
Abstract
Background
Vitamin A deficiency is considered as one of the public health problems among pregnant women worldwide. Population representative data on vitamin A status in pregnancy have not previously been published from Iran.
Objectives
The aim of this study was to publish data on vitamin A status in pregnant women in all the provinces of Iran in 2001, including urban and rural areas, and to describe the association of vitamin A status with maternal age, gestational age, and parity.
Design
This descriptive cross-sectional study was conducted on 3,270 healthy pregnant women from the entire country, 2,631 with gestational age ≤36 weeks, and 639 with gestational age >36 weeks. Vitamin A status was determined in serum using high-performance liquid chromatography.
Result
Retinol levels corresponding to deficiency were detected in 6.6% (<0.36 µmol/L) and 18% had insufficient vitamin A levels (≥0.36–<0.7 µmol/L). Suboptimal level of serum retinol was observed in 55.3% of the pregnant women (0.7–1.4 µmol/L). Only about 20% of the women had optimal values (>1.4 µmol/L). The level of serum retinol was lower in older pregnant women (p=0.008), and at higher gestational age (p=0.009). High vitamin A levels were observed in pregnant women in the central areas of Iran and the lowest values in those in the southern areas of Iran.
Conclusions
The vitamin A status was good in 2001 but should be closely monitored also in the future. About 25% of pregnant women had a vitamin A status diagnosed as insufficient or deficient (<0.7 µmol/L). The mean serum retinol decreased as the gestational age increased. The clinical significance of this finding should be further investigated, followed by a careful risk group approach to supplementation during pregnancy.
To access the supplementary material to this article please see Supplementary files under Article Tools online
Vitamin A deficiency is considered as one of the main public health problems in developing countries, where it is one of the main causes of high morbidity and mortality. Vitamin A is important for several functions, including vision, reproduction, growth, immunity, maintenance of epithelial tissue, and regulation of cell proliferation and differentiation (Citation1, Citation2). In addition, vitamin A effects are critical during periods of rapid cellular growth and differentiation, such as during pregnancy, when it is supplied by the mother to the fetus (Citation1).
Vitamin A comes from two sources, one comes from animal sources, which includes retinol, and the other group comes from plants, which includes beta-carotene. The body converts beta-carotene to vitamin A. Vitamin A can have significant toxicity in overdose, but provitamin A carotenoids does not cause vitamin A toxicity even in large doses because the body converts only what it needs.
Good food sources of vitamin A are liver, eggs, red and orange fruits, red palm oil, and green leafy vegetables (Citation3), while in Iran the main vitamin A intake comes from vegetables (44%), meat and eggs (18%), fruit (9%), dairy products (12%), and fat (3%) (Citation4). The majority of dietary vitamin A is stored in the liver in well-nourished people. Vitamin A restriction does not immediately lead to deficiency symptoms, those would emerge slowly since it takes 1 to 2 years for healthy adults, shorter for children, to empty liver stores (Citation5). The major cause of vitamin A deficiency is insufficient intake, which is related to socio-cultural and socioeconomic factors such as poverty, low access to vitamin A fortified food (Citation6, Citation7), low education, ethnicity, dietary practices and beliefs, and climate conditions (Citation8). A low vitamin A status in pregnant women can also be attributed to multiple pregnancies and minimal antenatal care (Citation9).
In the World Declaration and Plan of Action for Nutrition (Citation10) from 1992, 159 governments pledged to undertake all efforts to eliminate vitamin A deficiency within the decade, a pledge which was not fulfilled. Micronutrient deficiencies are one of the main public health concerns. Vitamin A deficiency is one of the most important nutritional problems because of its health consequences and wide geographic distribution. Globally, about 15% (19 million) of pregnant women have been estimated to be vitamin A deficient (Citation3), and one study suggested that about 2.5–5 million women worldwide would probably be suffering from night blindness (Citation11).
Low vitamin A status during pregnancy can result in a low vitamin A status of the infant at birth and in the early life. Vitamin A deficiency is strongly associated with depressed immune function and higher morbidity and mortality due to infectious diseases such as diarrhea, measles, and respiratory infections in children (Citation12).
