
Abstract
The Hierarchical Taxonomy of Psychopathology (HiTOP) is an empirical structural model of psychological symptoms formulated to improve the reliability and validity of clinical assessment. Neurobiology can inform assessments of early risk and intervention strategies, and the HiTOP model has greater potential to interface with neurobiological measures than traditional categorical diagnoses given its enhanced reliability. However, one complication is that observed biological correlates of clinical symptoms can reflect various factors, ranging from dispositional risk to consequences of psychopathology. In this paper, we argue that the HiTOP model provides an optimized framework for conducting research on the biological correlates of psychopathology from an ontogenetic perspective that distinguishes among indicators of liability, current symptoms, and consequences of illness. Through this approach, neurobiological research can contribute more effectively to identifying individuals at high dispositional risk, indexing treatment-related gains, and monitoring the consequences of mental illness, consistent with the aims of the HiTOP framework.
La taxonomía jerárquica de la psicopatología (TJP) es un modelo estructural empírico de síntomas psicológicos propuesto para mejorar la confiabilidad y la validez de la evaluación clínica. La neurobiología puede dar cuenta de las evaluaciones de riesgo precoz y estrategias de intervención, y el modelo de TJP tiene un mayor potencial para interactuar con las mediciones neurobiológicas que los diagnósticos categoriales tradicionales dada su mayor confiabilidad. Sin embargo, una complicación es que los correlatos biológicos observados de los síntomas clínicos pueden reflejar varios factores, que van desde el riesgo de la disposición hasta las consecuencias de la psicopatología. En este artículo, se argumenta que el modelo TJP proporciona un marco optimizado para realizar investigaciones sobre los correlatos biológicos de la psicopatología desde una perspectiva ontogenética que distingue entre indicadores de responsabilidad, síntomas actuales y consecuencias de la enfermedad. A través de este enfoque, la investigación neurobiológica puede contribuir de manera más efectiva con la identificación de individuos con un alto riesgo de disposición, el registro de los beneficios del tratamiento y el monitoreo de las consecuencias de la enfermedad mental, de acuerdo con los objetivos del marco de referencia de la TJP.
La taxonomie hiérarchique de la psychopathologie (HiTOP, Hierarchical Taxonomy of Psychopathology) est un modèle empirique et structuré de symptômes psychologiques visant à améliorer la fiabilité et la validité de l’évaluation clinique. L’évaluation sur le risque précoce et les stratégies thérapeutiques peuvent bénéficier des apports de la neurobiologie ; le modèle HiTOP interagit mieux avec les mesures neurobiologiques que les diagnostics catégoriels classiques, en raison de sa plus grande fiabilité. Néanmoins, le fait que les corrélats biologiques observés des symptômes cliniques peuvent refléter différents facteurs qui vont du risque lié à la prédisposition aux conséquences de la pathologie, complique les choses. Dans cet article, nous soutenons que le cadre du modèle HiTOP est optimal pour la recherche sur les corrélats biologiques de la psychopathologie d’un point de vue ontogénétique qui distingue les indicateurs de responsabilité, les symptômes actuels et les conséquences de la maladie. Par cette approche, la recherche neurobiologique permet de mieux identifier les personnes à risque de prédisposition élevé, de mieux répertorier les bénéfices liés au traitement et de surveiller les conséquences de la maladie mentale, selon les objectifs du cadre de l’HiTOP.
Introduction
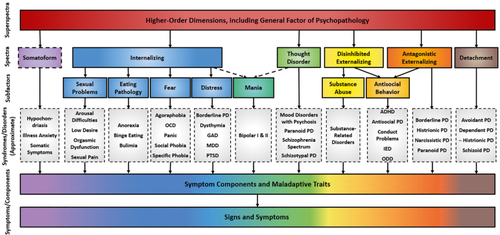
The Hierarchical Taxonomy of Psychopathology (HiTOP Citation1,Citation2 ) was advanced to characterize the empirical structure of psychopathology and overcome the myriad problems inherent in consensus-based nosologies such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) . Citation3 The HiTOP model, which is derived from factor-analytic studies of symptoms, diagnoses, and maladaptive trait data, describes a hierarchy of continuous dimensions accounting for broader spectra and super-spectra as well as narrower, symptom-level manifestations of psychopathology ( Figure 1 ). For example, the Internalizing spectrum encompasses narrower subfactors including Fear and Distress, which, in turn, encompass even more specific clinical phenotypes (eg, social anxiety, insomnia). One particular strength of the HiTOP framework is that continuous symptom dimensions exhibit higher reliabilities than categorical diagnoses, Citation4 laying the foundation for more valid measurement of psychopathology. Citation1,Citation5 Other strengths include the capacity of a dimensional approach to accommodate the heterogeneity of diagnostic conditions and their systematic co-occurrence. For example, high rates of comorbidity between DSM -defined generalized anxiety disorder and major depressive disorder—themselves highly heterogeneous syndromes—are likely to reflect cognitive, behavioral, and neurobiological commonalities between the two. Within HiTOP, these shared features are reflected in the Distress subfactor, with traits and symptoms specific to one or the other syndrome represented at lower levels of the hierarchy. Each level is conceptualized as a continuous dimension from minimal to extreme severity, rather than coded as absence versus presence of that feature. This structure facilitates the linkage of both broader and more specific HiTOP dimensions, identified through self-, peer, and clinician report, to variation observed in other measurement modalities (eg, functional neuroimaging) as a way to better understand psychobiological systems contributing to both transdiagnostic and condition-specific aspects of psychopathology. Citation6 In this respect, the HiTOP approach is consistent with the National Institute of Mental Health’s Research Domain Criteria (RDoC) initiative. Citation7
