
Abstract
Ever since psychiatry emerged as a clinical discipline and field of scientific inquiry in the late 18th century, debates about diagnosis have been at its very heart. Considered by many a requirement for clinical communication as well as for systematic study, others have critiqued psychiatric diagnosis for being modeled on a medical conception of disease that is ill-suited to the specific nature of mental disorders. Based on a review of seminal positions in the conceptual history of psychiatry and an examination of their epistemological underpinnings, we propose to consider diagnosis as dialogue. Such understanding, we argue, can serve as a meta-framework that provides a conceptual and practical umbrella to encourage open-minded conversation across the diverse conceptual and experiential frameworks that are characteristic of psychiatry. In this perspective psychopathology will also reinforce the interpersonal realm as a necessary element of any clinical encounter, be it diagnostic in purpose or otherwise. Current challenges to traditional diagnostic systems like Research Domain Criteria (RDoC) and Hierarchical Taxonomy of Psychopathology (HiTOP) are discussed in light of these considerations.
Desde finales del siglo XVIII, en que la psiquiatría surgió como disciplina clínica y campo de investigación científica, los debates acerca del diagnóstico han estado en su centro. Muchos lo han considerado como un requisito para la comunicación clínica, así como para el estudio sistemático, y otros han criticado el diagnóstico psiquiátrico por basarse en una concepción médica de la enfermedad, lo que no sería una buena adaptación a la naturaleza específica de los trastornos mentales. De acuerdo con una revisión de los planteamientos seminales en la historia conceptual de la psiquiatría y un examen de sus bases epistemológicas, se propone considerar el diagnóstico como un diálogo. Se argumenta que tal comprensión puede servir como un meta-marco que proporcione un paraguas conceptual y práctico para fomentar una conversación abierta a través de los diversos marcos conceptuales y experimentales que son característicos de la psiquiatría. De acuerdo con esta perspectiva, la psicopatología también reforzará el ámbito interpersonal como elemento necesario para cualquier encuentro clínico, ya sea de tipo diagnóstico u otro. A la luz de estas consideraciones, se discuten los desafíos actuales para los sistemas diagnósticos tradicionales como los Criterios de Dominio de Investigación (CDI) y la Taxonomía Jerárquica de la Psicopatología (TJP).
Le diagnostic en psychiatrie est au coeur de débats dans cette discipline devenue, à la fin du 18e siècle, à la fois clinique et domaine de recherche scientifique. Pour de nombreux médecins le diagnostic est aussi nécessaire à la communication qu’à la mise en œuvre d’études systématiques. D’autres en revanche ont critiqué cette conception médicale du diagnostic psychiatrique, inadaptée selon eux à la nature spécifique des troubles mentaux. Nous proposons d’envisager le diagnostic comme un dialogue, en examinant les positions fondamentales de l'histoire conceptuelle de la psychiatrie et leurs fondements épistémologiques. Selon nous, ce point de vue peut servir de méta-cadre pour un environnement conceptuel et pratique favorable à un échange ouvert au sein des divers contextes abstraits et expérientiels qui caractérisent la psychiatrie. Dans cette perspective, la psychopathologie renforcera également le domaine interpersonnel en tant qu'élément indispensable à toute rencontre clinique, que son but soit diagnostique ou non. Les méthodes de diagnostic traditionnelles, tels que les critères des domaines de recherche et la taxonomie hiérarchique de la psychopathologie, rencontrent aujourd’hui des difficultés examinées à la lumière de ces considérations.
Introduction: The entangled nature of psychiatric diagnosis
Ever since psychiatry emerged as an independent clinical discipline and field of scientific inquiry in the late 18 th century, debates about the concept (and content) of diagnosis have been at its very heart. Considered by many a requirement for clinical communication as well as for systematic study, others have critiqued psychiatric diagnosis for being modeled on a medical—in the sense of somatic—conception of disease that is ill-suited to the specific nature of mental disorders. Proponents of this latter position argue that psychiatric diagnosis disregards the complex individuality of any given person as well as cultural influences on diagnostic conceptions. Citation1 Taking this critical perspective further, “anti-psychiatrists” have claimed that psychiatric diagnosis is entirely normative—as opposed to descriptive—and a means of societal oppression. Citation2 A different, but related, point of critique has been the worry that psychiatric diagnosis rests too much on the assessment of the individual clinician, and that it grossly overrates intuition and personal experience, thereby giving an unacceptably high degree of power to the diagnostician and making diagnosis unreliable.
