Abstract
Background: Reducing maternal and perinatal mortality in sub Saharan Africa remains challenging and requires effective and context specific interventions.
Objective: The aims of this paper were to demonstrate the impact of the community mobilisation of the Skilled Care Initiative (SCI) in reducing maternal and perinatal mortality and to describe the concept and implementation in order to guide replication and scaling up.
Designs: A quasi experimental design was used to assess the extent to which the SCI was associated with increased institutional births, maternal and perinatal mortality reduction in an intervention (Ouargaye) versus a comparison (Diapaga) district. A geo-referenced census was conducted to retrospectively assess changes in outcomes and process measures. A detailed description of activities, rationale and timing of implementation were gathered from the SCI project officers and summarised. Data analyses included descriptive statistics and multivariate analyses.
Results: At macro level, the main significant difference between Ouargaye and Diapaga districts was the scope and intensity of the community-based interventions implemented in Ouargaye. There was a temporal association relationship before and after the implementation of the demand-driven interventions and a remarkable 30% increase in institutional births in the intervention district compared to 10% increase in comparison district. There was a significant reduction of perinatal mortality rates (OR =0.75, CI 0.70–0.80) in intervention district and a larger decrease in maternal mortality ratios in intervention district, although statistical significance was not reached. A comprehensive framework of community mobilisation strategy is proposed to improve maternal and child health in poorest communities.
Conclusion: Controlling for the availability and quality of health services, working in partnership and effectively with communities, and not for them – hence characterising communities as not being empty vessels – can have impacts on outcomes. Here, in the district with a community mobilisation programme, there was a marked increase in institutional births and reductions in maternal and perinatal deaths.
The rationale and effectiveness of community-based interventions on maternal and child health are not new and have been widely reported Citation1. These community-based interventions are referred to as community participation, community empowerment or social mobilisation and aim to increase the use of maternal health services Citation2Citation3Citation4, and to reduce maternal and perinatal mortality Citation1. Most community-based interventions involve the use of lay people referred to as community motivators, community health agents, community health workers among others Citation5Citation6. Although the requirement for both supply and demand side interventions are implicit and acknowledged in maternal mortality reduction frameworks, in practice, most maternal and perinatal reduction strategies have mainly focused on the supply side and more tangible interventions (such as buildings, equipments, vehicles, staffing, training and supervision among others). The added value of community-driven interventions, scope and configuration are not well known, and thus overlooked. The Skilled Care Initiative (SCI) developed and implemented in Ouargaye district, Burkina Faso Citation7, offers the opportunity to access the extent of the impact of demand-driven interventions implemented after the strengthening of the health system (upgrading the infrastructures, equipments and supplies, referral system, skills and competences of health personnel) in improving institutional delivery, and in reducing maternal and perinatal mortality. The evaluation methodology has been extensively reported elsewhere Citation8Citation9Citation10. This paper focuses on demonstrating the added value of the demand-driven interventions (community mobilisation) of the SCI and on describing the concept and implementation to guide future replication and scaling up.
1 Process of community mobilisation strategy
1.1 Community mobilisation: concepts and rationale
As part of the SCI Citation7, several community-based interventions were implemented in Ouargaye district from 2004 to 2005. The community-based interventions’ overall goal was to guide the community towards the use of quality delivery care during normal and complicated deliveries. The approach was developed after a review of previous community-based interventions towards maternal and child health in Burkina Faso, among which were the Tostan approach and the Maternal and Neontal Health approach in Bazega province and Koupéla district, respectively Citation11Citation12.
The approach was based on the concept of social mobilisation (), defined as a process, a movement of the population leading to behavioural changes towards a specific problem, mostly health related but also applicable to other development sectors such as education or agriculture Citation11. The social mobilisation – and thus, community mobilisation when restricted to a community – is summarised into four interrelated and complementary pillars: advocacy and awareness, social marketing, behavioural change communication (BCC) and capacity strengthening (), each of which is briefly described below along with its rationale.