HiTOP’s emphasis on transdiagnostic common factors contrasts with the recent Addictions Neuroclinical Assessment (ANA Citation8,Citation9 ) framework, which attempts to use neurobiology to address heterogeneity within a single phenomenon (ie, addiction), failing to consider that many neural indicators may operate transdiagnostically. The hierarchical structure of HiTOP provides a framework for more systematically investigating common and specific etiological processes in psychopathology using neurobiological methods and measures. Citation6
Improved measurement of manifest symptomatology, as represented in the HiTOP framework, provides an unprecedented opportunity to elucidate the ontogeny of mental illness—the developmental-experiential processes that, over time, give rise to psychopathology and its consequences. Citation10 A deeper, developmentally informed understanding of the mechanisms and processes that contribute to the range of known psychological problems would contribute directly and importantly to prevention and intervention efforts, Citation11 consistent with calls by psychiatrists for transdiagnostic “staging models” of psychopathology. Citation12 The goal of the present paper is to describe an ontogenetic framework for continuing research on the emergence, progression, and persistence of psychopathology in the context of the HiTOP framework. In doing so, we argue for the utility of neural systems variables alongside experiential and behavioral descriptions in characterizing these pathways. Citation6,Citation13,Citation14
Importantly, however, we also highlight distinctions in the role neurobiology is expected to play at different points in the ontogeny of psychopathology. For example, neural indicators of latent liability for psychopathology need to be distinguished from those reflecting symptoms and consequences of clinical illness. The ANA and similar initiatives do not specifically address this critical point, and it remains unclear what aspects of substance addiction are indexed by variables they identify as relevant neural indicators. This muddled picture is likely to impede the development of effective interventions. Differences among latent liability, current symptomatology, and consequences of psychopathology warrant strong consideration in the search for biological indicators of mental illness.
The HiTOP framework, too, can benefit from a formalized ontogenetic model of psychopathology. The current focus of HiTOP is on the most clinically salient point of this progression—ie, current manifest symptomatology. However, it cannot be assumed—indeed, it seems unlikely—that biological correlates of manifest symptom dimensions represented at various levels of the HiTOP hierarchy will necessarily reflect etiological mechanisms contributing to these dimensions. The HiTOP model is descriptive, providing important information about the empirical structure of psychopathology and points of observed co- occurrence versus distinctiveness of symptoms, with major implications for nosological refinement. Building upon the model as it stands, the ontogenetic synthesis presented here is intended to more clearly explicate the temporal and etiological aspects of psychopathology. From this perspective, a systematic, developmentally oriented program of research is needed to characterize the nature of biological processes that are relevant to various stages in the progression from latent liability to active psychopathology and its consequences.
The basic form of the proposed ontogenetic framework for psychopathology is depicted in Figure 2 . Each element of the framework is discussed in further detail below with reference to the running example of substance problems, as well as other syndromes where space allows. Briefly, the model defines liability factors as premorbid, transdiagnostic individual-difference characteristics conducive to psychopathology. These risk factors are presumed to reflect genetically influenced neural and cognitive processes, as well as early childhood experiences such as maltreatment or fetal alcohol exposure, that create a context for the operation of experiential influences on psychological processes and behavior. Citation15 The delineation of dispositional characteristics that prospectively predict psychopathology can help to identify individuals in greatest need of preventive efforts and those likely to be most amenable to particular treatments.
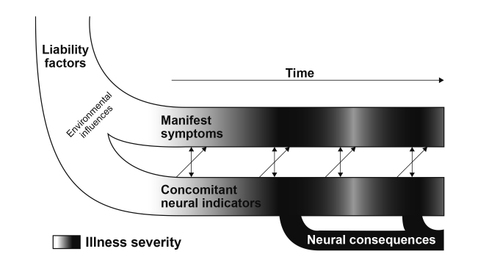
The second part of the model depicted in Figure 2 consists of current symptomatology—that is, the presence of thoughts, feelings, and behaviors that are associated with some degree of distress and/or impairment, and the neural indicators that covary with them over time. (While distress and impairment criteria are ubiquitous in current nosological frameworks of mental illness, discussion is ongoing about the exact manner in which distress and impairment are modeled within HiTOP. Citation16 ) Within the ontogenetic model, current symptoms are conceptualized as products of the complex interplay of liabilities and experience in promoting a particular manifestation of psychopathology. This stage of the ontogenetic progression corresponds to the symptom dimensions represented in HiTOP, which vary continuously in severity—rather than dichotomously as presence versus absence of particular features. In contrast with the relative stability of liability factors, current symptomatology and its associated neural indicators are expected to fluctuate over time, and thus can be used to monitor therapy-related improvements.
Finally, consequences of psychopathology encompass the lasting psychological and neurobiological alterations that are caused by mental illness and persist despite fluctuations in symptom expression. Of particular interest in this ontogenetic model are the structural and functional neural abnormalities caused by episodes of mental illness, consistent with a “scar model.” Citation17 “Scarring” differs from current symptomatology in that it is maintained regardless of improvement in symptoms. Consequences of psychopathology play an important role in the ontogenetic pathway because they can be used to monitor the progression of a syndrome in terms of persisting effects on the brain and behavior.
