
Abstract
Patient-reported outcome (PRO) refers to measures that emphasize the subjective view of patients about their health-related conditions and behaviors. Typically, PROs include self-report questionnaires and clinical interviews. Defining PROs for borderline personality disorder (BPD) is particularly challenging given the disorder's high symptomatic heterogeneity, high comorbidity with other psychiatric conditions, highly fluctuating symptoms, weak correlations between symptoms and functional outcomes, and lack of valid and reliable experimental measures to complement self-report data. Here, we provide an overview of currently used BPD outcome measures and discuss them from clinical, psychometric, experimental, and patient perspectives. In addition, we review the most promising leads to improve BPD PROs, including the DSM-5 Section III, the Recovery Approach, Ecological Momentary Assessments, and novel experimental measures of social functioning that are associated with functional and social outcomes.
El resultado percibido por el paciente (PRO) se refiere a las medidas que enfatizan la perspectiva subjetiva de los pacientes acerca de sus condiciones y conductas relacionadas con la salud. Típicamente, los PROs incluyen cuestionarios de autoreporte y entrevistas clínicas. Definir los PROs para el trastorno de personalidad borderline (TPB) es especialmente desafiante dada la alta heterogeneidad sintomática del trastorno, la elevada comorbilidad con otras condiciones psiquiátricas, los síntomas muy fluctuantes, las correlaciones débiles entre los síntomas y los resultados funcionales, y la falta de mediciones experimentales válidas y confiables para complementar los datos autoreportados. En este artículo se presenta una panorámica de las mediciones de resultados actualmente utilizadas en el TPB y se discuten desde perspectivas clínicas, psicométricas, experimentales y del paciente. Además se revisan los avances más prometedores para mejorar los PROs en el TPB, incluyendo la sección III del DSM-5, el enfoque de la recuperación, las evoluciones ecológicas momentáneas y las nuevas mediciones experimentales del funcionamiento social que se asocian con los resultados funcionales y sociales.
Les PRO (Patient reported outcomes ou résultats déclarés par les patients) sont des mesures reflétant le point de vue subjectif des patients sur leur état de santé et leurs comportements. Classiquement, les PRO contiennent des auto-questionnaires et des entretiens cliniques. Il est particulièrement difficile de définir des PRO pour le trouble de la personnalité borderline compte tenu de l'hétérogénéité élevée des symptômes dans la maladie, de la forte comorbidité avec les autres affections psychiatriques, de la grande fluctuation des symptômes, des faibles corrélations entre les symptômes et l'évolution fonctionnelle et du manque de mesures expérimentales fiables et valables pour compléter les résultats auto-déclarés. Nous présentons dans cet article une synthèse des résultats des mesures actuelles pour la personnalité borderline et les analysons sur le plan clinique, psychométrique et expérimental et du point de vue du patient. Nous examinons les avancées les plus prometteuses pour améliorer les PRO de la personnalité borderline, dont la section III du DSM-5 (Recovery Approach, Ecological Momentary Assessments), et de nouvelles mesures expérimentales du fonctionnement social associées aux résultats fonctionnels et sociaux.
Diagnostic concepts of borderline personality disorder
The modern concept of the diagnostic entity has emerged from various influences, starting from the late 19th century. As a diagnostic term, “borderline” was first mentioned by the English psychiatrist C. H. Hughes in 1884 in his article “Borderland Psychiatrists Records” for a symptom cluster that was not categorizable purely as “neurosis” or “psychosis.”
Sigmund Freud provided a description of symptoms, today seen as typical for the diagnosis of borderline personality disorder, but referred to them as a subgroup of hysteria. In 1938, the American psychoanalyst Adolf Stern described most of the symptoms that have lead to the modern diagnosis of borderline personality disorder (BPD), using the expression “borderline group of neuroses.”Citation1 It was of clinical importance because of the tendency of some patients to show “borderline” mental states of schizophrenia in unstructured situations.
“Borderline” was an inconsistent colloquialismCitation2-Citation3 until 1967, when O. F. Kernberg described Borderline Personality Organization as a level of psychological functioning.Citation4 Important features of this organization were primitive defenses like splitting, projective identification, identity diffusion, and difficulties in reality testing. He proposed psychoanalysis as the way of treating it, and saw an important etiology in abandonment and poor early parenting. This concept fits well with the personality trait research to which we will be referring below.
In contrast, R. Grinker in 1968 described borderline patients in his book The Borderline Syndrome Citation5 as a specific disorder. Within the framework of the International Pilot Study of Schizophrenia, J. G. Gunderson posited that borderline patients are distinct from schizophrenic patients and added a review “Defining Borderline Patients.”Citation3
In 1980, the borderline symptom complex entered the Diagnostic and Statistical Manual of Mental Disorders (DSM)-III as “borderline personality disorder” and has been defined consistently in the psychiatric nosology ever since. In the most, recent version of DSM (DSM-5), a diagnosis of BPD is appropriate when at least 5 of 9 criteria are present: (i) avoidance of real or imagined abandonment; (ii) alternating extremes of idealization and devaluation; (iii) identity disturbance; (iv) impulsivity in at least two areas that are potentially self-damaging; (v) recurrent suicidal behavior; (vi) affective instability; (vii) chronic feeling of emptiness; (viii) intense and inappropriate anger and difficulty controlling it; and (ix) transient paranoid ideation or dissociative symptoms.