Figure 1. Conceptual framework for maternal and child health community-based interventions.
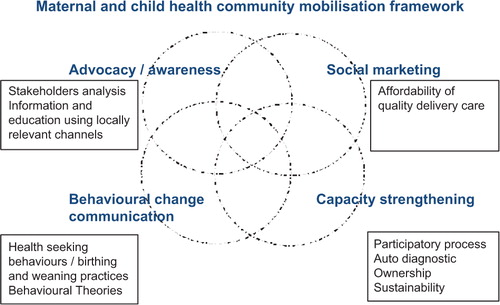
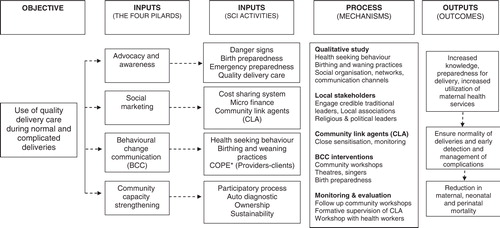
Figure 2. Logic model of community mobilisation strategy applied to the SCI, Ouargaye district, Burkina Faso
Awareness aims at engaging local traditional leaders, administrative and religious leaders, local associations with the use of skilled care through problem-solving techniques, negotiation, and persuasion and lobbying. It focuses on danger signs during pregnancy and delivery, birth preparedness Citation13, emergency preparedness and quality delivery care. In a context of low literacy, and where there is a value for community self identification and where communities are responsive to recommendations of religious and traditional leaders, it is critical that any intervention in a community meets the needs of local stakeholders and wins their support. Communities are not ‘empty vessels’ and understanding and building upon cultural beliefs of care and means of communication is more likely to be effective.
Social marketing postulates quality services at affordable price. In this framework, community-based interventions through social marketing aim at reducing financial barriers and out of pocket for the use of skilled care. There is no one-size-fits-all approach and communities are encouraged to use acceptable and effective strategies.
The third pillar is BCC. Much has been written on BCC theories such as learning theories, the transtheoretical model, the health belief model, reasoned action and planned behaviour, and social cognitive theory Citation14 among others. It is expected that each community use the most relevant, acceptable and effective one to induce change towards safer delivery. In this example of the SCI, the health belief model was used. This model postulates that a person's or community's health-related behaviour depends on his perceived risk of outcome (whether a woman or a family member perceives women at risk for maternal and perinatal deaths if skilled care is not sought during childbirth), his perceived severity of the outcome, the perceived benefits of engaging in preventive action and the perceived barriers to taking that action. The model also incorporates cues to action and self-efficacy Citation15 and was used for community workshops.
Lastly is the capacity strengthening pillar which refers to facilitating community problem-solving skills towards skilled delivery care. This process improves ownership of activities and includes analysis and prioritisation of community problems and sustainability of agreed upon consensual decisions. An important part in the capacity building pillar is also prompting household to raise funds for possible emergencies and to promote revenue generating activities.
1.2 From concepts to practice: description of the Skilled Care Initiative (SCI) community-based interventions
Burkina Faso is one of the poorest countries in the world, land-locked, situated in the heart of West Africa. Population is of mostly farmers with very low literacy rate (20% nationally but 5–8% in remote and rural areas). The SCI activities in Ouargaye district included strengthening health facilities (functional operating room, drugs and equipment), recruitment and posting of anaesthetists to ensure round the clock access to life saving interventions at district hospitals, upgrade of competencies of health workers in obstetric best practices, referrals (ambulance, wireless phone), refurbishment of infrastructures and electricity with solar panels. These supply side activities covered two-thirds of health facilities within the district as another financial and technical partner (UNFPA) had selected the remaining one-third for similar health facility strengthening. The demand side activities however were built around traditional leaders whose areas of influence are beyond health facility boundaries and ultimately covered the whole district. The main steps for implementing the community-based interventions were a baseline survey, an identification of key influential leaders, mobilisation of stakeholders, BCC and monitoring each of which are briefly described below:
A baseline qualitative survey: This used individual interviews, focus group discussions, immersion and observation to identify community health seeking behaviours, birthing and weaning practices, the social organisation and social networks, cultural community mechanisms of solidarity, locally valued communication channels and key influential leaders, level of their influence and coverage areas. It also provides an identification of barriers and facilitators to skilled care, community taboos and values and an understanding of the balance of power within the community.