Liability and its neural indicators
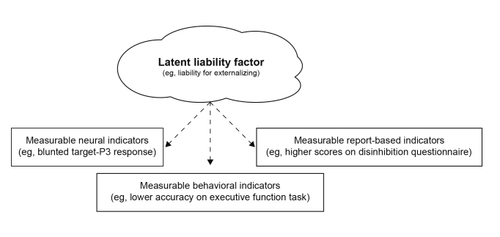
Within the ontogenetic framework, liability factors can be defined as genetically influenced dispositions, susceptible to early environmental modulation, that are associated with risk for psychopathology prior to the onset of illness. The identification of liability factors is a crucial research priority, as they serve as the basis for investigating how distal, heritable dispositions intersect with and contribute to more proximal pathogenic processes to give rise to manifest psychopathology. Citation18 Further, research on latent liability factors and their manifestations across particular measurement modalities (eg, specific patterns of neural response; Figure 3 ) can allow for the identification of individuals most likely to exhibit later psychopathology, so they can be prioritized for prevention programs. Knowledge of an individual’s constellation of liability factors could also be used to predict the efficacy of particular intervention approaches and thereby guide treatment planning.
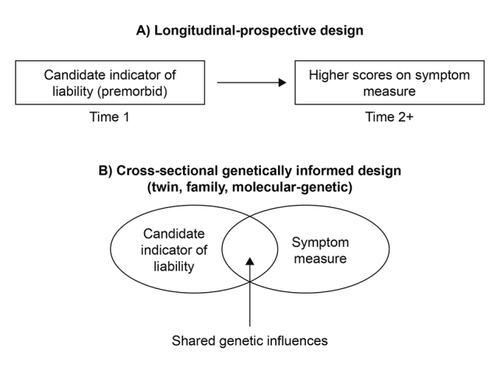
Different strategies can be used to identify indicators of liability and establish their prognostic efficacy ( Figure 4 ). The first and most crucial is to conduct longitudinal studies of young people exhibiting a candidate liability indicator to determine whether it prospectively predicts the emergence of the expected form of psychopathology. For example, longitudinal studies have identified indicators that are informative about the future likelihood of developing substance problems (SPs) and the probable course of such problems. Of note, although initially aimed at specific SPs such as alcohol or cocaine use disorder, numerous studies over the past several decades suggest that the most robust indicators of SP liability reflect risk for externalizing problems more broadly. Citation19-Citation21 The implication is that these indicators operate at higher levels of the HiTOP system (ie, the Disinhibited Externalizing spectrum or Externalizing super-spectrum.) (Although not visually depicted in the original HiTOP model [ Figure 1 ], the Externalizing super-spectrum is conceptualized as encompassing the Disinhibited Externalizing and Antagonistic Externalizing spectra). HiTOP-aligned research can facilitate efficient discovery of such principles by attending to multiple levels of the hierarchy simultaneously, rather than requiring decades of research on clinical groups segregated by diagnosis to reach the same conclusion.
One example of a well-established neural indicator of liability for SPs and other externalizing conditions is the target-P3 event-related potential (ERP), a brain response elicited by infrequently occurring task stimuli requiring a response. The P3 is thought to reflect cognitive processing following stimulus events, Citation19 and it covaries positively with task measures of executive function. Citation20 Research beginning in the 1980s found blunted amplitude of the target-P3 ERP response to be consistently linked to SPs, Citation22-Citation24 with later research extending this finding to individuals with externalizing problems of other types. Citation19,Citation25-Citation27 Blunted target-P3 was also observed in clinically unaffected relatives of individuals with externalizing problems, such as children of parents with SPs, Citation28-Citation30 and twin studies revealed a substantial contribution of genetic influences to target-P3 amplitude ( Figure 5 ). Citation31 Building on these findings, Iacono and colleagues Citation28 demonstrated that blunted target-P3 in adolescence predicted subsequent development of SPs and other externalizing problems in adulthood. The prospective nature of this association, together with evidence for familial aggregation, suggests that blunted target-P3 response, as a reflection of diminished cognitive processing of task- relevant stimuli, may constitute an indicator of liability for externalizing psychopathology ( Figure 4 ).
Another key approach to evaluating candidate liability indicators is to quantify genetic influences on an indicator variable’s association with psychopathology using multivariate causal modeling in twin studies. A substantial genetic contribution to the observed covariance between a putative liability indicator and an outcome measure of psychopathology implicates the presence of a common genetic predisposition in both. In conjunction with longitudinal research showing that the indicator predates and prospectively predicts symptomatology, twin study analyses demonstrating common genetic influences provide compelling evidence that the variable in question operates as an indicator of liability to that form of psychopathology ( Figure 4 ). Citation32 As an example, Hicks and colleagues Citation33 used twin modeling to demonstrate that the association between blunted target-P3 amplitude and externalizing symptomatology was attributable entirely to genetic influences in common between the two ( Figure 5 ). In sum, blunted target-P3 amplitude appears to be evident prior to the onset of externalizing psychopathology and shares heritable variance with externalizing problems. Citation33 (Of note, target-P3 and other executive function-related liability indicators are unlikely to be innately determined, but rather represent a product of genetic and environmental influences that give rise to a characteristically disinhibited cognitive- motivational style. Citation15 ) These features suggest that blunted target-P3 response can be considered an indicator of liability for externalizing psychopathology ( Figure 4 ).
Given that known liability factors tend to operate in a multifinal manner—increasing risk for a variety of psychopathologies Citation11 —future research should establish whether liability factors as described here relate mainly to higher-order HiTOP dimensions, or in some cases relate selectively to a more specific form of psychopathology. For example, neuroimaging studies suggest that differentiable structural and functional correlates are observed at general versus more specific levels of the hierarchy, Citation34,Citation35 but it is not yet known whether these correlates function as liability indicators. Similar to Barlow’s triple vulnerability model, Citation36 which posits that increasingly specific liabilities guide the expression of anxiety, transdiagnostic liabilities operating at higher levels of HiTOP (eg, the Externalizing super- spectrum) could be supplemented by more specific risk factors to produce particular signs and symptoms at the lower levels (eg, SPs).