The validity and specificity of BPD and its categorization in psychiatric classification systems is still a matter of debate. Thus far there is no generally accepted notion of how BPD fits with NIMH's Research Domain Criteria (RDoC) that is aimed at developing new ways to identify valid neurobiological data and observable behavioral dimensions across psychiatric disorders.Citation6 A number of reconceptualizations of BPD have been offered based on factors such as treatment recovery patterns, heritability, and underlying neurobiology.Citation7 In this paper we posit that BPD reflects a generalized maladaptive personality. Our focus is on how to assess the symptoms of BPD.
Patient-reported outcomes
There is growing evidence that all assessment methods have both objective and subjective components. As a consequence, we have avoided using the terms “objective” and “subjective.” Instead we constrain our language to be purely descriptive, for instance we refer to self-report measures as “questionnaires” and to measures involving standardized tasks with assessor-manipulated stimuli as “experimental.”
Table I. Examples of self-report questionnaires to assess outcomes in borderline personality disorder (BPD).
Our specific focus in this paper is on patient-reported outcomes or patient-reported outcome measures (PROs/PROMs). PRO is used to denote health data that are provided by the patient through a standardized system of reporting. The information is gathered by self-administered questionnaires completed by the patients themselves or patient interviews, emphasizing the patient's views about their feelings or what they are able to do as they are dealing with chronic diseases or conditions. Validated PRO methods can improve outcome measures by better taking into account the subjective view of patients, in addition to the more objective features of laboratory procedures or observer ratings.
The term PRO was first used in the field of oncology, where patient reports refer to self-report measures of psychosocial outcomes that were used to complement medical outcome measures such as tumor mass, laboratory exams, and other biological data. In psychiatry there is no a generally accepted definition of PRO. Nevertheless, there is consensus that PROs do not only include symptom-related measures but also functional outcomes, well-being, and quality of life.
Developing PROs to assess BPD is associated with significant challenges. For instance, PROs are designed to measure change, whereas there is a common presumption that BPD symptoms are stable. Thus PROs must be able to assess both the stable and dynamic features of BPD and related outcomes. A second challenge is that research on the structure of BPD suggests that it is multidimensional, and thus groups of individuals with that diagnosis display significant heterogeneity in symptom presentation and other features. PROs must be able to take this heterogeneity into account. Finally, some research suggests that symptom reduction as measured by PROs for BPD does not track as well with functional improvements as might be assumed, and that other features of personality provide significant information about well-being and functioning. Thus assessments are needed for both BPD symptoms as well as outcomes with which BPD may be associated.
Measuring outcomes in BPD by self-report questionnaires
Self-report measures for BPD can be divided into eight different categories, including focal assessments of BPD symptoms, multdimensional assessments of BPD/PD symptoms, multidimensional assessments of pathological traits, assessments of social functioning, assessments of distress, assessments of risky behavior, assessments of well-being, and general functioning. Scales assessing well-being, quality of life, and general functioning can be considered to be particularly close to the concept of PRO.
Regardless of instrument, the agreement between data from self-report questionnaires and from clinical interviews in BPD is generally moderate and often higher than in other personality disorders. The agreement in the Collaborative Study of Personality Disorders was r=.67 for symptom counts and kappa =.53 for categorical diagnosis.Citation27 In a meta-analysis, Samuel and WidigerCitation28 found correlations of around 0.5 between questionnaire data and interview data in BPD patients samples. This relative lack of consistency does not necessarily mean that the interview method is correct and the self-report is therefore inaccurate. For example, both self-report and interview methods are biased by the patient's acute state.Citation29 Rather, it demonstrates that the two methods reflect slightly different aspects of BPD and underlies the importance of PROs in studies of BPD.
An important limitation of current self-report assessment methods is the fact that BPD patients demonstrate poor memory regarding their extreme mood changes,Citation30 which raises questions about the validity of using retrospective questionnaires as outcome measures in BPD. Ecological Momentary Assessment (EMA) is a relatively new method that addresses this methodological problem. While participants are engaging in normal daily activity, EMA uses a series of computer-based repeated assessments of current affective, behavioral and contextual experiences and physiological processes.Citation31 While EMA is still in its infancy, real-time assessments of highly fluctuating affective and personality psychopathology have the potential to considerably improve the validity of PROs in BPD and other PDs.
“Recovery” refers to a complex outcome concept used in psychiatric rehabilitation. It does not define a specific outcome but instead emphasizes a person's potential for recovery, involving a secure sense of self, social support, empowerment, coping skills and meaning. We have shown in a pilot studyCitation32 that outcome dimensions related to the recovery approach such as personal growth, purpose of life and positive relationships with others may demonstrate important changes in patients with personality disorders from a patient perspective.