Meanwhile, teratogenic symptoms of excessive vitamin A intake (in its preformed state, retinol) during pregnancy have been shown. Birth defects, such as the retinoic acid syndrome, include those affecting the central nervous system, cardiovascular system, thymus malformations, and neural tube defects (Citation13, Citation14).
The estimated average requirement (EAR) for vitamin A in pregnant women is, according to the Dietary Reference Intakes from 2001, 770 µg retinol activity equivalents (RAE)/day for women aged above 19 years and 750 µg RAE/day for pregnant women aged 14 to 19 years (Citation15). According to the Dietary Reference Intakes, the tolerable Upper Level (UL) for adults is set at 3,000 µg RAE/day of preformed vitamin A (Citation15). Deficient and insufficient serum concentrations of vitamin A are determined as <0.36 and ≥0.36<0.7 µmol/L, respectively, and suboptimal and optimal concentrations of vitamin A as ≥0.7<1.4 µmol/L and ≥1.4 µmol/L, respectively (Citation16). According to the World Health Organization (WHO) (Citation10), three categories of national prevalence of vitamin A deficiency (where the blood level is less than 0.7 µmol/L) have been proposed, mild ≥2–10%, moderate 10–20%, and severe ≥20% on a population basis. These categories are suggested to indicate the severity of the problem and to thereby show the need for making vitamin A nutrition a national priority where needed. The prevalence of vitamin A deficiency (less than 0.7 µmol/L) in cord blood in previous report from Tehran was 21% on a population representative material (Citation17).
From a public health perspective, the global concerns to prevent and eliminate vitamin A deficiency are mainly due to its serious consequences and multiple effects on human health, especially the health of infants and women in reproductive age in developing countries (Citation11).
The aim of this study was to publish data on vitamin A status in pregnant women in all the provinces of Iran, including urban and rural areas, and to describe the association of vitamin A status with maternal age, gestational age, and parity.
Methods
Iran can be divided into 11 regions with 28 provinces (Supplementary file), based on ethnographic, demographic, epidemiologic, and socioeconomic factors (Citation18). This study was cross-sectional and was conducted during the year 2001 in Iran. It was a part of the micronutrient survey, which covered the whole country and was conducted by the Ministry of Health (MOH) of Iran.
The study population was households and the sampling method was unequal cluster sampling with unequal household sizes randomly selected throughout the country. The clusters were sampled relative to the size of the urban and rural population of each province in all 11 regions. The center of the cluster was selected by systematic random sampling. There were 880 clusters in all 11 regions, 504 urban and 376 rural clusters.
Before the study was conducted, a team of health workers in each health care center in urban and rural areas were selected. Each team was assigned to pick up at least five people for the study from each subregion. Pregnant women were informed about the study process. Assigned pregnant women gave informed consent, and accepted to give blood samples and complete questionnaires. These pregnant women were targeted in their own provinces by written invitation at the nearest health care center that belonged to their region. If a woman was not able to go to the health care center within the due date, the survey staff would go to the woman's house and invite her to participate in the study. As an inclusion criterion, it was important that the pregnant women were otherwise healthy and did not have any kind of chronic diseases such as diabetes or heart disease. The blood samples were collected carefully by trained health workers. The total number of pregnant women who participated in the study was 4,368 from all regions of Iran, but data on vitamin A levels were only available in 3,270 women.
A questionnaire was designed by the MOH in Iran to collect information about mothers on general characteristics, health status, supplements if used, number of abortions, pregnancies, and deliveries.
From each participant, a minimum of 6.5 mL venous blood was collected and kept in dry ice and sent to an accredited district laboratory for centrifugation. The samples were coded and kept at −20°C until analysis. All samples were transported in a refrigerated vehicle to an accredited laboratory in Tehran. Vitamin A was analyzed as retinol by using high-performance liquid chromatography (HPLC) at the WHO collaborating laboratory in Tehran after the samples were transported there in a cold chain vehicle.