Indexing liability using measures from different modalities: the psychoneurometric approach
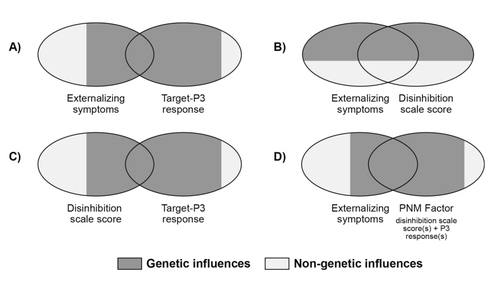
One promising approach to improving the quantification of liability factors is to combine measures of a liability construct from different response modalities (eg, self- or other report, neural reactivity, task performance; Figure 3 ) into a multi-method “psychoneurometric” composite. Citation6,Citation37,Citation38 For example, liability for externalizing problems can be operationalized by combining scores on one or more questionnaire measures of disinhibition (ie, assessing tendencies to act in impulsive-irresponsible ways) with one or more variants of P3 brain response. Citation38 This approach to quantifying externalizing liability is advantageous compared with a purely questionnaire-based measure because twin research demonstrates that a larger portion of the composite’s predictive association with externalizing problems can be attributed to shared genetic variance. Citation32 The reason is that the variance in common between scale-assessed disinhibition and externalizing problems reflects overlap in terms of environmental as well as genetic influences, whereas the variance in common between P3 brain response and externalizing problems reflects mainly overlapping genetic influences Citation33,Citation39 ( Figure 5 ). Prospective-longitudinal research could be undertaken to confirm that dispositional characteristics quantified in this manner predate manifest symptomatology and persist through remission and relapse, as would be expected of liability factors ( Figure 4 ).
The role of the environment
The progression from latent liability to manifest psychopathology depends importantly on environmental influences. For example, genetic predispositions appear to exert greater influence on SPs among adolescents who associate with alcohol-using peer groups, Citation40 an example of gene x environment interaction. In other words, the contribution of liability tends to be amplified in a developmental context that is conducive to psychopathological expression. Moreover, an individual’s level of exposure to adverse environments can be predicted by genetic liability factors, a phenomenon known as gene-environment correlation. For example, individuals exhibiting weak inhibitory control—a heritable liability factor—appear more likely to self-select environments that lead to easier drug access, such as deviant peer groups. Citation41 Moreover, upon initiating substance use, an individual’s overestimation of their peers’ drug use predicts cognitive and physiological changes associated with a worse trajectory. Citation42,Citation43 Overall, the cascading associations between liability and environment promote the emergence of psychopathology.
Current symptomatology and concomitant neural indicators
Neural indicators of liability, as described above, predate the emergence of clinical symptoms and are likely to remain stable over the course of the illness. In contrast, as psychopathology first arises and fluctuates in severity over time, other neurobiological indicators are likely to follow a temporal course that parallels symptom changes. Such concomitant indicators are part and parcel of the psychopathology itself (ie, disease-related dysfunction), as they accompany the presence of and changes in subjective experience and observed behavior patterns. Importantly, HiTOP-aligned symptom dimensions allow for the precise delineation of longitudinal relations between self- or other-rated symptoms and neural features, in ways that traditional diagnostic categories cannot. Small changes in expression of HiTOP dimensions over time, regardless of their proximity to arbitrary DSM diagnostic thresholds, could be linked to modest within-person changes in neural response, whereas studies using diagnostic categories would offer far less precision in identifying such associations. An example of a concomitant process pertaining to SPs is incentive sensitization, Citation44 wherein stimuli that become associated with substance-related reward over time (eg, a hypodermic needle) acquire potency as motivational cues (ie, become objects of “wanting”) separate from the hedonic impact of the substance itself (“liking,” eg, high of heroin). Citation45 This process is thought to contribute to the maintenance of SPs and proneness to relapse following cessation of use. Citation44
Incentive sensitization to psychoactive substances can be considered a concomitant indicator of SPs because it appears to (i) develop alongside SPs; and (ii) vary longitudinally with SP symptom severity. Evidence for these points comes from ERP research demonstrating variability in the neural responses to substance-related cues among individuals with varying severity of SPs, as well as longitudinal changes in these responses within SP-diagnosed individuals who experience recovery. One robust electrocortical indicator of incentive sensitization is the alcohol cue reactivity P3 response (ACR-P3 Citation46-Citation48 ), which is evoked by alcohol-related cues in the context of a larger visual categorization task. The ACR-P3 appears to capture incentive valuation (ie, degree of “wanting”) of alcohol and is greater in heavier-drinking individuals. Citation46 Other ERP indicators of incentive sensitization appear to covary with the longitudinal course of SPs. For example, in one study of individuals treated for cocaine use disorder, increases from pre- to post-treatment in the late positive potential response to pleasant non-drug-related images were found to be associated with decreased craving of cocaine following treatment. Citation49
Taken together, these findings suggest that neural indicators of incentive sensitization may covary with the severity of SPs, both across individuals and within the same subjects over time. Importantly, unlike a liability factor, incentive sensitization cannot occur in substance-naïve individuals, instead developing concomitantly with the emergence of SPs. One benefit of identifying such indicators is that they can then be utilized as measures of within-subject change in psychopathology, including treatment-related improvements. Incorporating regular assessment of these indicators into treatment Citation37,Citation50 could be particularly helpful for syndromes characterized by low insight into one’s own symptoms, such as SPs, as a supplement to report-based measures and behavioral tasks (eg, the drug-choice paradigm, in which subjects decide between viewing substance-related and -unrelated images Citation51 ). Knowledge of concomitant neural indicators could also facilitate the development of novel interventions, such as neurofeedback training, that hold promise for ameliorating certain forms of psychopathology. Citation50
Neural indicators that change concomitantly with symptomatology can also shed light on the prospective course of psychopathology, perhaps because of their presumed proximity to an underlying neural mechanism. (Note that it is critical not to conflate observed differences between patient and healthy control groups on some neural measure with discovery of a mechanism underlying that form of psychopathology, given: [i] the abovementioned limitations of diagnostic-group research that HiTOP was designed to address, as well as [ii] the impossibility of making mechanistic inferences from cross-sectional, ontogeny-agnostic studies, particularly when relevant experimental work has not been performed.) For example, once an individual has accumulated experience with alcohol, ACR-P3 amplitude appears to prospectively predict increased engagement in heavy drinking Citation46 ; this association may reflect the mechanistic role of incentive sensitization in the transition from repeated alcohol use to alcohol dependence. Whereas neural indicators of liability are clinically useful for identifying individuals at increased risk for psychopathology prior to symptom onset, concomitant neural indicators may have distinct utility for predicting future course among those already experiencing psychopathology.