Whilst some criticisms, especially the lack of reliability, have been addressed by more recent research on and developments of diagnostic systems, the general points of contention remain: The epistemological dichotomy between conceptions of psychiatry as a quantifying nomothetic science searching for general rules behind the individual case on the one hand, and the (much older) “ars medica- approach” with its focus on qualitative, subjective phenomena to do with the individual person and thus being idiographic in nature on the other hand, results in conceptions of psychiatric diagnosis as “carving nature at its joints” Citation3 as opposed to views according to which psychiatric diagnosis is per se unfounded. Citation4 Debates about diagnosis can thus not be separated from debates about broader nosological and epistemological frameworks, and diagnosis necessarily mirrors the entangled nature of mental disorders.
What are we to do then if we take up a pragmatic position of minimal epistemological consensus and agree that diagnosis can indeed be helpful to condense information and thereby ensure reliable communication in clinical, research, and teaching contexts?
In this article, we propose to consider diagnosis as dialogue . This implies that we ought to be aware, and teach awareness, that diagnosis cannot be reduced to clear-cut, unequivocally applicable algorithms, but needs to be accompanied by reflection and discussion of its nosological, epistemological, and anthropological underpinnings.
To argue for such a conception, we first give an overview of landmark positions on diagnosis in the conceptual history of Western psychiatry. We then work out the general nosological frameworks underlying these positions, highlighting their implications for the epistemological status of diagnosis. Finally, current approaches to diagnosis are reviewed in light of these considerations. Diagnosis as dialogue, as we understand it, can serve as a meta-framework not to blur the lines where there are ontological or epistemological incommensurabilities between diagnostic systems, but to provide a conceptual and practical umbrella to make underlying theoretical assumptions explicit and to encourage open-minded conversation across diverse conceptual and experiential frameworks, both amongst clinicians and researchers as well as between clinicians and patients.
Landmark positions on diagnosis in the conceptual history of Western psychiatry
Two markedly different anthropological approaches accompanied and influenced the very beginning of psychiatry as a medical discipline: The era of Enlightenment in the 18 th century brought forward a strongly rational understanding of personhood and citizenship as well as an optimistic stance on the scientific comprehensibility, not to say mastery of our world. Autonomous and responsible decision making became one of the hallmarks of being a person. In turn, not being able to make use of one’s own rational powers was increasingly conceptualized not only as a deficit, but as an illness calling for medical diagnosis and treatment. Thus, the conceptual framework for establishing psychiatric diagnosis was rationalism .
Some decades later, at the beginning of the 19 th century, romanticism regarded a rationalistic attitude as simplifying and laid emphasis on the affective, not to say the irrational, dimension of human experience and behavior. Mental disorders were now regarded as consequences of excessive or otherwise disturbed affective states: Some authors saw a direct link between such affective instabilities and the person’s attitudes and lifestyle, thus attributing at least a significant part of the responsibility for becoming mentally ill to the patient himself or herself. The scope of psychiatric diagnosis thereby became broader and more value-laden as it conceived of mental illness as an aberration from the proper way of life. Here, the individual biography, personal attitudes, and accepted moral values of a given cultural context shaped the process of generating a psychiatric diagnosis.
Wilhelm Griesinger (1817-1868), a central figure in the conceptual history of psychiatry, pursued the understanding of psychiatry as an integral part of medicine, thus strictly departing from speculative philosophical approaches that had prevailed in the romantic era. Psychiatry should adopt empirical research methods, especially concerning the brain: Griesinger was therefore one of the founders of neuroscience, but he also insisted on the limitations of such an approach and warned not to prematurely accept oversimplifying views. Citation5 As for nosology, he vouched for the existence of just one all-embracing mental illness, the “unitary psychosis” (“Einheitspsychose”). He argued that there exists only one single mental disorder that in its different stages may exhibit the whole spectrum of psychopathological phenomena. Citation6 Hence, for Griesinger, diagnosis was centered around the clinical picture, its course in time, and possible correlations with brain dysfunctions , but not around presumably distinct nosological entities.
Based on Karl Ludwig Kahlbaum’s (1828-1899) proposal Citation7 to direct psychiatric research towards specific patterns in the temporality of defined clinical syndromes (“syndrome-course-entities”, “Syndrom-Verlaufs-Einheiten”), Emil Kraepelin (1856-1926) strongly and sustainably favored the idea of the existence and scientific detectability of “natural disease entities” (“natürliche Krankheitseinheiten”). Citation8,Citation9 He saw these entities as objective parts of nature, as given things, although he accepted different scientific ways to detect them: research on etiology, on pathological anatomy, or on clinical course. From this perspective, psychiatric diagnoses were tools to get as close as possible to “real” nosological entities .