Statistical analysis
Data for 3,270 pregnant women were analyzed with SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). One-way ANOVA test was carried out to test the significant differences between the mean of vitamin A levels within groups with different age and gestational age. Vitamin A was normally distributed among the study population. Post Hoc tests were computed to investigate differences in the categories. One-way ANOVA test was computed to test the significant difference of parity on vitamin A status. Two-way ANOVA test was carried out to test the impact of age and areas (rural and urban) on the levels of vitamin A in pregnant women. Mean (standard deviation, SD) is given if not otherwise indicated. The level of significance was set at p≤0.05.
Ethical approval
The approval for this study was obtained from the Ethics Committee of the MOH in Iran. Informed consent was obtained from all women.
Results
The mean age of the participating women was 26 years, ranging from 14 to 47 years. The mean parity was 2, ranging between 1 and 12 deliveries. Gestational age ranged from 22 to 42 weeks at the time of blood sampling. The number of included pregnant women in the 11 regions varied between 229 and 330 (). Mean (SD) values of serum vitamin A ranged from 0.77 (0.46) to 1.12 (0.43) µmol/L. In , the regional as well as national mean (SD) levels of vitamin A as well as prevalence rates within the categories deficient, insufficient, suboptimal, and optimal is shown. The combined prevalence rates within the categories deficient and insufficient (<0.7 µmol/L) are also shown. The highest mean plasma retinol level (1.12 µmol/L [0.43]) was found in central Iran (region 6). Deficiency was mainly seen in regions 2, 5, 7, 8, and 11. Only 6.6% showed deficiency (<0.36 µmol/L), while 18.3% had insufficiency (0.36–<0.7 µmol/L) indicating that the population prevalence below 0.7 µmol/L for the whole nation is well above 20% (24.9%) and should therefore be characterized as severe according to the WHO categories. In some parts of the country the prevalence below 0.7 µmol/L is over 30% (Citation3, Citation11) with one region reaching the level of 45.9% (Citation7).
Table 1 The mean (±SD) of plasma retinol levels in pregnant women and the percentage distribution of deficient, insufficient, suboptimal, and optimal levels
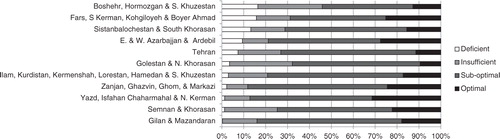
In , the percentage distribution of vitamin A status is shown for the 11 regions. Deficiency was mainly seen in regions 2, 5, 7, 8, and 11. The highest optimal percentage of vitamin A was in regions 2, 4, 6, 9, and 11. More than half of pregnant women had serum vitamin A with suboptimal level, while vitamin A deficiency was only seen in less than 7% of all pregnant women in the study, and insufficiency in 18%.
Fig. 1 Percentage distribution of vitamin A status in the 11 regions of Iran.
No statistical differences were observed between rural and urban areas. The mean (SD) vitamin A level in rural and urban areas were 0.98 (0.4) and 1.00 (0.4) µmol/L, respectively.
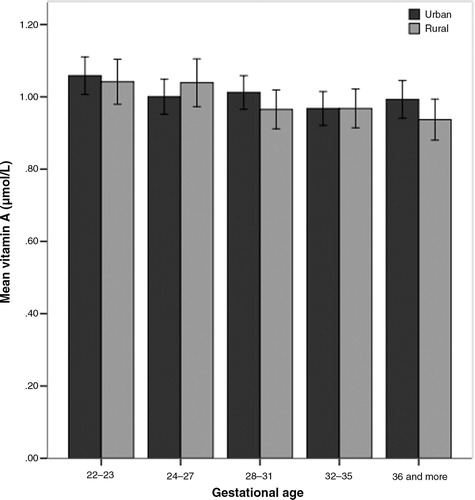
Vitamin A in each age group was slightly lower in rural than that in urban areas. A two-way ANOVA for group analysis of variance was performed. The difference showed that the difference of vitamin A in both areas was not statistically significant. However, there was a statistically significant main effect of age on vitamin A level (p=0.005). Using the same test, this effect size was rather small (eta squared=0.003) ().
Fig. 2 Mean vitamin A in rural and urban areas at different gestational age groups. Error bars represent 95% CI.