Complicating matters further, liability and concomitant processes likely interact, such that mechanisms promoting symptom maintenance and exacerbation are enhanced by dispositional risk factors. One example from the neuroimaging literature is that, as incentive sensitization increases, a growing imbalance between incentive reward and executive control brain networks seems to lead to increasingly compulsive drug-related urges. Citation52 Although executive control network activation in part reflects externalizing-related liability, its interaction with other brain systems in the context of emerging incentive sensitization promotes further development of substance-related psychopathology. This type of interplay is important to consider in studies seeking to identify neurobiological indicators of psychopathology risk and expression.
Consequences of psychopathology
The final component of this ontogenetic framework consists of the lasting consequences of psychopathology, including neurobiological measures indicative of dysfunction caused by illness. In contrast to the concomitant indicators described above, neural indicators that do not abate with the remission of psychological symptoms are consistent with a “scar” resulting from the experience of mental illness. Citation17 Some of the most apparent consequences of psychopathology are medical, such as liver failure resulting from chronic alcohol overuse, or esophageal damage following frequent purging behaviors in eating pathology. However, psychopathology can also have lasting impacts on many psychological domains, from cognitive ability and personality to sensorimotor adaptations, and these effects are likely mediated by biological changes. Neural consequences of psychopathology play an important role in the ontogenetic pathway because they can be used to monitor the progression of an illness in terms of lasting effects on the brain, in the same way that medical tests can be used to quantify the progression of liver failure.
As discussed for liability factors, one critical tool for establishing a given neural indicator as a consequence of psychopathology is longitudinal research. In contrast to liability indicators, which must be present prior to the onset of psychopathology and persist over the course of illness, and concomitant neural indicators, which must be present alongside clinical symptoms, scarring becomes apparent only following symptom onset and must persist in the face of changes in clinical presentation. Studies examining such a progression are exceedingly rare, and none to our knowledge have used HiTOP-aligned symptom-dimension designs. In the psychosis field, research has suggested that individuals diagnosed with schizophrenia may experience greater brain tissue loss per year (-0.5%) than healthy controls (-0.2%), with inconsistent links between symptom fluctuations and the rate of neural degeneration. Citation53,Citation54 However, these gray matter alterations may also be present in high-risk premorbid individuals, Citation55,Citation56 suggesting they are not solely a consequence of the experience of psychosis. The advent of large-scale longitudinal studies that include functional and/or structural neural data will be of enormous utility in the search for indicators of neural scarring, as premorbid brain data will be available for those who go on to develop psychopathology.
In addition to longitudinal studies, co-twin control analyses provide another means for evaluating whether an individual difference characteristic reflects liability for versus consequences of psychopathology. This approach involves comparing twins with differing levels of symptomatology on a characteristic of interest, controlling for genetic and shared environmental influences. Evidence from co-twin control studies suggests that central nervous system hyperarousal and resultant negative affectivity—as well as alterations in electrocortical dynamics related to response inhibition—occur as consequences of alcohol use, and that alcohol, cannabis, and tobacco use contribute causally to reduced ventral striatum functional connectivity. Citation57,Citation58 Each of these indicators is strongly linked to externalizing psychopathology, but they are also implicated in other syndromes; in contrast, as described above, gray matter decrements appear relatively unique to psychosis. It remains to be seen which neural indicators reflect scarring effects at differing levels of specificity within the HiTOP hierarchy.