Eugen Bleuler’s influential innovation in the present context—especially regarding “dementia praecox,” reconceptualized by him as “group of schizophrenias”—was to explicitly acknowledge a hermeneutical—specifically: a psychoanalytical—approach as a scientific element of psychiatric diagnosis, therapy, and research, notably without deemphasizing the role of descriptive and neurobiological factors. Citation10 Bleuler enriched the scope of diagnosis by the psychodynamic dimension , in this specific respect resembling ideas of “romantic psychiatry” a century before (see above).
The assumption that mental disorders were manifestations of a transgenerational process of “degeneration” (“Entartung”), although lacking a sound scientific basis and conceptual rigor, became highly influential in medicine in the late 19 th century. Citation11 Psychiatry was no exception; on the contrary: Most contemporary textbooks introduced chapters on “degenerative psychoses” or similar terms. Here, the process of diagnosis in a way succumbed to the underlying dogma by focusing on the detection of (somatic or psychopathological) “stigmata degenerationis” (Cesare Lombroso’s (1835-1909) “ Criminal anthropology ” Citation12 is a prominent example for this approach, but by far not the only one), thus grossly disregarding the subjective and interpersonal dimensions. This may be a drastic example of neglecting the patient’s individuality, of the very opposite of person-centeredness. However, any diagnostic approach in psychiatry does, in principle, carry this risk.
Considering the conceptual cornerstones of what became known as “psychotherapy” during the 20 th century, further frameworks, embedding the diagnostic process, emerged: In the psychoanalytical perspective , diagnosis cannot be neatly separated from therapy since the prominent role of interpretation both of the patient’s narratives and the therapeutic relationship essentially influences any single act within psychotherapy. As opposed to this, behaviorism , at least in its early phase, placed emphasis on the patient’s empirically observable and, therefore, quantifiable behavior, thus keeping its distance from the hermeneutical approach as well as from possible neurobiological underpinnings. Anthropological psychiatry emerged after World War II and, in fact, dominated psychiatric literature for a couple of years. It radically opposed the crude biologism and social Darwinism of psychiatry during the era of national socialism. Authors like Ludwig Binswanger (1881-1966) Citation13 and Wolfgang Blankenburg (1928-2002) Citation14 advocated a person- and biography-oriented approach, partly resembling, but not identical with the psychoanalytic one, that searched for a meaningful link between the patient’s mental disorder and his or her individual life. Note that the neurobiological dimension was not neglected in this view. It was credited as necessary, but not sufficient, not as the essential precondition of adequately dealing with the phenomenon of mental illness.
Systemic psychotherapy with its partly eclectic approach enriched the scope of psychotherapy by emphasizing the relevance of the patient’s social context, especially his or her family and occupational situation. Diagnosis had to encompass a much broader range of relevant information than, eg, in descriptive clinical psychopathology. (This outline of major theoretical approaches in psychotherapy focuses on the perspective of conceptual history. Towards the end of the 20th century, eclectic models were developed that explicitly drew on different schools of thought, eg, the Cognitive Behavioral Analysis System of Psychotherapy Citation15 ).
Concurrent to the discovery of new and effective psychopharmacological agents and their subsequent implementation into psychiatric practice starting from about 1950 onwards, the disadvantages of the highly heterogeneous field of psychiatric diagnosis (and nosology) became obvious. Large-scale international clinical studies depended on a common diagnostic language and especially on its reliability in order to quantify therapeutic response, side effects, and course of illness under treatment. This situation (together with the arrival of modern neuroscientific research methods as biochemistry or brain imaging) prompted the development of operationalized rating scales and, ultimately, diagnostic manuals such as ICD-10 Citation16 or DSM-III . Citation17 They strongly focus on reliability and, in order to achieve it, on precise definitions of psychopathological terms and diagnostic algorithms. This descriptive approach endeavors to avoid implicit theoretical presuppositions, especially regarding etiology and treatment of mental disorders. Not what, eg, schizophrenia “really is” or how it should be optimally treated, but how the term schizophrenia can be defined and used in a reliable way , is the very core of operationalized diagnosis in psychiatry (nominalistic approach, see below). Not leaving these common grounds, but as an amplification of ICD-10 , additional concepts have been proposed and clinically adapted, for instance, the “Operationalized Psychodynamic Diagnosis.” Citation18
In a remarkable step beyond the “atheoretical” ambition of ICD-10 , ICD-11 arranges disorders on the basis of shared putative etiological and pathophysiological features (eg, disorders associated with stress) as well as shared clinical phenomenology (eg, dissociative disorders). Citation19 Besides several new diagnoses and alterations to existing criteria of disorders, innovations in ICD-11 comprise the description of essential features of each disorder and the integration of a lifespan approach as well as culture-related information. Also, as in DSM-5 , disorder groupings were ordered to be related to developmental psychopathology (eg, neurodevelopmental disorders are enlisted first and neurocognitive disorders at the end). A major innovation is the incorporation of dimensional approaches within the framework of a categorical system with explicit taxonomic restrictions, especially applied in the classification of personality disorders Citation20 (and also partially for schizophrenia and other primary psychotic disorders).