Methodological challenges of PD assessment methods
A significant challenge in the assessment of BPD involves the potential for discrepancies between the various methods available to assess such constructs.Citation33,Citation34 From a psychometric perspective, no particular tool or class of tools offers a definitive perspective on the latent construct of BPD.Citation35 Nevertheless, certain methods have come to enjoy this kind of privileged status in the literature. Researchers are particularly prone to attribute this kind of status to diagnostic interviews,Citation36 even though research has shown that interviews are no more valid than other approaches (eg, patient reports) for predicting method-neutral outcomes.Citation37
It may seem problematic when two methods designed to assess the same construct do not agree. However, this situation can also be seen as an opportunity to understand a person or construct more deeply, because test divergences may be important sources of information.Citation38 For example, although self-report questionnaires and diagnostic interviews of BPD symptoms are not differentially valid, they tend to suggest different rates of BPD symptoms and are differentially able to predict certain kinds of outcomes. These differences may be clinically important. Specifically, symptom endorsement rates tend to be higher by questionnaire than by interview, perhaps because it is easier for patients to acknowledge certain problems when they don't have to do so verbally to a person whom they do not know, or perhaps because clinicians are helpful in distinguishing symptoms from behaviors that are present but not symptomatic. Some research suggests that externally observable symptoms such as risky behavior are more valid when assessed by interviews, whereas more internal thoughts and feelings, such as emptiness, are more valid when assessed by questionnaires.Citation39 Clinicians can martial these sorts of findings to maximize predictive validity via the use of multiple methods.
Table II organizes several approaches to assessing psychological constructs and provides specific examples of each method for the assessment of BPD. This list is not meant to be exhaustive, but rather to reflect the array of approaches one could take to diagnosing this construct and its related outcomes. It should also not be presumed that each of these methods has the same level of empirical support in the research literature. Again, the point is to show the variability in approaches that could be used to assess BPD-related PROs.
Table II. Example methods for the assessment of borderline personality disorder (BDP).
Among these methods, direct verbal approaches such as diagnostic interviews and patient self-reports have been by far the most common in research and practice. Although these methods have been useful in both clinical and research settings, there is a significant negative consequence of the over-reliance on such methods in the assessment of BPD. Specifically, verbal methods, and particularly interviews, have been commonly treated as a criterion for the disorder itself. From a psychometric perspective, this practice violates a central tenet in psychometrics by confusing a latent variable (eg, BPD) for a particular measurement, approach to indicating that latent variable (eg, a score on a particular interview designed to measure BPD). To the extent that interviews provide a skewed perspective on the nature of BPD, the over-reliance on this approach as a “gold standard” skews the general understanding of the disorder. For example, well-known biases associated with both BPDCitation40 and with clinical diagnosisCitation41 likely influence the information that is gained via diagnostic interviews, whereas other approaches are less susceptible to such biases.
This emphasizes the importance of using other types of approaches to develop a more complete understanding of BPD. For example, informant report data offer one way to address issues of patient and clinician bias by getting the perspective of someone who regularly observes the patient's behavior.Citation14 EMAsCitation31 address issues related to retrospective bias because the patient reports their experiences in real time in their actual lives; this approach also provides a very rich source of information about, how pathological dynamics play out over time. NarrativeCitation42 and perceptual assessmentsCitation43 provide a less direct means of observing the inner workings of the patient's mind, and thereby perhaps offer an alternative method for circumventing biases associated with direct questioning about symptoms. Finally, there is significant potential in a number of cognitive and neuropsychological approaches that have been developed for basic research, such as basic laboratory tasks,Citation44 EEG,Citation45 or functional magnetic resonance imaging (fMRI).Citation46
Overall, the integration of multiple methods, such as those listed in Table II, would signify a more complex and complete understanding of the etiology and phenomenology of BPD. However, the agreement between most of these methods is understudied and typically poor; there is much work to be done. Understanding BPD from multiple angles is therefore likely to be a major theme of future research.
Approaches to PD assessment from quantitative trait psychology
As discussed above, a central problem in developing PROs for BPD is that its symptoms are heterogeneous, and rates of diagnostic co-occurrence are high across a range of conditions. These features of the diagnosis render it less than optimal from a clinical management standpoint because many patients have more than one diagnosis and many patients with the same diagnosis display different symptoms. The quantitative trait perspective offers the view that personality and psychopathology attributes can be arranged in a more orderly fashion than is suggested by the categorical polythetic approach of the diagnostic manuals, and that rearranging them based on an evidence -based structure of such attributes provides solutions to problems such as co-occurrence and heterogeneity.Citation47
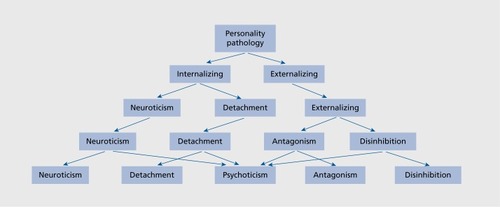
From this perspective, individual differences in personality and psychopathology can be organized in a hierarchical fashion (). Citation48,Citation49 At the top of the hierarchy is the general dysfunction that is shared by all forms of psychopathology. The next level is comprised of internalizing and externalizing dimensions, which describe a fundamental distinction in psychopathology, indicated most prominently by anxiety and mood problems (internalizing) vs conduct, antisocial, and substance use problems (externalizing).Citation50,Citation51 At the third level, internalizing tends to split into negative affectivity and detachment, so that the three traits together closely resemble Eysenck's (1967) well-known three-factor model of personality.Citation52 Within the fourth level, externalizing generally splits into antagonism and disinhibition, and thus this level closely resembles Livesley's (1998) four-factor model of pathological personality traits.Citation53 A psychoticism factor tends to emerge at the fifth level, which closely resembles the Five-Factor Model of personality trait psychology.Citation54 The hierarchy could, in principle extend downward into increasingly narrow traits, such as the 25 primary traits proposed for the DSM-5, Section III.
