Abstract
It has been speculated that superstitiousness and obsessivecompulsive disorder (OCD) exist along a continuum. The distinction between superstitious behavior italic>and superstitious belief, however, is crucial for any theoretical account of claimed associations between superstitiousness and OCD. By demonstrating that there is a dichotomy between behavior and belief, which is experimentally testable, we can differentiate superstitious behavior from superstitious belief, or magical ideation. Different brain circuits are responsible for these two forms of superstitiousness; thus, determining which type of superstition is prominent in the symptomatology of an individual patient may inform us about the primarily affected neurocognitive systems.
Se ha especulado que la superstición y el trastorno obsesivo-compulsivo (TOC) se dan en un continuo. La distinción entre conducta supersticiosa y creencia supersticiosa; sin embargo, es crucial para cualquier tipo de teoría acerca de las asociaciones entre superstición y TOC. Existe una dicotomía entre la conducta y la creencia, que se puede demostrar experimentalmente, lo que nos permite diferenciar la conducta supersticiosa de la creencia supersticiosa o la ideación mágica. Diferentes circuitos cerebrales son responsables de estas dos formas de superstición. Conocer el tipo de superstición que predomina en la sintomatología de un paciente afectado de un TOC permite comprender mejor el papel de los principales sistemas neurocognitivos implicados en la patología.
Il est souvent proposé que la superstitiosité et le trouble obsessionnel compulsif feraient partie d' un même continuum. La distinction entre le comportement superstitieux et la croyance superstitieuse est néanmoins cruciale pour toute théorie s'intéressant aux associations entre superstitiosité et TOC. Il existe une dichotomie, démontrable expérimentalement, entre le comportement et les croyances superstitieuses, qui permet de différencier les comportements des croyances superstitieuses, et de la pensée magique. Des réseaux neuronaux distincts sont responsables de ces deux formes de superstitiosité. Ainsi, la connaissance du type de superstition dominante dans la symptomatologie d'un patient atteint de TOC pourrait permettre de mieux comprendre le rôle des principaux systèmes neurocognitifs impliqués dans cette pathologie.
According to the Merriam-Webster online dictionary (http://www.merriam-webster.com), a superstition is “a belief or practice resulting from ignorance, fear of the unknown, trust in magic or chance, or a false conception of causation.” Focusing on one or several aspects of this broad definition, some authors have suggested that superstitions are a fundamental feature of obsessive-compulsive disorder (OCD).Citation1-Citation5 We first elaborate on the dichotomy between behavior and belief, mentioned in the above definition, and differentiate superstitious behavior from superstitious belief, or magical ideation. We then propose that different brain circuits may be responsible for these two forms of superstitiousness, and that the type of superstition observed in an individual patient may thus inform investigators about the prominently affected neurocognitive systems.
Superstitious behavior
In its purest form, superstitious behavior was described in the behaviorist literature as a consequence of response-independent reinforcement. Skinner's experiments with pigeons are legendary6; the birds were offered food at random intervals and behavior incidentally displayed at times of food delivery was continuously reinforced, such that idiosyncratic behavioral stereotypies were established. Noting that the birds behaved as if they assumed a causal relation between the appearance of food and their behavior, Skinner coined the term “superstitious behavior” for this type of response-reinforcement association. This was later critity cized with statements that the inference regarding the animals beliefs about a nonexistent causality was not necessarily warranted, and attributes like “mediating” and “collateral” were suggested to describe their behavior in a more parsimonious way (see ref 7 for the literature). In fact, some of the behavioral sequences shown by human subjects in a situation of response-independent reinforcement are more reminiscent of a desperate attempt to explore the nature of the schedule of reinforcement than of any “superstitiousness” in the sense of a fixed belief. We may cite the particularly illustrative example of a healthy woman seated in a test booth with a response lever on a table in front of her and a signal light and point counter mounted on the wall.Citation8 About 5 min into the session, a point delivery occurred after she had stopped pulling the lever temporarily and had put her right hand on the lever frame. This behavior was followed by a point delivery, after which she climbed on the table and put her right hand to the counter. Just as she did so, another point was delivered. Thereafter she began to touch many things in turn, such as the signal light, the screen, a nail on the screen, and the wall. About 10 min later, a point was delivered just as she jumped to the floor, and touching was replaced by jumping. After five jumps, a point was delivered when she jumped and touched the ceiling with her slipper in her hand. Jumping to touch the ceiling was continued repeatedly and was followed by points until she stopped about 25 min into the session, perhaps because of fatigue (p 265). Unfortunately, as introspective reports have never been seriously considered in the behaviorist literature, this subject had not been explicitly asked about her thoughts and beliefs while apparently obsessed with touching and jumping.