The second step was the selection of key influential leaders to be centrepieces of the process of community-based interventions. Indeed, societies, worldwide, are characterised by a political and social organisation to ensure peaceful administration and regulation of the society. In mostly rural communities such as those in Ouargaye district, there were, besides local administrative officials, people that communities valued, trusted and respected more than administrative officials because of their role model, their wisdom and their religious power among others. There were traditional leaders whom communities listened to, obeyed and respected and who managed all administrative and judicial matters within their areas of influence. By obeying these traditional leaders people had a sense of social belonging to the community. Recognising the influence of these traditional leaders and their potential roles for engaging their communities in behavioural change, the SCI community mobilisation strategy selected the most influential ones and developed a participatory approach with them.
The third step was engaging stakeholders. After identifying among the traditional leaders those willing to fully back the community-based interventions, the next step was to engage a limited number of them in the process. It was crucial to start slowly before going to scale. This was done through structured meetings with prominent traditional leaders who, after an identification of main barriers to utilisation of maternal health services and possible solutions, invited their peers and other stakeholders (health professionals, religious leaders, administrative officials, associations) and engaged with them in the process (Box 1).
The fourth step was the implementation of the BCC activities. The low level of utilisation of maternal health services may be related to several factors, some obvious such as distance to health facility, cost, time and other less obvious such as cultural barriers or perceived quality of care. In partnership with community leaders, a number of culturally acceptable activities were developed building on existing societal mechanisms: community workshops, recruitment and posting of community relay agents in all villages of the intervention areas (Box 2), public concerts with traditional singers, theatres and financial schemes to reduce out-of-pocket expenses during emergencies (Box 3).
The fifth step was monitoring of action plans and activities, a structured process that started with a preparatory phase and was followed by sensitisation meetings with communities, elaboration of community action plans, a formal and very symbolic engagement from the leaders to implement the action plans, identification of monitoring indicators and feedback processes (Box 3).
2 Methods
2.1 Context, study design and participants
A baseline survey was conducted in the intervention and comparison districts to assess health indicators, to describe existing interventions and to document barriers and facilitators to skilled care. A detailed description of the context and intervention is presented elsewhere Citation7Citation8Citation9Citation10. A description of the study context was done with regard to health human resources, literacy and fertility rates, antenatal coverage and institutional delivery at baseline, and timing of the different components of skilled care activities in intervention and comparison districts.
A geo-referenced census was conducted from February to May 2006 in the intervention district (Ouargaye) and a comparison district (Diapaga). Further details on the evaluation study design and comparability of districts are presented elsewhere Citation8. Information were collected from all women aged 12–49 with experience of pregnancy in the survey referenced period (2001–2005), on the number of pregnancies, pregnancies lasting more than six months, place of delivery, delivery attendant and foetal/newborn survival during the five years prior to the interview (2001–2005), as well as general census data such as household assets, socio-demographic characteristics of household members (age, sex, occupation, education, marital status, etc.). In this study, maternal death was defined as a death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death. This is a time-of-death definition of maternal death, referred to as pregnancy-related death. Perinatal death was defined as stillbirth or death of a newborn less than a month. Caveats of using these operational definitions and an unprecedented five year recall census (misclassification, underreporting and recall bias) have been extensively discussed elsewhere Citation8.