The DSM-5 Section III model: distinguishing symptoms from functions
Although the DSM-III/IV model of PD was retained in the official (Section II) diagnostic portion of DSM-5, Section III of the manual describes an alternative approach for PD diagnosis.Citation55 The intention seems to be for the Section III model to migrate into a position of official diagnostic status in an upcoming edition of the manual. However the form of this model has been the subject of considerable debate. As it stands, PDs will be diagnosable based on 5 sets of criteria in DSM-5 Section III. The first involves the level of personality functioning, as defined by the patient's capacity to: (i) maintain a stable, self-supportive, and coherent identity; (ii) engage in pro-social, self-directed behavior; (iii) be empathic towards others, and (iv) establish mutually satisfying intimate relationships. The second involves specific traits that underlie the disorder. Predictably, initial research has shown that these traits can be organized into a hierarchical model similar to Figure 1.Citation56 The rest of the criteria specify the stability and pervasiveness of these problems and provide rule outs.
The specific criterion A features proposed for BPD include impoverished self-image, internal emptiness, and stress-related dissociation (Identity); instability in goals and plans (Self-direction); interpersonal hypersensitivity and negatively skewed perceptions (Empathy); and unstable and conflictual relationships, preoccupation with abandonment, and vacillation between idealization and devaluation (Intimacy). To achieve the diagnosis, the patient must also exhibit significant levels of at least four pathological traits, including emotional lability, anxiousness, separation insecurity, and depressivity (from Neuroticism or Negative Affectivity in the Five Factor Model/Figure 1), impulsivity and risk taking (from Disinhibition), and hostility (from Antagonism). The criteria also stipulate that at least one of impulsivity, risk taking, or hostility must be elevated in addition to those from the Negative Affectivity domain.
Although the DSM-5 Section III model demarcates specific traits thought to be diagnostic of BPD, research tends to suggest that BPD is associated with a broader array of pathological traits at each level of the hierarchy depicted in Figure 1. For instance, Hopwood et al (2012) found correlations >.50 between BPD and the Detachment and Psychoticism domains, even though the Section III model does not allocate any of the traits from those domains to the diagnosis.Citation57 Sharp and colleagues (in review) used bi factor modeling to show that the BPD diagnosis relates primarily to what all PDs tend to have in common, rather than to a specific constellation of traits (Sharp et al, unpublished data). Patterns like this suggest that BPD essentially reflects “generalized maladaptive personality,” and are more consistent with perspectives that reserve the term borderline for a broad class of personality problems in generalCitation58 than with the descriptive psychiatric approach that treats BPD as a discrete concept, separate from other personality disorders.
Implications of the DSM-5 Section III for the future of BPD diagnosis
The A and B criteria of DSM-5 Section III represent an effort to parse trait and functional elements of PD that are confounded in DSM-IV criteria. For instance, it is well known that there is a strong correlation between BPD and neuroticism,Citation59 and it would be quite unusual to find a person with a BPD diagnosis who does not have a high standing on this trait. That being said, it would not be unusual for a person with high neuroticism to not meet the diagnostic criteria for BPD. In essence, DSM-5 Section III defines BPD as a combination of a particular personality constellation and a pattern of dysfunctional behavior, thus accounting for features of traits like neuroticism and symptoms of disorders such as BPD. This distinction improves the clinical utility of diagnosis. Criterion A symptoms determine whether the patient has pathology and the severity of that pathology, whereas Criterion B indicate the way in which that pathology is expressed. Criterion A reflects the specific behaviors that might be the targets for change, whereas Criterion B reflects the personality context underlying these behaviors. Some research suggests that these distinctions also have implications for stability, with traits being somewhat more stable than dysfunctional behaviors.Citation60 Thus, the nuance provided by the Section III model may provide a method by which clinicians can parse the relatively enduring aspects of personality that predispose problems in living, alongside the specific, contextual problems that bring patients to the clinic. This kind of nuance is consistent with the underlying principles of the PRO approach.
The International, Statistical Classification of Diseases (ICD) seems to be moving in a similar direction, albeit with a somewhat less complex system.Citation61 Although this seems to be the form that personality disorders will increasingly take in the future, the ICD-11 and DSM-5 models do not align perfectly, and there continues to be significant debate in the PD literature about the optimal way to organize this content. Future research will determine the form BPD diagnosis takes in future editions of the diagnostic manuals.
Experimental measures of BPD pathology
Theories of the pathology and the treatment of BPD usually suggest that particular basic dysfunctions build the foundation of BPD pathology. Consequently, this dysfunction must be addressed in treatment. As a prominent example, dialectical behavior therapy (DBTCitation62) suggests that BPD patients suffer from emotional dysregulation, ie, they show excessive emotional reactions to any given emotional stimulus, and return to baseline more slowly than healthy people. Such basic dysfunctions are thought to build the basis of emotion-related BPD symptoms such as emotional instability or intense feelings of abandonment. Similarly it has been speculated that BPD patients are not able to control their impulses, maybe similarly to people with frontal brain damage or ADHD, given their problems with impulsive behavior.Citation62 More cognitively based psychotherapy approaches pronounce the role of early negative relationship experiences and suggest that BPD patients show particularly negative beliefs about themselves and others, which may lead to dysfunctional emotions and reactions.Citation63,Citation64 It should be noted that we do not have reliable measures for all these complex constructs.