Research on other spectra and future directions
Various report-, performance-, and physiology-based measures have been shown to relate to diverse forms of psychopathology, but it remains unclear whether the constructs assessed by such measures represent stable pre- existing liability factors, correlates of current psychopathology, or lasting consequences of illness. Ongoing work on the ontogeny of mental illness will require comprehensive, multimodal assessment as well as longitudinal studies with genetically informative samples (eg, twins and/or individuals providing genomic data). Citation37
The topics discussed here are not unique to SPs, nor to the Externalizing super-spectrum. Neural indicators of liability have been described in relation to numerous other forms of psychopathology. For example, the reward positivity (“RewP”) brain-ERP response shows a consistent negative association with major depression and prospectively predicts increases in depressive symptomatology. Citation59,Citation60 Importantly, this brain-response measure appears to index proneness to depression rather than neural dysfunction associated with current depressive symptomatology. Citation61 Bolstering the case for liability status, reduced RewP response is present in unaffected family members of depressed individuals Citation62 and is observed even in preschool-aged depressed children. Citation63,Citation64 The RewP is also beginning to be examined in relation to other forms of psychopathology involving reward system dysfunction, including SPs. Citation65 Beyond the RewP, numerous studies demonstrate that neurobiological indicators, including other ERP measures, can be used to index liability for a range of psychopathology, including—but not limited to—SPs. A limitation of work to date is that relatively few studies have utilized dimensional symptom measures, and none to our knowledge have explicitly examined higher-order spectra of psychopathology in relation to ERPs, apart from the externalizing-P3 literature described above. HiTOP provides an optimal platform for testing research questions of this kind. For example, the notion that neural indicators of liability might operate primarily at higher-order levels of the HiTOP model represents an important topic for future investigation.
In contrast to the growing literature on neural indicators of liability, relatively little dimensional work has been undertaken to distinguish these from neurobiological indicators of current symptoms or lasting consequences for any of the HiTOP dimensions. Much more extensive longitudinal and dimensional work is needed to better understand the latter two elements of the ontogenetic pathway, with the goal of predicting the future course of clinical problems and monitoring disease- and treatment-related change using neural measures. Citation37,Citation50,Citation66
Beyond the individual model elements we have emphasized (liability, current symptomatology, consequences) and our specific focus on neurobiological indicators, the ontogenetic framework proposed here is not unique to the SP literature, nor to explicitly HiTOP-aligned research: It complements and extends existing ontogenetic models of externalizing, bipolar, and thought disorders. Citation67-Citation69 For example, McGorry et al Citation69 proposed a “clinical staging” model of psychosis, mania, and depression wherein signs and symptoms largely overlapped at the earliest stages but became increasingly distinct during the progression to acute, severe symptomatology. In parallel, our model posits that factors driving symptom expression at early stages should not be studied in isolation (eg, mania versus control group), but rather in line with a hierarchical understanding of mental illness at the HiTOP spectrum or super-spectrum level. For purposes of early identification and intervention, time is better spent understanding liability processes contributing to the generation of disordered cognitive and behavioral patterns shared across syndromes (ie, at higher levels of HiTOP), rather than in any subgroup alone. Conversely, symptom expression at the last stage of McGorry’s model Citation69 is highly differentiated and would likely operate at the symptoms/components level of HiTOP, potentially driving consequences specific to psychotic symptom expression and not mania, or vice versa. Here, neural indicators of current symptomatology and, perhaps, lasting consequences would be expected to show specificity to a particular syndrome. As illustrated by the parallels with McGorry’s model, Citation69 as well as with models of other forms of psychopathology, Citation67,Citation68 the HiTOP framework and this ontogenetic perspective can be applied to myriad psychopathological conditions.
Conclusion
The ontogenetic model we have described provides a framework for organizing existing knowledge and guiding continued research on the etiology, mechanisms, and consequences of mental illness as represented in the HiTOP model. In particular, we have emphasized how neurobiological measures can aid in this endeavor and the ways in which HiTOP provides an ideal platform for ontogenetic research, given its reliable, clearly organized, and structurally valid symptom dimensions. With a greater knowledge of the distinct liability factors, concomitant indicators, and lasting consequences associated with particular symptom dimensions, mental health professionals will be better equipped to identify and intervene with at-risk individuals and monitor the progressive remediation and lasting consequences of their psychopathology.