Superstitious belief
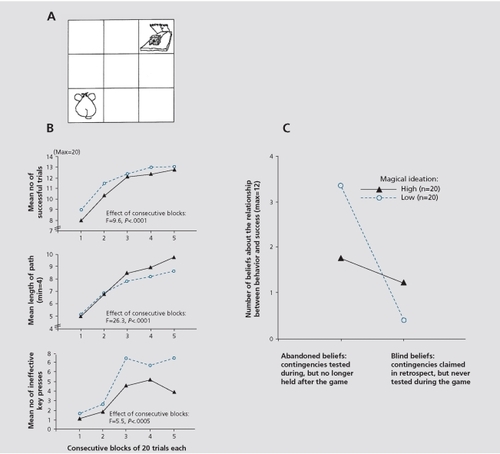
As “false conceptions of causation,” superstitious beliefs are conceptually removed from the touching and jumping behavior described above. They usually lack a direct motor manifestation. In fact, most characteristic of modern superstitious beliefs are rather abstract ideas about a paranormal causation of coincidences (telepathy, clairvoyance, precognition). These ideas are cross-culturally universal and, within a society, largely resistant to education. Designated as “magical ideation” (MI), they are a core element of positive symptoms in schizotypy,Citation9 equivalent to the delusions of reference in schizophrenia. While magical or superstitious beliefs can be conceived as the cognitive equivalents of superstitious behaviors, it is important to note that each type of superstition can occur without the other. In the pigeon, there is clear evidence, obtained from well-designed studies, for a dissociation between motor and cognitive superstitions. It was shown, for instance, that the same birds, whose pecking superstitions were based on temporal contiguity instead of contingency, were well able to distinguish between events elicited by chance and those controlled by their own behavior.Citation10 In human subjects, a similar dissociation was demonstrated when studying the relationship between superstitious behavior and superstitious belief.Citation7 In a computer game, high and low scorers on the MI scale,Citation9 an instrument designed to quantify superstitious beliefs in everyday life, displayed superstitious behavior to a comparable degree. However, the subjects believing in paranormal forms of causation were more inclined than the disbelievers to assume a causal relationship between their (irrelevant) behavior and success in the game (see for more details).
Superstitious behavior and superstitious belief in OCD
The distinction between superstitious behavior and superstitious belief is crucial for any theoretical account of claimed associations between superstitiousness and OCD. As indicated above, in healthy individuals superstitious motor behavior can occur without accompanying beliefs in nonexistent causative forces. Conversely, the formation of superstitious beliefs may take place without direct mediation by the motor system. We suggest, therefore, that different neural circuits are involved in the genesis of the two forms of superstitiousness. Specifically, we propose that the origin of superstitious rituals in OCD primarily involves the basal ganglia “habit system,”Citation11 including its connections with the (orbito)frontal cortex. Dysfunction of this neural circuitry is prominent in patients with OCD and OC-spectrum disorders. It is responsible for behavioral routines, whose stereotypy and irrationality is typically recognized by the patient. Nonetheless, recognition of the senselessness of the repetitive motor displays does not enable a patient to break the routine. Significantly, whether superstitiously motivated or not, perseveration is an almost defining feature of an obsessive-compulsive ritual ( ).Citation12

Another region of interest in connection with OCD comprises medial temporal lobe structures, in particular the hippocampus.Citation13 According to one model,Citation11,Citation12 a “limbic memory system” coordinates those subordinate brain circuits controlling inflexible habits and fixed action sequences. It states that one prominent task of the hippocampus is to enhance behavioral variability, and OCD symptoms are thought to emerge from the failure of the hippocampal complex to curb the subcortical-frontal “habit system” (see ref 14 for an alternative view of the hippocampus in OCD). In the literature on superstitious behavior and belief, the important