.Br J Psychiatry.198815234383167367
- SieverLJ.TrestmanRL.CoccaroEF.et al.The growth hormone response to clonidine in acute and remitted depressed male patients.Neuropsychopharmacology.199261651771599607
- HoeheMM.ValïdoG.MatussekN.Growth hormone response to clonidine in endogenous depressive patients: evidence for a trait marker in depression. In: Shagass C, Josîassen RC, Bridger WH, Weiss KJ, Stoff D, Simpson GM, eds.Biological Psychiatry Development in Psychiatry Vol 7. Proceedings of the IV World Congress of Biological Psychiatry. Amsterdam, The Netherlands: Elsevier.1985788790
- DuvalF.MokraniMC.MonrealJ.BaileyP.HamelB.MacherJP.Effect of antidepressant treatment on alpha 2-adrenoreceptor function in depression.Biol Psychiatry.200353(suppI)188S
- AnsseauM.Von FrenckellR.MaassenD.et al.Prediction of treatment response to selective antidepressants from clonidine and apomorphine neuroendocrine challenges. In: Briley M, Fi I lion G, eds.New Concepts in Depression. London, UK: McMillan Press.1988269276
- CooteM.WilkinsA.WerstiukES.SteinerM.Effects of electroconvulsive therapy and desipramine on neuroendocrine responses to the clonidine challenge test.J Psychiatry Neurosci.1998231721789595891
- CorreaH.DuvalF.MokraniMC.et al.Noradrenergic dysfunction and antidepressant treatment response.Eur Neuropsychopharmacol.20011116316811313162
- NemeroffCB.Psychopharmacology of affective disorders in the 21st century.Biol Psychiatry.1998445175259787875
- WillnerP.Dopaminergic mechanisms in depression and mania. In: Bloom FE, Kupfer DJ, eds.Psychopharmacology: the Fourth Generation of Progress. New York, NY: Raven Press.1995921931
- CassanoP.LattanzïL.SoldaniF.et al.Pramipexole in treatment-resistant depression: an extended follow-up.Depress Anxiety.20042013113815549689
- MeltzerHY.KolakowskaT.FangVS.et al.Growth hormone and prolactin response to apomorphine in schizophrenia and the major affective disorders.Arch Gen Psychiatry.1984415125196721674
- LaiS.Apomorphine in the evaluation of dopaminergic function in man.Prog Neuropsychopharmacol Biol Psychiatry.198812117164
- SokoloffP.GirosB.MartresMP.BouthenetML.SchwartzJC.Molecular cloning and characterization of a novel dopmaine receptor (D3) as a target for neuroleptics.Nature.19903471461511975644
- CreeseI.Biochemical properties of CNS dopamine receptors. In: Meltzer HY, ed.Psychopharmacology: the Third Generation of Progress. New York, NY: Raven Press.1987257264
- JezovaD.VigasM.Apomorphine injection stimulates p-endorphin, adrenocorticorticotropin, and Cortisol release in healthy man.Psychoneuroendocrinology.198985201203
- MokraniMC.DuvalF.CrocqMA.BaileyPE.MâcherJP.Multihormonal response to apomorphine in mental illness.Psychoneuroendocrinology.1995203653758532820
- DuvalF.MokraniMC.CrocqMA.et al.Dopaminergic function and the Cortisol response to dexamethasone in psychotic depression.Prog Neuro-psychopharmacol Biol Psychiatry.2000242072253
- McPhersonH.WalshA.SilverstoneT.Growth hormone and prolactin response to apomorphine in bipolar and unipolar depression.J Affect Disord.20037612112512943941
- PitchotW.HansenneM.Gonzalez MorenoA.AnsseauM.Effect of previous antidepressant therapy on the growth hormone response to apomorphine.Neuropsychobioiogy.1995321922
- DuvalF.MokraniMC.CrocqMA.BaileyP.DiepTS.MacherJP.Dopamine function in men with bipolar depression.Biol Psychiatry.20004773S
- MonréalJA.DuvalF.MokraniMC.PinaultG.MâcherJP.Exploration de la fonction dopamïnergique dans les dépressions bipolaires et unipolaires.Ann Méd Psychol (Paris). 2005.2005163399404
- DuvalF.MokraniMC.MonrealJA.FattahS.MâcherJP.HPA and HPT axis dysfunction in depression: dopaminergic and noradrenergic correlates.Biol Psychiatry.200455(suppI)34S
- BonhommeN.EnnioE.Involvement of serotonin and dopamine in the mechanism of action of novel antidepressant drugs: a review.J Clin Psychopharmacol.1998 1 84474549864076
- HealyE.McKeonP.Dopaminergic sensitivity and prediction of antidepressant response.J Psychopharmacol.2000141521 5610890309
- DuvalF.MokraniMC.CrocqMA.BaileyP.DiepTS.MacherJP.Noradrenergic and thyroid axis dysfunction in depression.Biol Psychiatry.199639643
- SïntzelF.MallaretM.BougeraiT.Potentializing of tricyclics and serotonergics by thyroid hormones in resistant depressive disorders.Encephale.20043026727515235525