Still, and like DSM-5 , ICD-11 in many ways offers no strict alternative to the current descriptive-phenomenological approach, and has not introduced fundamental conceptual alterations. One may argue, that ICD-11 ’s main advance is a technological one, ie, the transition to an electronic conceptual infrastructure, to a database that reflects the hierarchical structure of the classification and integrates within a single logical model all categories, conceptions, entities, groups, synonyms, and exclusion criteria as well as their relations (“foundation component” Citation21 ). The coding of diagnoses is altered, offering more precise and differentiated combinations. The documentation, multilingual utilization, and translations as well as linkage to other terminologies are facilitated.
Finally, two distinctively critical lines of thought towards psychiatric diagnosis in general shall be mentioned: Firstly, authors who reproached psychiatry for following a much too narrow medical model of mental disorders and for uncritically accepting the role of a social control agent (“anti-psychiatry”), regarded psychiatric diagnoses as pars pro toto for the alleged fundamental shortcomings of psychiatry. Citation2 The field of social psychiatry, emerging after 1960, took up, in a more moderate and pragmatic way, some of these arguments, especially concerning the medical model and its implicit risk of fostering rigid, stigmatizing and deindividualized diagnoses. Citation22
Secondly, since about 1980 a profoundly skeptical attitude arose towards nosological entities in psychiatry—and, consequently, towards diagnostic procedures codifying them—in the context of an increasingly neuroscientifically oriented self-understanding of psychiatry, in some respects revitalizing ideas Wilhelm Griesinger (and others) had proposed more than a century ago (see above). This position strongly gained momentum and condensed in a new term, “denosologization.” Van Praag’s plea from 1987 Citation23 triggered this debate that has been going on up to the present day; in fact, it was markedly boosted by recent concepts such as Research Domain Criteria (RDoC) Citation24 or Hierarchical Taxonomy of Psychopathology (HiTOP) Citation25,Citation26 and, generally, by the claim of the emerging fields of social neuroscience and computational psychiatry to generate “a new understanding of mental disorders.” Citation27 This will be addressed in more detail below.
General nosological frameworks and their implications for the epistemological status of psychiatric diagnosis
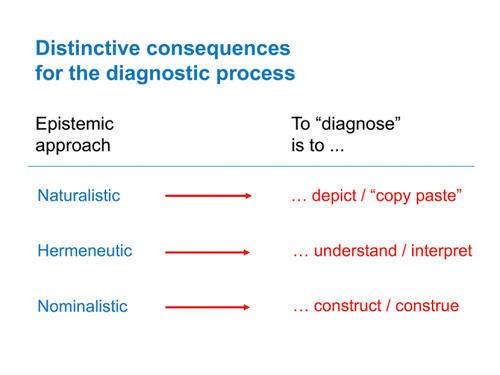
From the conceptions of diagnosis sketched above, that have become influential in the history of Western psychiatry, the following three general nosological frameworks can be distilled. They differ markedly in terms of their implications for the epistemological status of diagnosis and entail equally different approaches to the diagnostic process ( Figures 1 and 2 ).
Framework 1
Mental illness is a malfunction of certain parts, domains, or networks of the central nervous system that can be detected using neuroscientific methods .
Epistemologically, this approach is close to the classical medical model of somatic disorders. The factual existence of mental illness “within” the patient is regarded as completely independent from the experts’ conceptualization. The clinician just has to “detect” (and then, of course, treat) the illness, and the researcher strives to “carve nature at its joints.” Citation3 In philosophical terms, this is the naturalistic-realistic view . (“Realism” is here to be understood in an epistemological sense, ie, as the assumption that “natural objects” or “nature” exist completely independently from human beings and their cognitive acts). It typically implies a “reification” of mental illness. Citation28
Framework 2
Mental illness is an individual reaction to stressful life events or episodes. The brain’s relevance as a necessary condition for any mental phenomenon is not contested here. However, in contrast to framework 1, the central nervous system is not seen as the essential etiological factor. Rather, these are the patient’s life experiences, personality traits, and social competences. The underlying basis of diagnosis is thus conceptualized as mental phenomena that have to be interpreted or understood. Hence, hermeneutical methods constitute the center of this framework, which may be called the biographical view.