However, throughout the last decade an increasing number of experimental studies have been conducted to test such assumptions. Neuropsychological researchers have proposed different objective tests for this purpose. The advantage of these tests is that they are likely to tap different features of BPD than questionnaires or interview data, and thus provide incremental information about functioning. Such tests include psychophysiological assessments to assess basic emotional reactions, tests to assess (emotional) distractability and inhibition (eg, Stroop test, (emotional) Go/NoGo tests, implicit association tests), and interpretation tests, to mention only some. Early studies did indeed find evidence for different basic dysfunctions, including impulse control deficits,Citation65 stronger startle responses to neutral stimuli,Citation66 and more intense self-rated negative emotions regardless of the type of emotion (review in ref 67). However, as the methodological quality of studies improved (larger sample sizes; exclusion of patients with psychotropic medication; better matching procedures; inclusion of patient control groups in addition to healthy control groups; assessments with experimental procedures instead of self-ratings only), the picture became more complex and some hypotheses could also be rejected.
With regard to impulse control, several well-controlled studies using different types of experimental inhibition paradigms found no differences between patients with BPD and healthy people when emotionally neutral stimuli are used.Citation68,Citation69 By contrast, patients with ADHD do show impaired inhibition as compared with healthy controls and BPD subjects in experimental tasks.Citation70,Citation71 Earlier findings of impaired impulse control in BPD may be alternatively explained by comorbid ADHD,Citation72 a common comorbid disorder in people with BPD.Citation73,Citation74 Furthermore, BPD patients may display disinhibition particularly in the context of emotional stimuli Citation75,Citation76 In sum, it is emotional reactivity and not simple distractibility that is diagnostic of BPD.
With regard to emotion regulation, several studies did not find pathologically strong emotional reactions to stimuli which are not specifically related to BPD experiences such as trauma memories or childhood abuse.Citation77,Citation78 Attention to negative emotional stimuli as measured in tasks such as the emotional Stroop test, on the other hand, has been found to be stronger in BPD than in healthy people (review in ref 40). However, when patient control groups (for example depressive controls) are included, they show similar disturbances as BPD patients to general negative stimuli.Citation79,Citation80
In regard to cognitive emotional processes, BPD patients show a broader pattern of disturbances than in the other areas mentioned so far (review in ref 40). This relates, for example, to the interpretation of other people's intentions, to the experience of being excluded by others,Citation44 and to beliefs about the self, others, and the world.Citation63,Citation81,Citation82 BPD people experience others as malevolent, powerful, and rejecting, and themselves as weak, dependent, and rejected. This applies to both questionnaire findings and experimental procedures such as interpretation tests. Therefore, these type of tests might be a candidate for more experimental assessments within clinical trials. One could, for example, test whether a treatment aiming at more intense experience of interpersonal safety and attachment (eg, schema therapy) leads to a more positive interpretation of neutral movie characters (presumably via corrective relationship experiences and imagery techniques), or to stronger feelings of being included in a cyberball game.
Social decision-making
BPD patients typically show problems in relation to affect regulation, maintaining relationships Citation54 and adjusting to social norms.Citation83,Citation84 The implementation of social norms,Citation85 and the punishment of those who do not conform are crucial elements in societies.Citation86
In the last decades, novel experimental methods have been developed that allow researchers to quantify complex social behaviors related to trust, competition, and punishment. A promising paradigm that consists of economic decision theory and neurosciences, neuroeconomics has the power to objectify social interaction by using incentivized decisions from experimental economics.Citation87 Complex social emotions such as trust or fear of punishment can be put in a mathematical function to model and understand social behavior.
In a yet-unpublished study (Brändle, Preuss, Haynes, Fischbacher, Hasler), we conducted three social games, a trust game, a coordination game, and a punishment game. For the trust and the punishment game, a social and a nonsocial or control condition were applied. BPD patients, MDD patients, and healthy controls were playing with real people randomly assigned to each round. By measuring the money or punishment points transferred to the other person in the social interaction, the social preferences were assessed and analyzed. Overall, social behavior in BPD was not significantly different from healthy controls. However, we found that BPD patients were significantly more inconsistent in social decision-making over the rounds than healthy controls and depressed patients. These inconsistencies were limited to social game conditions and not found in nonsocial control experiments. Inconsistent social decision-making was associated with the experience of low social support,Citation88 particularly in the trust and the punishment game. Taken together, this type of measurement of social behavior based on game theory might be suitable to complement self-report assessments of social functioning with experimental measures. In addition, the methodology encourages researchers to use social games as diagnostic tool to improve personalization of psychotherapeutic and sociotherapeutic treatments.
Conclusions
PRO refers to health data that are provided by the patient through a system of reporting. The information is typically gathered by self-administered questionnaires completed by the patients themselves or patient interviews, emphasizing patients' views and feedback on their feelings, patients' needs, and patients' competencies as they are coping with psychiatric problems.
Defining PROs for personality disorders, particularly BPD, is subject to major challenges:
BPD is defined by heterogeneous clinical symptoms and may be best understood as generalized maladaptive personality. In addition, it shows high comorbidity with Axis I psychiatric disorders. As a result, PROs must include broad assessments of psychopathology.
Various methods available to assess personality psychopathology do not always agree well with one another. From a psychometric perspective, no particular tool or class of tools offer a privileged perspective on the latent construct. As a result, a multimodal approach is needed to provide comprehensive outcome measures for BPD.