Vitamin A levels in pregnant women decreased by increasing maternal age (ANOVA, p=0.005) (). Women who were less than 23 years old had higher levels of serum retinol than the older ones. There was a weak negative but significant correlation between age and vitamin A status (Pearson correlation, r=−0.047, p=0.007).
Table 2 The mean±SD of vitamin A (µmol/L) in pregnant women at different age groups
shows levels of vitamin A in pregnant women during different gestational ages. The mean vitamin A decreased as the gestational age increased (p=0.009, one-way ANOVA). The mean serum retinol decreased as the gestational age increased (p=0.009, one-way ANOVA).
Table 3 Mean±SD of vitamin A (µmol/L) in pregnant women with different gestational age
There was no significant relation between parity and vitamin A status (F=0.79, p=0.45) as shown in .
Table 4 Mean±SD of vitamin A (µmol/L) in pregnant women with different parity
Discussion
This study showed that pregnant women in 2001 in this nationally representative study from Iran had a low vitamin A status since 25% of pregnant women had insufficient or deficient vitamin A levels. Using the WHO cut-offs for national prevalence of vitamin A deficiency, Iran should by this standard be considered a country with severe vitamin A insufficiency prevalence (<0.7 µmol/L) in 2001. In contrast, reports from the north of Iran, Marand district, in 2002 showed that 2.1% of child-bearing women had a deficiency level of vitamin A (<0.7 µmol/L) but 18% had values between insufficient or suboptimal level of vitamin A (Citation19). Prevalence of deficiency levels (<0.36 µmol/L) was 6.6% nation-wide and similar to the average global prevalence of maternal vitamin A deficiency in developing countries (7%) (Citation20). The highest prevalence of deficiency to our knowledge was reported from Nepal (31%) (Citation21), about five times higher than in Iran. China had the lowest prevalence of deficiency, only 2% in 2001 (Citation21, Citation22). In contrast, data from WHO in 2005 showed that on average 11.6% of pregnant women in Europe had vitamin A deficiency, ranging from 2.6 to 20.6% over the past 15 years (Citation10). Maternal vitamin A deficiency was also correlated to a reduced intra-uterine growth rate and birth weight, and higher infant mortality Citation23–(Citation25) .
The prevalence of vitamin A deficiency we found indicates a slight improvement in vitamin A status from severe to moderate deficiency during 1989 to 2001 (Citation10). A general severe deficiency of vitamin A in cord blood in male infants in 1989 developed into moderate deficiency in 2001 in Iran (Citation17). Despite the improvement in prenatal health care facilities, which in the meanwhile have been organized in each province supplying multivitamin (vitamins A+D) supplements free of charge through the Primary Health Care system. Supplementation of vitamin A to infants from 2 weeks of age until 2 years by MOH in the past decades may be responsible for a previous finding that vitamin A deficiency and insufficiency were rare in infancy (Citation18). The higher prevalence of insufficient vitamin A levels in the south of Iran might be associated with lower contribution of animal and milk products to the total energy intake, being 6 and 1%, respectively, in comparison with central and north of Iran, where animal and milk products contributed to about 8 and 4%, respectively, of the total energy intake (Citation26). A low access in the south of Iran to main sources of vitamin A (dairy products, vegetables, and fruits) may be related to the hot and dry climate in this region (Citation27). One study in northwest of Iran showed that the important sources of vitamin A in child-bearing women were nuts and green leaves, products that were not typical of other populations (Citation19). Vegetables and fruits provide carotenoids equivalent to more than 50% of vitamin A (Citation4). MOH reported that the ‘intake to need’ ratio of vitamin A shows a scattered provincial distribution, from 60% in Sistanbalouchestanto to 100% in East Azarbayejan (Citation26). This is in accordance with the consumption of the main sources of vitamin A in the south of Iran, that is, Sistanbalouchestan is low ranking in both urban and rural areas. This might also be related to socioeconomic status, drought, and low production of fruits and vegetables.
Referring to the UN Food and Agriculture Organization (FAO) regarding the nutritional intake in Iran (2002), the average daily intake of vitamin A was lower in villages than in towns, but insufficient in both, based on lower intake of animal products, fruits, and vegetables (Citation26). In this study, the level of vitamin A deficiency was almost the same in both areas.