Framework 3
Mental illness is a concept based on descriptive psychopathological findings rather than on etiological assumptions. The definitions of symptoms and syndromes as well as diagnostic algorithms are products of an expert consensus, taking epidemiological and other scientific data into account wherever possible.
Diagnoses in this context do not claim to represent “real” entities that independently exist “behind” the clinical picture (as opposed especially to framework 1) but are conceptual conventions on how to use diagnostic terms. Hence, framework 3 can be called the nominalistic view . Such a view was prominently adopted by operationalized diagnostic manuals, eg, ICD-10 and DSM-5 . As discussed above, ICD-11 partially moves away from this position.
Implications for diagnosis
What are the implications of each of these frameworks for the epistemological status of psychiatric diagnosis and for the clinical process of diagnosing?
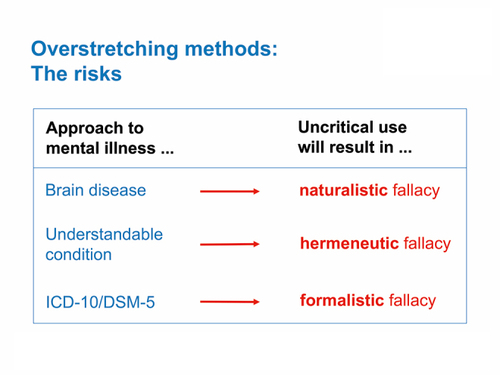
In a strictly naturalistic view, that claims to exhaustively explain mental illness as brain disorder, diagnoses represent “natural kinds.” To diagnose accordingly means to depict given facts in a way that is as objective, ie, researcher- or clinician-independent, as possible. Critics of this viewpoint note the naturalistic fallacy , ie, the risk of unreflected identification of (neuro-)biological with mental phenomena. Citation29
In the biographical view, diagnoses are patterns of experience and interindividually valid categories of meaning. In the diagnostic process, the clinician thus seeks to understand and interpret the patient’s personal history as well as his or her intra- and interpersonal situation. Emphasizing the explanatory power of these factors bears the risk of a hermeneutic fallacy , ie, the unreflected identification of a coherent psychological model with the etiology and pathogenesis of a given mental disorder.
Operational diagnostic manuals in psychiatry, like ICD-10 or DSM-5 , do not claim to address “real” nosological entities and therefore refrain from “reifying” mental illness. Instead, they construct diagnostic terms by defining rules or algorithms such that these terms can be reliably applied. One of their principal aims is not to make unnecessary theoretical assumptions, eg about the etiology or the “nature” of mental disorders, in order to be compatible with different methodological and cultural backgrounds. Taking this approach too far may result in a formalistic fallacy , ie, the unreflected identification of operationalized psychopathological criteria with the multifaceted mental suffering of the individual person.
As can be seen, there is a considerable link between nosological assumptions, be they explicitly stated or only implicitly influential, and practical diagnostic procedures. Any diagnostic approach comes with theoretical baggage, any one has its blind spots, and none therefore ought to be regarded as or used as a stand-alone-technique.
Why this is relevant for the ongoing debate
Conceptual history of psychiatry is not “l’art pour l’art.” Close readings and thorough reflections on “classical” psychiatric positions as, for example, in the works of Wilhelm Griesinger, Emil Kraepelin, Sigmund Freud, or Eugen Bleuler, facilitate and enrich the present debate on psychiatric diagnosis. This argument becomes even stronger in view of the immense heterogeneity and dynamics of this debate. It is situated (and, in a way, oscillates) between two poles: Emil Kraepelin’s notion of scientifically detectable “natural disease entities” based on philosophical realism on the one hand, Citation30 and the epistemologically more modest nominalistic approach of modern diagnostic manuals on the other hand. In recent years, both poles have been subjected to fierce criticism: From the 1980s onwards, the concept of “denosologization” has increasingly (re-)gained acceptance. More recently, it was integrated into the evolving paradigms of computational and dimensional psychiatry. Citation27 “Denosologization” is spurred by the worry that conventional psychiatric diagnoses—which are still based on Kraepelin’s nosology Citation19 —are neither sufficiently valid nor reliable, but in fact obstruct clinical work as well as scientific research by narrowing down the conceptual horizon. The poor acceptance of diagnoses by patients, relatives, and the general public to do with their stigmatizing potential is another common argument in favor of denosologization.