BPD patients exhibit poor memory regarding their most extreme mood changes, raising questions about the validity of retrospective questionnaires. Novel assessment methods using a series of computer-based repeated assessments of current affective, behavioral, and contextual experiences and physiological processes during daily life may considerably improve the validity of BPD PROs.
PROs need to be able to measure both the stable and more dynamic aspects of BPD and personality-related outcomes.
Given the weak correlation between BPD symptoms and functional and social outcomes, the inclusion of general measures on functioning and quality of life are particularly important.
Specifically defined outcomes for BPD may not neatly match patient's individual treatment goals; the recovery approach is qualified to take individual outcome concepts into account.
To date, experimental measures are rarely used in clinical practice to complement outcome assessments with questionnaires, although there are promising leads to develop new assessments tools based on simple social games that relates to social and functional outcomes.
Related Research Data
REFERENCES
- SternA.Psychoanalytic investigation of and therapy in the borderline group of neuroses.Psychoanal Q.19387467489
- StoneMH.The Borderline Syndromes. New York, NY: McGraw-Hill;1980
- GundersonJ.Borderline personality disorder: ontogeny of a diagnosis.Am J Psychiatry.20091665
- KernbergO.Borderline personality organization.J Am Psychoanal Assoc.1967156416854861171
- GrinkerRR.WerbleB.DryeRC.The Borderline Syndrome: a Behavioral Study of Ego-Functions. New York, NY: Basic Books;1968
- BlairRJ.WhiteSF.MeffertH.HwangS.Disruptive behavior disorders: taking an RDoC(ish) approach.Curr Top Behav Neurosci.2013 [Epub ahead of print]
- NewAS.TriebwasserJ.CharneyDS.The case for shifting borderline personality disorder to Axis I.Biol Psychiatry.20086465365918550033
- ZanariniMC.VujanovicAA.ParachiniEA.BoulangerJL.FrankenburgFR.HennenJ.A screening measure for BPD: the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD).J Pers Disord.20031756857314744082
- ZanariniMC.Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology.J Pers Disord.20031723324212839102
- PorehAM.RawlingsD.ClaridgeG.FreemanJL.FaulknerC.SheltonC.The BPQ: a scale for the assessment of borderline personality based on DSM-IV criteria.J. Pers Disord.20062024726016776554
- CraigRJ.VerinisJS.WexlerS.Personality characteristics of drug addicts and alcoholics on the Millon Clinical Multiaxial Inventory.J Pers Assess.1985491561603998985
- MoreyLC.LanierVW.Operating characteristics of six response distortion indicators for the personality assessment inventory.Assessment.199852032149728028
- MelleyAH.OltmannsTF.TurkheimerE.The Schedule for Nonadaptive and Adaptive Personality (SNAP): temporal stability and predictive validity of the diagnostic scales.Assessment.2002918118712066833
- MarkonKE.QuiltyLC.BagbyRM.KruegerRF.The development and psychometric properties of an informant-report form of the personality inventory for DSM-5 (PID-5).Assessment.20132037038323612961
- Mullins-SweattSN.EdmundsonM.Sauer-ZavalaS.LynamDR.MillerJD.WidigerTA.Five-factor measure of borderline personality traits.J Pers Assess.20129447548722489634
- WeissmanMM.BothwellS.Assessment of social adjustment by patient self-report.Arch Gen Psychiatry.19763311111115962494
- WeissmanMM.PaykelES.SiegelR.KlermanGL.The social role performance of depressed women: Comparisons with a normal group.Am J Orthopsychiatry.1971413904054929647
- AldenLE.WigginsJS.PincusAL.Construction of circumplex scales for the Inventory of Interpersonal Problems.J. Pers Assess.1990555215362280321
- RizzoR.PiccinelliM.MazziMA.BellantuonoC.TansellaM.The Personal Health Questionnaire: a new screening instrument for detection of ICD-10 depressive disorders in primary care.Psychol Med.20003083184011037091
- BeckAT.EpsteinN.BrownG.SteerRA.An inventory for measuring clinical anxiety: psychometric properties.J Consult Clin Psychol.1988568938973204199
- PilkonisPA.ChoiSW.ReiseSP.StoverAM.RileyWT.CellaD.Item banks for measuring emotional distress from the Patient-Reported Outcomes Measurement Information System (PROMIS(R)): depression, anxiety, and anger.Assessment.20111826328321697139
- SansoneRA.WiedermanMW.SansoneLA.The Self-Harm Inventory (SHI): development of a scale for identifying self-destructive behaviors and borderline personality disorder.J Clin Psychol.1998549739839811134
- WhitesideSP.LynamDR.Understanding the role of impulsivity and externalizing psychopathology in alcohol abuse: application of the UPPS impulsive behavior scale.Exp Clin Psychopharmacol.20031121021712940500
- NewcombeDA.HumeniukRE.AliR.Validation of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): report of results from the Australian site.Drug Alcohol Rev.20052421722616096125
- FrischMB.Quality of life therapy and assessment in health care.Clinical Psychology: Science and Practice.199851940
- DerogatisLR.The psychosocial adjustment to illness scale (PAIS).J Psychosom Res.19863077913701670
- HopwoodCJ.NewmanDA.DonnellanMB.et alThe stability of personality traits in individuals with borderline personality disorder.J Abnorm Psychol.200911880681519899850
- SamuelDB.WidigerTA.A meta-analytic review of the relationships between the five-factor model and DSM-IV-TR personality disorders: a facet level analysis.Clin Psychol Rev.2008281326134218708274
- ZimmermanM.Diagnosing personality disorders. A review of issues and research methods.Arch Gen Psychiatry.1994512252458122959
- SolhanMB.TrullTJ.JahngS.WoodPK.Clinical assessment of affective instability: comparing EMA indices, questionnaire reports, and retrospective recall.Psychol Assess.20092142543619719353
- SantangeloP.BohusM.Ebner-PriemerUW.Ecological momentary assessment in borderline personality disorder: a review of recent findings and methodological challenges.J Pers Disord.2012 [Epub ahead of print].