2.2 Data analysis
Description of components of skilled attendance by year Citation7 was done over the reference study period 2001–2005 in intervention and comparison districts. Descriptive statistics were used to compare percentages of deliveries in health institutions, maternal mortality ratio and perinatal death rates between the intervention district (Ouargaye) and the comparison district (Diapaga), and before (2002–2003) and after (2004–2005) implementation of the demand-driven interventions of the SCI. In addition, a multivariate analysis was used to assess differentials in maternal and perinatal mortality risk by maternal age, distance from household to nearest health facility, educational level of mothers, household wealth quintiles and by district.
3 Results
3.1 Context and timing of skilled attendance activities in Ouargaye and Diapaga
The intervention (Ouargaye) and comparison (Diapaga) districts are remote and rural districts located in Centre East Region and lacked running water, serviceable roads and an effective transport system. Prior to the SCI, the mean coverage radius of health centres, ratio of physicians to population and ratio of nurses to population were 11 and 16 km, one for 213,000 inhabitants and one for 134,000 inhabitants, and one for 8,300 inhabitants and one for 6,400 inhabitants, respectively, in Ouargaye and Diapaga. Similarly, the fertility rate, the literacy rate, the antenatal care coverage and institutional delivery were, respectively, 7.5 and 6.0%, 21.7 and 18.6%, 63 and 62%, and 18.0 and 24.4% in Ouargaye and Diapaga districts Citation8.
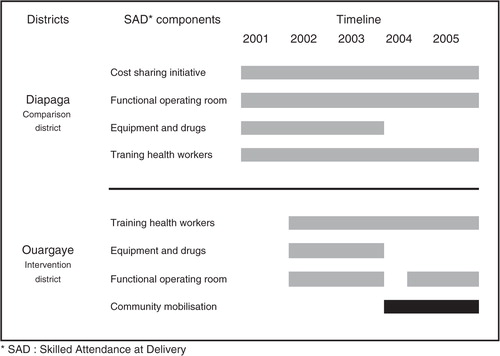
As shown in , there are similarities between Ouargaye and Diapaga districts in terms of strengthening health facilities, access to life saving interventions at district hospitals and capacity strengthening for health workers. The main differences are on demand side activities: there was a community-based cost sharing initiative for emergencies and a radio service that the district management used to broadcast weekly sensitisation message to community on reproductive health in comparison district whilst in the intervention district there was more comprehensive and more intensive community mobilisation (cost sharing initiative for emergencies, advocacy and awareness, BCC and community capacity strengthening). This investment in communities through an understanding of their social structure and health seeking behaviours, through identification and partnership with credible community leaders, and through identification of culturally sensitive and locally acceptable approaches to address transport and referrals was the single significant difference between the two districts.
Figure 3. Timing of supply and demand-side interventions of skilled attendance at delivery in Ouargaye and Diapaga, Burkina Faso, 2001–2005.
3.2 Effects of the Skilled Care Initiative (SCI) community mobilisation on institutional births
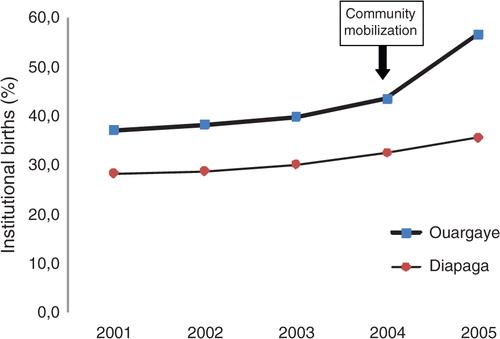
Births in the comparison district were much less likely to be institutional than births in intervention district. Although institutional delivery increased over time in both districts, and although there was a difference at baseline, it significantly increased over time (p<0.001) in both intervention and comparison districts and there was a remarkable and statistically significant 30% increase in intervention district following the implementation of community mobilisation activities compared to 10% increase in Diapaga over the same period ().
Figure 4. Trends of institutional births in Ouragaye and Diapaga, Burkina Faso, 2001–2005.