This work was supported by National Institute of Mental Health grants F31MH122096 (ERP) and T32MH93311-08 (ERP); a Ford Foundation Predoctoral Fellowship administered by the National Academies of Sciences, Engineering, and Medicine (KJJ); US Army grant W911NF-14-1-0018 (CJP); DFG Heisenberg Professorship 389624707 (UR); and Province of Ontario Ministry of Research and Innovation Early Researcher Award ER14-10-185 (ACR). ACR is also a University of Toronto Scarborough Research Excellence Faculty Scholar. The content of this paper is solely the responsibility of the authors and does not necessarily reflect the official views of the US Government, National Institutes of Health, Department of Defense, Department of the Army, Department of Veterans Affairs, or US Recruiting Command. Funding sources had no role in the study design, in the collection, analysis, and interpretation of data, in the writing of the report, or in the decision to submit the article for publication. ACR has received consulting fees from System Analytic; the other authors have no financial disclosures or competing interests. ERP, KJJ, and CJP contributed to the initial composition of the manuscript. All other authors contributed to revision of the manuscript, adding important intellectual content; members of the HiTOP Neurobiology Workgroup are listed by contribution (RDL to UR) and subsequently in alphabetical order (MHA to DHZ). The authors wish to thank two anonymous reviewers and Nancy J. Reed, MD, for their helpful input on earlier drafts of the manuscript
REFERENCES
- KotovRKruegerRFWatsonDet alThe hierarchical taxonomy of psychopathology (HiTOP): a dimensional alternative to traditional nosologiesJ Abnorm Psychol201712645447728333488
- KruegerRFKotovRWatsonDet alProgress in achieving quantitative classification of psychopathologyWorld Psychiatry201817328229330229571
- American Psychiatric Association (APA)Diagnostic and Statistical Manual of Mental Disorders20135th ed.Washington, DCAmerican Psychiatric Association Publishing
- ChmielewskiMClarkLABagbyRMWatsonDMethod matters: understanding diagnostic reliability in DSM-IV and DSM-5J Abnorm Psychol201512476476926098046
- MarkonKEChmielewskiMMillerCJThe reliability and validity of discrete and continuous measures of psychopathology: a quantitative reviewPsychol Bull201113785687921574681
- PerkinsERLatzmanRDPatrickCJInterfacing neural constructs with the Hierarchical Taxonomy of Psychopathology: ‘why’ and ‘how’Personal Ment Health202014110612231456351
- InselTCuthbertBGarveyMet alResearch domain criteria (RDoC): toward a new classification framework for research on mental disordersAm J Psychiatry2010167774875120595427
- KwakoLEMomenanRLittenRZKoobGFGoldmanDAddictions neuroclinical assessment: a neuroscience-based framework for addictive disordersBiol Psychiatry20168017918926772405
- KwakoLEMomenanRGrodinENLittenRZKoobGFGoldmanDAddictions neuroclinical assessment: a reverse translational approachNeuropharmacology201712225426428283392
- PatrickCJHajcakGRDoC: translating promise into progressPsychophysiology20165341542426877135
- CicchettiDRogoschFAEquifinality and multifinality in developmental psychopathologyDev Psychopathol19968597600
- McGorryPNelsonBWhy we need a transdiagnostic staging approach to emerging psychopathology, early diagnosis, and treatmentJAMA Psychiatry201673319119226765254
- DepueRAIaconoWGNeurobehavioral aspects of affective disordersAnnu Rev Psychol1989404574922648983
- EysenckHJThe Biological Basis of Psychopathology1967 Springfield, IL Charles C. Thomas
- NiggJTCaseyBJAn integrative theory of attention-deficit/hyperactivity disorder based on the cognitive and affective neurosciencesDev Psychopathol20051778580616262992
- BornsteinRFFrom structure to process: on the integration of AMPD and HiTOPJ Pers Assess2019101436036630358430
- ClarkLATemperament as a unifying basis for personality and psychopathologyJ Abnorm Psychol2005114450552116351374
- Buchman-SchmittJMBrislinSJVenables NCJoinerTEPatrickCJTrait liabilities and specific promotive processes in psychopathology: the example of suicidal behaviorJ Affect Disord201721610010827726889
- PatrickCJBernatEMMaloneSMIaconoWGKruegerRFMcGueMP300 amplitude as an indicator of externalizing in adolescent malesPsychophysiology200643849216629688
- VenablesNCFoellJYanceyJRKaneMJEngleRWPatrickCJQuantifying inhibitory control as externalizing proneness: a cross-domain modelClin Psychol Sci20186561580
- YoungSEFriedmanNPMiyakeAet alBehavioral disinhibition: liability for externalizing spectrum disorders and its genetic and environmental relation to response inhibition across adolescenceJ Abnorm Psychol200911811713019222319
- AnokhinAPVedeniapinABSirevaagEJet alThe P300 brain potential is reduced in smokersPsychopharmacology200014940941310867969
- BigginsCAMacKaySClarkWFeinGEvent-related potential evidence for frontal cortex effects of chronic cocaine dependenceBiol Psychiatry1997424724859285083
- BrancheyMHBuydens-BrancheyLHorvathTBEvent-related potentials in substance-abusing individuals after long-term abstinenceAm J Addict19932141148
- BauerLOHesselbrockVMP300 decrements in teenagers with conduct problems: implications for substance abuse risk and brain developmentBiol Psychiatry199946226327210418702
- CostaLBauerLKupermanSet alFrontal P300 decrements, alcohol dependence, and antisocial personality disorderBiol Psychiatry200047121064107110862806
- KimMSKimJJKwonJSFrontal P300 decrement and executive dysfunction in adolescents with conduct problemsChild Psychiatry Hum Dev20013229310611758881
- IaconoWGCarlsonSRMaloneSMMcGueMP3 event-related potential amplitude and the risk for disinhibitory disorders in adolescent boysJAMA Psychiatry200259750757
- BegleiterHPorjeszBBihariBKissinBEvent-related brain potentials in boys at risk for alcoholismScience19842254669149314966474187
- HillSYSteinhauerSRAssessment of prepubertal and postpubertal boys and girls at risk for developing alcoholism with P300 from a visual discrimination taskJ Stud Alcohol1993543503588487544
- KatsanisJIaconoWGMcGueMKCarlsonSRP300 event-related potential heritability in monozygotic and dizygotic twinsPsychophysiology19973447589009808
- VenablesNCHicksBMYanceyJRet alEvidence of a prominent genetic basis for associations between psychoneurometric traits and common mental disordersInt J Psychophysiol201711541227671504
- HicksBMBernatEMaloneSMet alGenes mediate the association between P3 amplitude and externalizing disordersPsychophysiology20064498105
- KaczkurkinANMooreTMCalkinsMEet alCommon and dissociable regional cerebral blood flow differences associate with dimensions of psychopathology across categorical diagnosesMol Psychiatry201823101981198928924181