role of the hippocampus was early recognized. Hippocampectomized rats were found to display exaggerated superstitious behaviorCitation15,Citation16 that was not simply a consequence of enhanced perseverative tendencies, but reflected the crucial role played by the hippocampus “in adapting economically to a loss of positive contingency and in averting the burden of superstition when reinforcers never bear causal relation to behavior (p 274)”. Citation16 In human clinical neuropsychology, medial temporal lobe pathology has been implicated in the emergence of superstitious beliefs. Patients suffering from temporal lobe epilepsy often show a “syndrome of sensory-limbic hyperconnection,”Citation17 which is characterized by a preoccupation with mystical, religious, and paranormal themes and an exaggerated belief in an extrasensory causation of coincidences (ref 18 for the literature). In patients with OCD who manifest marked magical ideation,Citation5 limbic dysfunction might also predominate. It remains to be determined whether these patients would represent a proper “schizotypy subtype” of OCD.Citation19
Conclusion
To conclude with a word of caution: we doubt that, over and beyond an exaggeration of normal patterns of behavior and thought, superstitions are a genuine element of OCD. However, disentangling components of superstitious motor behavior from those of superstitious beliefs may not only help the clinician, but might provide insights into the mechanisms underlying the disorder.
REFERENCES
- LeonardHLGoldbergerELRapoportJLCheslowDLSwedoSEChildhood rituals: normal development or obsessive-compulsive symptoms?J Am Acad Child Adolesc Psychiatry 199029 17232295573
- FrostROKrauseMSMacMahonMJPeppeJEvansMMcPheeAEHoldenMCompulsivity and superstitiousness Behav Res Ther 1993314234258512543
- AmirNFreshmanMRamseyBNearyEBrigidiBThought-action fusion in individuals with OCD symptomsBehav Res Ther 20013976577611419608
- EvansDWMilanakMEMedeirosBRossJLMagical beliefs and rituals in young childrenChild Psychiatry Hum Develop 2002334358
- EinsteinDAMenziesRGThe presence of magical thinking in obsessive compulsive disorderBehav Res Ther 20044253954915033500
- SkinnerBFSuperstition in the pigeonJ Exp Psychol. 19483816817218913665
- BruggerPGravesRETesting vs. believing hypotheses: magical ideation in the judgment of contingencies Cog Neuropsychiatry 19972251272
- OnoKSuperstitious behavior in humansJ Exp Analysis Behav 198747261271
- EckbladMChapmanLMagical ideation as an indicator of schizotypyJ Cons Clin Psychol 198351215225
- KilleenPRSuperstition: a matter of bias not detectabilityScience 1978199889017569494
- PitmanRKAnimal models of compulsive behaviorBiol Psychiatry 1989261891982660914
- EilamDZorRSzechtmanHHermeshHRituals, stereotypy and compulsive behavior in animals and humansNeurosci Biobehav Rev 20063045647116253329
- AtmacaMYildirimHOzdemirHet al.Hippocampus and amygdalar volumes in patients with refractory obsessive-compulsive disorderProg Neuro-Psychopharm Biol Psychiatry 20083212831286
- GrayJAMcNaughtonN2nd ed. Oxford, UK: Oxford University PressThe Neuropsychology of Anxiety: An Enquiry into the Functions of the Septo-Hippocampal System 2003
- DevenportLDSuperstitious bar-pressing in hippocampal and septal ratsScience 1979205721723462183
- DevenportLDHollowayFAThe rat's resistance to superstition: role of the hippocampusJ Comp Physiol Psychol 1980946917057190980
- BearDMTemporal lobe epilepsy - a syndrome of sensory-limbic hyperconnectionCortex 197915357384540509
- BruggerPDowdyMAGravesREFrom superstitious behavior to delusional thinking: the role of the hippocampus in misattributions of causalityMed Hyp 199443397402
- SobinCBlundellMLWeillerFGaviganCHalmanCKarayiorgouMEvidence of a schizotypy subtype in OCD. J Psychiatry Res 2000341524