The association between the status of vitamin A and age has been reported earlier (Citation10, Citation21) and has been related to factors such as dietary patterns and life-style that influence the nutritional status (Citation28). The current study revealed that there was a significant correlation between gestational age and serum retinol. Similarly, among Nepalese pregnant women, even though the prevalence of vitamin A deficiency was higher only in late pregnancy, it lead to night blindness (Citation9). This might be explained by an increased vitamin A-transfer to the fetus during late pregnancy. In contrast to our finding regarding the negative association of vitamin A with age, it has been reported elsewhere that night-blind women were more likely to be teenagers; however, the risk again increased with age among women aged above 30 (Citation9). The difference could be explained by the fact that the Nepalese study reported data based on whether the women had night blindness during pregnancy or not, while our study reported serum retinol levels. In addition, we had no records of the socioeconomic status which could be an influencing factor here, as it has been shown in the previously mentioned study (Citation9). Relation between serum retinol to parity. Similar to our findings, one study in Bangladesh showed no correlation between parity and serum retinol (Citation29).
A limitation to our study was that investigations at the regional level in the 11 included regions did not include data on sociodemographic differences.
Conclusions
This study illustrates that the status of vitamin A was good in 75% of pregnant women in Iran. As the WHO goal is to eliminate vitamin A deficiency globally, this study shows that Iran has achieved a relatively good result historically in the drive to eliminate vitamin A deficiency only in some provinces but not at the national level. Therefore, the problem needs to be closely monitored. Since this data does not represent the current status of vitamin A in the country, further information on vitamin A status in pregnant women are required for a strict surveillance of this important problem and to ensure that the vitamin A status continues to improve in Iran.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Appendix
Download MS Word (982.6 KB)Acknowledgement
Special thanks go to the Deputy Minister of Health, the Nutrition Department in the Ministry of Health, the Secretariat of Applied Research in the Ministry of Health, the National Nutrition and Food Technology Research Institute. We are also grateful to Dr. Robabe Shikholeslam for her assistance.
Notes
To access the supplementary material to this article please see Supplementary files under Article Tools online
References
- Azais-Braesco V, Pascal G. Vitamin A in pregnancy: requirements and safety limits. Am J Clin Nutr. 2000; 71: 1325S–33S. [PubMed Abstract].
- Blomhoff R, Green MH, Green JB, Berg T, Norum KR. Vitamin A metabolism: new perspectives on absorption, transport, and storage. Physiol Rev. 1991; 71: 951–90. [PubMed Abstract].
- UNICEF. Monitoring the situation of children and women. 2009. http://www.childinfo.org/vitamina.html [cited 28 December 2010]..
- NNFTRI. National Nutrition and Food Technology Research Institute. National comprehensive study on household food consumption pattern and nutritional status in Iran (2001–2003). http://www.agri-peri.ir/AKHBAR/86/aban/kargah/first day/Dr dorosty/FoodSecurity.pdf [cited 28 December 2010]..
- Bendich A. The safety of beta-carotene. Nutr Cancer. 1988; 11: 207–14.
- Dary O, Mora JO. Food fortification to reduce vitamin A deficiency: International Vitamin A Consultative Group recommendations. J Nutr. 2002; 132: 2927S–33S. [PubMed Abstract].
- Underwood BA. Maternal vitamin A status and its importance in infancy and early childhood. Am J Clin Nutr. 1994; 59: 517S–22S; discussion 22S–24S. [PubMed Abstract].
- Lee V, Ahmed F, Wada S, Ahmed T, Ahmed AS, Parvin Banu C, etal. Extent of vitamin A deficiency among rural pregnant women in Bangladesh. Public Health Nutr. 2008; 11: 1326–31.
- Katz J, Khatry SK, West KP, Humphrey JH, Leclerq SC, Kimbrough E, etal. Night blindness is prevalent during pregnancy and lactation in rural Nepal. J Nutr. 1995; 125: 2122–7. [PubMed Abstract].