3.3 Effects of the Skilled Care Initiative (SCI) community mobilisation on pregnancy related mortality
There was a 31.5% reduction in maternal mortality ratios between the period before and after the community mobilisation in intervention district compared with 15.8% reduction in Diapaga. Although maternal mortality ratios decreased over time in both districts, and although there was a difference between intervention and comparison districts before the community mobilisation, the maternal mortality ratio decreased to a greater extent in Ouargaye compared to Diapaga ().
Table 1. Mortality ratios in Diapaga and Ouargaye districts, Burkina Faso, 2002–2005
3.4 Effects of the Skilled Care Initiative (SCI) community mobilisation on perinatal mortality
A logistic regression was used to assess the risk for perinatal mortality per district and per SCI areas within the intervention district (). In 2005, the perinatal mortality rates were 27.5 and 33 per 1,000 live birth in Ouargaye and Diapaga, respectively (OR = 0.75, CI 0.70–0.80). Similarly, the perinatal mortality rates were 26 and 31.3 per 1,000 live birth in areas covered by SCI supply component versus areas not covered in Ouargaye district, respectively (OR = 0.72, CI 0.68–0.77). These differences persist even after adjusting for maternal age, distance from household to nearest health centre, household assets ownership and place of delivery.
Table 2. Multivariate analysis of perinatal mortality risk in Ouargaye and Diapaga districts, 2001–2005
Table 3. Box 1. Steps in engaging a community leader, SCI community mobilisation strategy, Ouargaye district, Burkina Faso.
Table 4. Box 2. Community relay workers (CRW), Skilled Care Initiative, Ouargaye district, Burkina Faso.
Table 5. Box 3. Steps of a community workshop, SCI community mobilisation strategy, Ouargaye district, Burkina Faso.
4 Discussion
An analysis of the contexts in intervention and comparison districts before, during and after the SCI points to associations between community-driven interventions, increases in institutional births and reductions in maternal and perinatal deaths in Ouargaye district compared to Diapaga district. Although this temporal relationship is not sufficient for attributing cause, the comparability of context and socio-demographic profile in both districts Citation8, and the similarities of maternal and child health indicators before the SCI, and of skilled attendance at delivery interventions with the exception of a comprehensive demand-driven interventions in Ouargaye district have empirically led us to the conclusion that community mobilisation was a major contributing factor to the changes observed. These results have also shed some light on configuration and timing of skilled attendance at delivery components. Upgrading health facilities, training health personnel and ensuring availability and quality of life saving interventions are requirements for access to skilled care, but uptake of care and effectiveness could not be achieved without comprehensive demand-driven interventions. Not only is there an equal importance of both supply and demand-led interventions, but the results indicate that a comprehensive framework for demand-driven activities is needed as opposed to selective community based activities such as the case in the comparison district. Although there is no magic bullet, nor a one-size-fits-all ideal community mobilisation approach, closely working with communities by consulting them at all stages of design, planning and implementation of delivery care is critical for achieving reduction in maternal and perinatal mortality. This will require from maternal and child health policy makers and programme managers a comprehensive policy () in working with communities for surveillance, measurements of maternal and newborn adverse outcomes, as well as policy and strategies.
5 Conclusion
Although skilled attendance at delivery is widely regarded as the main strategy to reduce maternal and perinatal deaths, there is less certainty on the optimal configurations of interventions and timing for different health system contexts in order to achieve ultimate health gains. This evaluation demonstrates that reaching reductions in maternal and perinatal mortality requires an adequate coverage of life saving interventions and quality of care, but should be equally met with an investment in community mobilisation. In poorest communities such as Burkina Faso, working in partnership with communities using a comprehensive approach may accelerate progress towards reductions in maternal and perinatal mortality. These demand-driven interventions require an understanding the social structure of local contexts, the political and cultural logic of power, participation and ownership of the process (hence communities not empty vessels) for a successful behavioural change strategy towards skilled delivery.