- HaslerG.MoergeliH.SchnyderU.Outcome of psychiatric treatment: what is relevant for our patients?Compr Psychiatry.20044519920515124150
- DavidsonKM.ObonsawinMC.SeilsM.PatienceL.Patient and clinician agreement on Personality using the SWAP-200.J Pers Disord. 2003/06/01200317208218
- SamuelDB.WidigerTA.Comparing personality disorder models: cross-method assessment of the FFM and DSM-IV-TR.J Pers Disord.20102472174521158596
- LoevingerJ.Objective tests as instruments of psychological theory.Psychol Rep.19573635694
- JacobsbergL.PerryS.FrancesA.Diagnostic agreement between the SCID-II screening questionnaire and the personality disorder examination.J Pers Assess.1995654284338609583
- HopwoodCJ.MoreyLC.EdelenMO.et alA comparison of interview and self-report methods for the assessment of borderline personality disorder criteria.Psychol Assess.200820818518315403
- BornsteinRF.Toward a process-focused model of test score validity: Improving psychological assessment in science and practice.Psychol Assess.20112353254421668126
- VazireS.Who knows what about a person? The self-other knowledge asymmetry (SOKA) model.J Pers Soc Psychol.20109828130020085401
- BaerRA.PetersJR.Eisenlohr-MoulTA.GeigerPJ.SauerSE.Emotion-related cognitive processes in borderline personality disorder: A review of the empirical literature.Clin Psychol Rev.20123235936922561966
- LilienfeldSO.Can psychology become a science?Pers Individ Dif.201049281288
- HibbardS.PorcerelliJ.KamooR.SchwartzM.AbellS.Defense and object relational maturity on Thematic Apperception Test scales indicate levels of personality organization.J Pers Assess.20109224125320408024
- MihuraJL.MeyerGJ.DumitrascuN.BombelG.The validity of individual Rorschach variables: systematic reviews and meta-analyses of the comprehensive system.Psychol Bull.201313954860522925137
- StaeblerK.RennebergB.StopsackM.FiedlerP.WeilerM.RoepkeS.Facial emotional expression in reaction to social exclusion in borderline personality disorder.Psychol Med.2011411929193821306661
- HegerlU.SteinM.MulertC.et alEEG-vigilance differences between patients with borderline personality disorder, patients with obsessive-compulsive disorder and healthy controls.Eur Arch Psychiatry Neurol Sci.2008258137143
- HerpertzSC.DietrichTM.WenningB.et alEvidence of abnormal amygdala functioning in borderline personality disorder: a functional MRI study.Biol Psychiatry. 8/15/200150292298
- KruegerRF.MarkonKE.Reinterpreting comorbidity: a model-based approach to understanding and classifying psychopathology.Annu Rev Clin Psychol.2006211113317716066
- MarkonKE.KruegerRF.WatsonD.Delineating the structure of normal and abnormal personality: an integrative hierarchical approach.J Pers Soc Psychol.20058813915715631580
- WrightAGC.ThomasKM.HopwoodCJ.MarkonKE.PincusAL.KruegerRF.The hierarchical structure of DSM-5 pathological personality traits.J Abnorm Psychol.201212195195722448740
- AchenbachTM.The classification of children's psychiatric symptoms: a factor-analytic study.Psychol Monogr.1966801375968338
- KruegerRF.The structure of common mental disorders.Arch Gen Psychiatry.19995692192610530634
- EysenckHJ.The Biological Basis of Personality. Springfield, IL: Thomas;1967
- LivesleyW.JangKL.VernonPA.Phenotypic and genetic structure of traits delineating personality disorder.Arch Gen Psychiatry.1998559419489783566
- WidigerTA.TrullTJ.Plate tectonics in the classification of personality disorder: shifting to a dimensional model.Am Psychol.200762718317324033
- American Psychiatric Association.Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing;2013
- WrightAGC.ThomasKM.HopwoodCJ.MarkonKE.PincusAL.KruegerRF.The hierarchical structure of DSM-5 pathological personality traits.J Abnorm Psychol.201212195195722448740
- HopwoodCJ.ThomasKM.MarkonKE.WrightAGC.KruegerRF.DSM5 personality traits and DSM-IV personality disorders.J Abnorm Psychol.201212142443222250660
- KernbergOF.Severe Personality Disorders: Psychotherapeutic Strategies. New Haven, CT: Yale University Press;1984
- SamuelDB.WidigerTA.A meta-analytic review of the relationships between the five-factor model and DSM-IV-TR personality disorders: a facet level analysis.Clin Psychol Rev.2008281326134218708274
- HopwoodCJ.MoreyLC.DonnellanMB.et alTen-year rank-order stability of personality traits and disorders in a clinical sample.J Personal.201381335344
- TyrerP.CrawfordM.MulderR.et alThe rationale for the reclassification of personality disorder in the 11th revision of the International Classification of Diseases (ICD-11).Personal Ment Health.20115246259