This complex issue may be condensed in one question: Do we need a “transdiagnostic psychiatry” Citation31 that departs from traditional nosological frameworks? Two recent examples of concepts following such a transdiagnostic path are RDoC Citation24 and HiTOP. Citation25,Citation26
RDoC epistemologically stands closer to Kraepelin’s postulate of the existence and scientific detectability of natural disease entities than to descriptive and hermeneutical concepts. However, its authors claim that nosology has to be data-based rather than, as conventional diagnosis, symptom-based. The substantial heterogeneity of a group of patients diagnosed with, eg, major depressive disorder according to ICD-10 , is sought to be overcome by integrating all available data from the domains genetic risk, brain activity, physiology, behavioral processes and life experiences, aiming to reveal data-based categories or clusters. These are expected to represent more homogenous groups of patients than, for example, ICD-10 categories. Ultimately, the new systematics is hoped to facilitate specifically targeted research on future pharmacological and psychotherapeutic strategies.
HiTOP shares RDoC’s criticisms of the classical taxonomies as neither sufficiently reliable nor valid. In response, it offers a data-driven psychometric methodology that attempts to advance consensus dimensional classification and thus enhance conventional diagnostic systems (like ICD and DSM ). Citation25 The objective is to define an inner structure of psychopathology. Using a quantitative higher-order dimensional and hierarchical structure of psychopathology, it aims at revealing underlying dimensions of psychopathology and decrease artefactual comorbidity. Citation32 In this way, arbitrary boundaries between disorders as well as insufficient reliability of categorical diagnoses are meant to be overcome. Citation26 Within-disorder heterogeneity is addressed by developing dimensions based on covariations of symptoms thereby detecting coherent constructs. At its core, HiTOP proposes that psychopathological dimensions can be organized in a hierarchical order that ranges from “spectra” (eg, “internalizing” or “thought disorder”), to specific clusters of symptoms. Citation32
The already thriving field of social neuroscience, dimensional and computational psychiatry will presumably be further enlarged and differentiated in the foreseeable future. There is no doubt that this is a scientifically desirable and promising development. However, the following caveat should be considered: The debate on future directions of psychiatric diagnosis critically depends on a sustained and substantial reflection on the epistemological frameworks involved. For example, how shall we integrate the notions of subjectivity, autonomy, and personhood with neuroscientific data? In order to justify the designation of an important realm of current psychiatric research as social neuroscience, this question has to be answered. The proposals of “first-person neuroscience” Citation33 and “two-person neuroscience” Citation34 are attempts to get ahead with this issue.
Generally speaking, any nosological and diagnostic approach developed by psychiatry ever since its beginning carries, more or less, the risk of becoming rigid and dogmatic. Therefore, the essential ambition of the ongoing debate on psychiatric diagnosis should not be to ignore or just to replace previous concepts. This would indefensibly narrow down the scientific scope of our field. Instead, social neuroscience, taken here as pars pro toto for recent conceptual and methodological advances in psychiatric research, should establish a conceptual dialogue , critical and constructive, with “classical” psychopathological concepts. The latter should not be scientifically devaluated only because they are part of a specific intellectual tradition.
The ambition to debate diagnosis in the abovementioned sense is supported by many seminal figures in the psychopathological tradition, especially Karl Jaspers (1883-1969). He declared a multidimensional, ie, epistemologically open-minded approach that engages in a critical dialogue between competing positions as necessary requirement of person-centered psychiatry. If we understand psychopathology in this Jaspersian sense, ie, as a comprehensive intellectual framework rather than only a technical guidance for descriptive symptomatology, it might well regain the function of a conceptual bracket for psychiatry. Citation35,Citation36 Given the fragile sense of professional identity within psychiatry we presently witness, such a bracket is very much needed.
Conclusion: what psychiatric diagnosis in the 21st century is all about
What is diagnosis in 21 st century psychiatry all about, and what ought it to be about? From a conceptual history perspective, in view of the many competing and at least partly incommensurable approaches to diagnosis that psychiatry has seen over the centuries, one cannot help but have the impression that psychiatric diagnosis is essentially about debate: This debate has been ongoing at least since the seminal work of Emil Kraepelin and, after a comparably stable phase of international implementation of the two operationalized diagnostic manuals DSM-III Citation17 and ICD-10 , Citation16 the field has become dynamic and substantially controversial again in recent years.