- World Health Organization. Global prevalence of vitamin A deficiency in population at risk: 1995–2005. 2011. http://www.who.int/vmnis/vitamina/prevalence/report/en/ [cited 15 January 2011]..
- Qazaq HS, Aladeeb NZ, Al-Masri J. Is vitamin A deficiency a problem among pregnant Emirati women in Al-Ain City?. East Mediterr Health J. 2005; 11: 648–56. [PubMed Abstract].
- Ortega RM, Andres P, Martinez RM, Lopez-Sobaler AM. Vitamin A status during the third trimester of pregnancy in Spanish women: influence on concentrations of vitamin A in breast milk. Am J Clin Nutr. 1997; 66: 564–8. [PubMed Abstract].
- Dudas I, Czeizel AE. Use of 6,000 IU vitamin A during early pregnancy without teratogenic effect. Teratology. 1992; 45: 335–6.
- Lammer EJ, Chen DT, Hoar RM, Agnish ND, Benke PJ, Braun JT, etal. Retinoic acid embryopathy. N Engl J Med. 1985; 313: 837–41.
- Institute of Medicine. Food and Nutrition Board. Dietary reference intakes for vitamin A VK, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. 2001; Washington, DC: National Academy Press.
- Blomhoff R, Vitamin A. In Nordic nutrition recommendations 2004: integrating nutrition and physical activity. 2004; Copenhagen: Nordic Council of Ministers.
- Yassai MB, Malek F. Newborns vitamin A in relation to sex and birth weight. J Trop Pediatr. 1989; 35: 247–9.
- Olang B, Naghavi M, Bastani D, Strandvik B, Yngve A. Optimal vitamin A and suboptimal vitamin D status are common in Iranian infants. Acta Paediatr. 2011; 100: 439–44.
- Omidvar N, Ghazi-Tabatabie M, Harrison GG, Eghtesadi S, Mahboob SA, Pourbakht M. Development and validation of a short food-frequency questionnaire for screening women of childbearing age for vitamin A status in northwestern Iran. Food Nutr Bull. 2002; 23: 73–82. [PubMed Abstract].
- Rice AL, West KP, Black R. Vitamin A deficiency: counting the cost in women's lives. United States Agency for International Development (USAID) & Academy for Educational Development (AED). 2007. http://www.aed.org/Publications/upload/Vitamin-A-and-maternal-mortality-Final.pdf [cited 15 January 2011]..
- West KP Jr.. Extent of vitamin A deficiency among preschool children and women of reproductive age. J Nutr. 2002; 132: 2857S–66S. [PubMed Abstract].
- Lin L, Liu Y, Ma G, Tan Z, Zhang X, Jiang J, etal. [Survey on vitamin A deficiency in children under-6-years in China]. Zhonghua Yu Fang Yi Xue Za Zhi. 2002; 36: 315–19. [PubMed Abstract].
- Dabi DR, Parakh M, Bothra A. A study of maternal vitamin A status and its relationship with intrauterine growth restriction. J Obstet Gynecol India. 2006; 56: 489–94.
- Semba RD, Miotti PG, Chiphangwi JD, Dallabetta G, Yang LP, Saah A, etal. Maternal vitamin A deficiency and infant mortality in Malawi. J Trop Pediatr. 1998; 44: 232–4.
- Tielsch JM, Rahmathullah L, Katz J, Thulasiraj RD, Coles C, Sheeladevi S, etal. Maternal night blindness during pregnancy is associated with low birthweight, morbidity, and poor growth in South India. J Nutr. 2008; 138: 787–92. [PubMed Abstract].
- Nutrition country profiles. [database on the Internet]. 2010. http://www.fao.org/ag/AGN/nutrition/IRN_en.stm [cited 28 December 2010]..
- Ghassemi H, Harrison G, Mohammad K. An accelerated nutrition transition in Iran. Public Health Nutr. 2002; 5: 149–55.
- Succari M, Garric B, Ponteziere C, Miocque M, Cals MJ. Influence of sex and age on vitamin A and E status. Age Ageing. 1991; 20: 413–16.
- Ahmed F. Vitamin A deficiency in Bangladesh: a review and recommendations for improvement. Public Health Nutr. 1999; 2: 1–14.