- LinehanM.Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York, NY: Guilford Press;1993
- ArntzA.DreessenL.SchoutenE.WeertmanA.Beliefs in personality disorders: a test with the Personality Disorder Belief Questionnaire.Behav Res Ther.2004421215122515350860
- ButlerAC.BrownGK.BeckAT.GrishamJR.Assessment of dysfunctional beliefs in borderline personality disorder.Behav Res Ther.2002401231124012375731
- BerlinHA.RollsET.IversenSD.Borderline personality disorder, impulsivity, and the orbitofrontal cortex.Am J Psychiatry.20051622360237316330602
- Ebner-PriemerUW.BadeckS.BeckmannC.et alAffective dysregulation and dissociative experience in female patients with borderline personality disorder: a startle response study.J Psychiatr Res.200539859215504426
- RosenthalMZ.GratzKL.KossonDS.CheavensJS.LejuezC.LynchTR.Borderline personality disorder and emotional responding: A review of the research literature.Clin Psychol Rev.200828759117544188
- JacobGA.GutzL.BaderK.LiebK.TuscherO.StahlC.Impulsivity in borderline personality disorder: impairment in self-report measures, but not behavioral inhibition.Psychopathology.20104318018820375540
- VölkerKA.SpitzerC.LimbergA.GrabeH-J.FreybergerHJ.BarnowS.Executive dysfunctions in female patients with borderline personality disorder with regard to impulsiveness and depression.Psychother Psychosom Med Psychol.20095926427218600611
- LampeK.KonradK.KroenerS.FastK.KunertH.HerpertzS.Neuropsychological and behavioural disinhibition in adult ADHD compared to borderline personality disorder.Psychol Med.2007371717173017506923
- NiggJT.SilkKR.StavroG.MillerT.Disinhibition and borderline personality disorder.Dev Psychopathol.2005171129114916613434
- SebastianA.JacobG.LiebK.TüscherO.Impulsivity in borderline personality disorder: a matter of disturbed impulse control or a facet of emotional dysregulation?Curr Psychiatry Rep.20131518
- FossatiA.NovellaL.DonatiD.DoniniM.MaffeiC.History of childhood attention deficit/hyperactivity disorder symptoms and borderline personality disorder: a controlled study.Comp Psychiatry.200243369377
- PhilipsenA.LimbergerMF.LiebK.et alAttention-deficit hyperactivity disorder as a potentially aggravating factor in borderline personality disorder.Br J Psychiatry.200819211812318245028
- JacobGA.ZvonikK.KamphausenS.et alEmotional modulation of impulse control In women with borderline personality disorder—a functional MRI study.J Psychiatry Neurosci.20133816417223046830
- SilbersweigD.ClarkinJ.GoldsteinM.et alFailure of frontolimbic inhibitory function in the context of negative emotion in borderline personality disorder.Am J Psychiatry.20071641832184118056238
- JacobGA.HellstemK.OwerN.et alEmotional reactions to standardized stimuli in women with borderline personality disorder: stronger negative affect, but no differences in reactivity.J Nerv Ment Dis.200919780881519996718
- KuoJR.LinehanMM.Disentangling emotion processes in borderline personality disorder: physiological and self-reported assessment of biological vulnerability, baseline intensity, and reactivity to emotionally evocative stimuli.J Abn Psychol.2009118531
- ArntzA.AppelsC.SieswerdaS.Hypervigilance in borderline disorder: a test with the emotional Stroop paradigm.J Pers Disord.20001436637311204344
- von Ceumern-LindenstjernaI-A.BrunnerR.ParzerP.MundtC.FiedlerP.ReschF.Initial orienting to emotional faces in female adolescents with borderline personality disorder.Psychopathology.201043798720068378
- BeckAT.ButlerAC.BrownGK.DahlsgaardKK.NewmanCF.BeckJS.Dysfunctional beliefs discriminate personality disorders.Behav Res Ther.2001391213122511579990
- BharSS.BrownGK.BeckAT.Dysfunctional beliefs and psychopathology in borderline personality disorder.J Pers Disord.20082216517718419236
- SeresI.UnokaZ.KeriS.The broken trust and cooperation in borderline personality disorder.Neuroreport.20092038839219218873
- King-CasasB.SharpC.Lomax-BreamL.LohrenzT.FonagyP.MontaguePR.The rupture and repair of cooperation in borderline personality disorder.Science.200832180681018687957
- FehrE.FischbacherU.Third-party punishment and social norms.Evolution Hum Behav.2004256387
- SpitzerM.FischbacherU.HerrnbergerB.GronG.FehrE.The neural signature of social norm compliance.Neuron.20075618519617920024
- HaslerG.Can the neuroeconomics revolution revolutionize psychiatry?Neurosci Biobehav Rev.201236647821550365
- FydrichT.SommerG.TydecksS.BrählerE.Fragebogen zur sozialen Unterstützung (F-SozU): Normierung der Kurzform (K-14)Social Support Questionnaire (F-SozU): Standardization of short form (K-14).Z Med Psychol.2009184348