An essential background of this development is to be seen in new perspectives like computational and dimensional psychiatry, social neuroscience, or, generally speaking, in options for mental health issues that have arisen by “big data” and artificial intelligence. At first sight, these recent approaches might be regarded as predominantly methodological in nature; however, they do raise fundamental questions about psychiatric nosology and the epistemological status of diagnosis. This, for sure, is a positive development, since critical evaluation of any given concept is the very core of scientific progress. Therefore, RDoC, HiTOP, and comparable approaches are promising precisely by challenging traditional nosological and diagnostic concepts.
We have to be cautious however that their critique does not become dogmatic but is itself critically debated. As it stands (November 2019), such critical debate certainly takes place about the scientifically promising and practically relevant ICD-11 . Psychiatry, being as complex and entangled with a large variety of “external” factors as it is (and probably always will be), needs a substantial and sustained debate that addresses the foundations, including the conceptual history, of its nosological assumptions and diagnostic procedures. The latter are not only scientifically relevant, but also—explicitly or implicitly—underlie and thus guide everyday clinical work. The question should not be if we need a neurobiological, computational, or a psychopathological approach in psychiatry, but how to establish and foster a critical dialogue between these (and other) different perspectives. Citation37
For practical diagnostic work, this means that psychiatric diagnosis encompasses more than technical aspects of symptomatology and patient interviewing, and that psychiatric diagnosis is never an end in itself , neither in clinical practice nor in research about diagnostic processes. Of course, it does include technique—eg, knowing the definitions of psychopathological terms like delusional ideas, hallucinations, stupor etc, and knowing how to establish a therapeutic relationship so that the patient feels comfortable telling the interviewer about personal issues that are typically part of his or her private sphere. Citation38 But just as diagnostic systems are situated in a historical and cultural context, so is practical diagnosis situated in a cultural and—most importantly— interpersonal context. The act of diagnosis must thus be seen as an interpersonal act. This act too ought to be dialogical.
Understanding diagnosis as dialogue fits well with a Jaspersian understanding of what psychopathology basically is about: Psychopathology, we suggest, offers a conceptual bracket that allows keeping together the necessarily different scientific perspectives of psychiatry condensing in manifold debates about diagnosis. It also offers a framework positioning the interpersonal realm at the heart of any clinical encounter, be it diagnostic in purpose or otherwise. Furthermore, it can serve as an epistemological barrier against unreflected or undetected simplifications of psychiatry.
The authors declare that they have no conflict of interest regarding the content of this article
REFERENCES
- KirmayerLJLemelsonRCummingsCARe-Visioning Psychiatry: Cultural Phenomenology, Critical Neuroscience, and Global Mental Health2015 Cambridge, UK Cambridge University Press 10.1017/CBO9781139424745
- SzaszTThe Myth of Mental Illness: Foundations of a Theory of Personal Conduct [1961]1974 New York, NY Hoeber-Harper
- CampbellJKO’RourkeMSlaterMHCarving Nature at Its Joints: Natural Kinds in Metaphysics and Science2011 Cambridge, Mass MIT Press
- TimimiSNo more psychiatric labels: Why formal psychiatric diagnostic systems should be abolishedInt J Clin Health Psychol201414320821510.1016/j.ijchp.2014.03.004
- HoffPHippiusHWilhelm Griesinger (1817-1868)—sein Psychiatrieverständnis aus historischer und aktueller PerspektiveDer Nervenarzt2001721188589210.1007/s001150170026 11758099
- JanzarikWDie klinische Psychopathologie zwischen Griesinger und Kraepelin im Querschnitt des Jahres 1878Psychopathologie als Grundlagenwissenschaft19795161
- KahlbaumKDie Gruppierung der psychischen Krankheiten und die Eintheilung der Seelenstörungen1863 Danzig, Germany Kafemann
- KraepelinELehrbuch der Psychiatrie1896 Leipzig, Germany Barth