- SnyderHRHankinBLSandmanCAHead KDavisEDistinct patterns of reduced prefrontal and limbic gray matter volume in childhood general and internalizing psychopathologyClin Psychol Sci2017561001101329399423
- BarlowDHUnraveling the mysteries of anxiety and its disorders from the perspective of emotion theoryAm Psychol2000551247126311280938
- PatrickCJIaconoWGVenablesNCIncorporating neurophysiological measures into clinical assessments: fundamental challenges and a strategy for addressing themPsychol Assess2019
- PatrickCJVenablesNCYanceyJRHicksBMNelsonLDKramerMDA construct-network approach to bridging diagnostic and physiological domains: application to assessment of externalizing psychopathologyJ Abnorm Psychol201312290291624016026
- YanceyJRVenablesNCHicksBMPatrickCJEvidence for a heritable brain basis to deviance-promoting deficits in self-controlJ Crim Justice201341309317
- DickDMPaganJLVikenRet alChanging environmental influences on substance use across developmentTwin Res Hum Genet20071031532617564520
- BurtASMcGueMIaconoWGNonshared environmental mediation of the association between deviant peer affiliation and adolescent externalizing behaviors over time: results from a cross-lagged monozygotic twin differences designDev Psychol2009451752176019899929
- BorsariBCareyKBPeer influences on college drinking: a review of the researchJ Subst Abuse20011339142411775073
- ClappJDMcDonnellALThe relationship of perceptions of alcohol promotion and peer drinking norms to alcohol problems reported by college studentsJ Coll Stud Dev2000411926
- RobinsonTEBerridgeKCThe neural basis of drug craving: an incentive-sensitization theory of addictionBrain Res Rev1993182472918401595
- BerridgeKCRobinsonTELiking, wanting, and the incentive-sensitization theory of addictionAm Psychol201671867067927977239
- BartholowBDHenryEALustSAEffects of alcohol sensitivity on P3 event-related potential reactivity to alcohol cuesPsychol Addict Behav20072155556318072838
- BartholowBDLustSATragesserSLSpecificity of P3 event-related potential reactivity to alcohol cues in individuals low in alcohol sensitivityPsychol Addict Behav20102422022820565148
- MartinsJSBartholowBDCooperMLIrvinKMPiaseckiTMInteractive effects of naturalistic drinking context and alcohol sensitivity on neural alcohol cue-reactivity responsesAlcohol Clin Exp Res20194381777178931233217
- ParvazMAMoellerSJMalakerPSinhaRAlia-KleinNGoldsteinRZAbstinence reverses EEG-indexed attention bias between drug-related and pleasant stimuli in cocaine-addicted individualsJ Psychiatry Neurosci2017422788628245173
- HajcakGKlawohnJMeyerAThe utility of event-related potentials in clinical psychologyAnnu Rev Clin Psychol201915719531067414
- MoellerSJBeebe-WangNWoicikPAKonovaABMaloneyTGoldsteinRZChoice to view cocaine images predicts concurrent and prospective drug use in cocaine addictionDrug Alcohol Depend2013130117818523218913
- KarolyHCHarlaarNHutchisonKESubstance use disorders: a theory-driven approach to the integration of genetics and neuroimagingAnn NY Acad Sci20131282719123470155
- Hulshoff PolHEKahnRSWhat happens after the first episode? a review of progressive brain changes in chronically ill patients with schizophreniaSchizophr Bull200834235436618283048
- VitaADe PeriLDesteGSacchettiEProgressive loss of cortical gray matter in schizophrenia: a meta-analysis and meta-regression of longitudinal MRI findingsTransl Psychiatry20122e19023168990
- BhojrajTSSweeneyJAPrasadKMet alGray matter loss in young relatives at risk for schizophrenia: Relation with prodromal psychopathologyNeuroImage201154S272S27920441795
- KeshavanMSDevelopment, disease and degeneration in schizophrenia: A unitary pathophysiological modelJ Psychiatr Res19993351352110628528
- BurwellSJDoes substance use during youth cause lasting changes in resting-state neurophysiology and brain functional connectivity? a co-twin control investigation [dissertation]2017 Minneapolis, MN University of Minnesota Digital Conservancy Available at: http://hdl.handle.net/11299/191390
- HarperJMaloneSMIaconoWGImpact of alcohol use on EEG dynamics of response inhibition: a cotwin control analysisAddict Biol20182325626727859998
- Hajcak ProudfitGThe reward positivity: from basic research on reward to a biomarker for depressionPsychophysiology20155244945925327938
- NelsonBDPerlmanGKleinDNKotovRHajcakGBlunted neural response to rewards as a prospective predictor of the development of depression in adolescent girlsAm J Psychiatry2016173121223123027363510
- BowyerCBJoynerKJYanceyJRVenablesNCHajcakGPatrickCJToward a neurobehavioral trait conceptualization of depression pronenessPsychophysiology2019
- WeinbergALiuHHajcakGShankmanSABlunted neural response to rewards as a vulnerability factor for depression: results from a family studyJ Abnorm Psychol201512487888926214708
- BeldenACIrvinKHajcakGet alNeural correlates of reward processing in depressed and healthy preschool-age childrenJ Am Acad Child Adolesc Psychiatry201655121081108927871643
- BarchDMWhalenDGilbertKet alNeural indicators of anhedonia: predictors and mechanisms of treatment change in a randomized clinical trial in early childhood depressionBiol Psychiatry2019851086387130583852
- JoynerKJBowyerCBYanceyJRet alBlunted reward sensitivity and trait disinhibition interact to predict substance use problemsClin Psychol Sci201971109112431853427
- LuckSJMathalonDHO’DonnellBFet alA roadmap for the development and validation of event-related potential biomarkers in schizophrenia researchBiol Psychiatry201170283421111401
- BeauchaineTPMcNultyTComorbidities and continuities as ontogenic processes: Toward a developmental spectrum model of externalizing psychopathologyDev Psychopathol2013254pt21505152824342853
- FrankEVimgaonkarVLPhillipsMLKupferDJAll the world’s a (clinical) stage: rethinking bipolar disorder from a longitudinal perspectiveMol Psychiatry201520233125048003
- McGorryPDNelsonBGolstoneSYungARClinical staging: A heuristic and practical strategy for new research and better health and social outcomes for psychotic and related mood disordersCan J Psychiatry201055848649720723276