Acknowledgements
The authors would like to thank Celestin Pouya and Ann Fitzmaurice for their contributions in data analysis, Professor Wendy Graham for reviewing the paper, Immpact and Family Care International teams for this collaborative evaluation. This work was undertaken as part of Immpact, funded by the Bill & Melinda Gates Foundation, the UK Department for International Development, the European Commission and USAID. Immpact is an international research programme (website: www.immpact-international.org) which also provides technical assistance through its affiliate organisation, Ipact. The funders and the reviewers have no responsibility for the information provided or views expressed in this paper. The views expressed herein are solely those of the authors.
Related Research Data
References
- Costello A, Osrin D, Manandhar D. Reducing maternal and neonatal mortality in the poorest communities. BMJ. 2004; 329: 1166–8. 10.3402/gha.v2i0.1947.
- Bolam A, Manandhar DS, Shrestha P, Ellis M, Costello AM. The effects of postnatal health education for mothers on infant care and family planning practices in Nepal: a randomized controlled trial. BMJ. 1998; 316: 805–11.
- Emond A, Pollock J, Da Costa N, Maranhao T, Macedo A. The effectiveness of community-based interventions to improve maternal and infant health in the Northeast of Brazil. Pan Am J Public Health. 2002; 12: 101–10.
- Rogo KO, Bohmer L, Ombaka C. Developing community-based strategies to decrease maternal morbidity and mortality due to unsafe abortion: pre-intervention report. East Afr Med J. 1999; 76: S1–71.
- Shefner-Rogers CL, Sood S. Involving husbands in safe motherhood: effects of the SUAMI SIAGA campaign in Indonesia. J Health Commun. 2004; 9: 233–58. 10.3402/gha.v2i0.1947.
- Kandeh HB, Leigh B, Kanu MS, Kuteh M, Bangura J, Seisay AL. Community motivators promote use of emergency obstetric services in rural Sierra Leone. The Freetown/Makeni PMM Team. Int J Gynaecol Obstet. 1997; 59: S209–18. 10.3402/gha.v2i0.1947.
- Graham W, Themmen E, Bassane B, Meda N, De Brouwere V. Evaluating skilled care at delivery in Burkina Faso: principles and practice. Trop Med & Int Health. 2008; 13: 6–13.
- Hounton S, Sombié I, Meda N, Bassane B, Byass P, Stanton C, et al.. Methods for evaluating effectiveness and cost-effectiveness of a Skilled Care Initiative in rural Burkina Faso. Trop Med Int Health. 2008; 13: 14–24.
- Hounton S, Chapman G, Menten J, De Brouwere V, Ensor T, Sombié I, et al.. Accessibility and utilisation of maternity care within a Skilled Care Initiative in rural Burkina Faso. Trop Med Int Health. 2008; 13: 44–52.
- Hounton S, Menten J, Ouédraogo M, Dubourg D, Meda N, Ronsmans C. Effects of a Skilled Care Initiative on pregnancy-related mortality in rural Burkina Faso. Trop Med Int Health. 2008; 13: 53–60.
- Ouoba D, Congo Z, Diop NJ, Melching M, Banza B. Experience from a community based education program in Burkina Faso, the Tostan Program.. WashingtonDC: Population Council, Frontiers in Reproductive Health. 2004, p. 62.
- Moran AC, Sangli G, Dineen R, Rawlins B, Yameogo M, Banza B. Birth preparedness for maternal health: findings from Koupela district, Burkina Faso. J Health Popul Nutr. 2006; 24: 489–97.
- Stanton CK. Methodological issues in the measurement of birth preparedness in support of safe motherhood. Eval Rev. 2004; 28: 179–200. 10.3402/gha.v2i0.1947.
- Coreil J, Bryant CA, Henderson JN. Social and behavioral foundations of public health. Sage Publications. California, 2001
- Hounton S, Carabin H, Henderson N. Towards an understanding of barriers to condom use in rural Benin using the Health Belief Model: a cross sectional survey. BMC Public Health. 2005; 5: 8.10.3402/gha.v2i0.1947.