- HoffPEmil Kraepelin Und Die Psychiatrie Als Klinische Wissenschaft: Ein Beitrag Zum Selbstverständnis Psychiatrischer Forschung.201373 Heidelberg, Germany Springer-Verlag
- MaatzAHoffPAngstJEugen Bleuler’s schizophrenia—a modern perspectiveDialogues Clin Neurosci2015171434925987862
- ChamberlinJEGilmanSLDegeneration: The Dark Side of Progress1985 New York, NY Columbia University Press
- LombrosoCL’uomo Delinquente in Rapporto All’antropologia, Giurisprudenza e Alle Discipline Carcerarie187821 Turin, Italy Fratelli Bocca
- BinswangerLWahn [Delusion]1965 Pfullingen, Germany Verlag Gunther Neske
- BlankenburgWDer Verlust der natürlichen Selbstverständlichkeit: Ein Beitrag zur Psychopathologie symptomarmer Schizophrenien1971 Stuttgart, Germany Enke
- McCulloughJPTreatment for chronic depression using cognitive behavioral analysis system of psychotherapy (CBASP)J Clin Psychol200359883384610.1002/jclp.10176 12858425
- The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines 1992 Geneva, Switzerland World Health Organization WHO
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders19803rd ed.Washington, DCAmerican Psychiatric Association Publishing
- OPD Task ForceOperationalized Psychodynamic Diagnosis OPD-2: Manual of Diagnosis and Treatment Planning20081st ed.Ashland, OHHogrefe & Huber Publishers
- ReedGMFirstMBKoganCSet alInnovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disordersWorld Psychiatry201918131910.1002/wps.20611 30600616
- ReedGMProgress in developing a classification of personality disorders for ICD-11World Psychiatry201817222722910.1002/wps.20533 29856549
- International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision) 2018 Geneva, Switzerland World Health Organization
- ScheffTJBeing Mentally Ill: A Sociological Study2017 Abington-on-Thames, UK Routledge
- van PraagHMKahnRSAsnisGMet alDenosologization of biological psychiatry or the specificity of 5-HT disturbances in psychiatric disordersJ Affect Disord19871311810.1016/0165-0327(87)90067-x 2959695
- InselTCuthbertBGarveyMet alResearch Domain Criteria (RDoC): Toward a new classification framework for research on mental disordersAm J Psychiatry2010167774875110.1176/appi.ajp.2010.09091379 20595427
- KotovRKruegerRFWatsonDet alThe Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologiesJ Abnorm Psychol2017126445447728333488
- KotovRKruegerRFWatsonDA paradigm shift in psychiatric classification: the Hierarchical Taxonomy Of Psychopathology (HiTOP)World Psychiatry2018171242510.1002/wps.20478 29352543
- HeinzAA New Understanding of Mental Disorders: Computational Models for Dimensional Psychiatry2017 Cambridge, MA MIT Press
- HoffPKendlerKParnasJOn reification of mental illness: historical and conceptual issues from Emil Kraepelin and Eugen Bleuler to DSM-5 Philosophical Issues in Psychiatry IV: Classification of Psychiatric Illness2017 Oxford, UK Oxford University Press
- ZacharPPsychiatric disorders are not natural kindsPhilos Psychiatr Psychol200073167182
- HoffPZum Krankheitsbegriff bei Emil KraepelinNervenarzt1985565105133908947
- Fusar-PoliPSolmiMBrondinoNet alTransdiagnostic psychiatry: a systematic reviewWorld Psychiatry201918219220710.1002/wps.20631 31059629
- KruegerRFKotovRWatsonDet alProgress in achieving quantitative classification of psychopathologyWorld Psychiatry201817328229310.1002/wps.20566 30229571
- NorthoffGHeinzelAFirst-person neuroscience: A new methodological approach for linking mental and neuronal statesPhilos Ethics Humanit Med20061310.1186/1747-5341-1-3
- LeongVSchilbachLThe promise of two-person neuroscience for developmental psychiatry: using interaction-based sociometrics to identify disorders of social interactionBr J Psychiatry2019215563663810.1192/bjp.2019.73
- HoffPDo social psychiatry and neurosciences need psychopathology-and if yes, what for?Int Rev Psychiatry200820651552010.1080/09540260802564797 19085407
- StanghelliniGBroomeMRPsychopathology as the basic science of psychiatryBr J Psychiatry2014205316917010.1192/bjp.bp.113.138974 25179621
- HoffPBottlenderRNeurowissenschaft und Psychopathologie heute—Ergänzung, Fusion, Verdrängung?Zeitschrift für Psychiatrie, Psychologie und Psychotherapie201260424925610.1024/1661-4747/a000124
- MaatzASchnellerLHoffPTrachselMTekinSBiller-AndornoNGaabJSadlerJPrivacy and confidentiality in psychotherapy: Conceptual background and ethical considerations in light of clinical challengesOxford Handbook of Psychotherapy Ethics2019 Oxford, UK Oxford University Press