Background
Chronic non-communicable diseases (NCDs) are the leading cause of morbidity, mortality, and disability worldwide. More than 80% of chronic disease deaths occur in low-income and middle-income countries. Epidemiological data on the burden of chronic NCD and the risk factors which predict them are lacking in most low-income countries. The INDEPTH Network (http://www.indepth-network.org) which includes the Health and Demographic Surveillance System (HDSS) with many surveillance sites in low-middle income countries provided an opportunity to establish surveillance of the major chronic NCD risk factors in 2005 using a standardised approach.
Objective
This paper presents the conceptual framework and research design of the chronic NCD risk factor surveillance within nine rural INDEPTH HDSS settings in Asia.
Methods
This multi-site study was designed as a baseline cross-sectional survey with sufficient sample size to measure trends over time. In each of nine HDSS sites in five Asian countries, a sample of 2,000 men and women aged 25–64 years, using the WHO STEPwise approach to Surveillance (http://who.int/chp/steps), was selected using stratified random sampling (in each 10-year interval) from the HDSS sampling frame.
Results
A total of 18,494 men and women from the nine sites were interviewed with an overall response rate of 98%. The major NCDs risk factors included self-reported information on tobacco and alcohol consumption, fruit and vegetable intake, physical activity patterns, and measured body weight, height, waist circumference, and blood pressure. A series of training sessions were conducted for research scientists, supervisors, and surveyors in each site. Data quality was ensured through spot check, re-check, and data validation procedures, including accuracy and completeness of data obtained. Standardised data entry programme, created using the EPIDATA software, was used to ensure uniform database structure across sites. The data merging and analysis were done using STATA Version 10.
Conclusion
This multi-site study confirmed the feasibility of conducting chronic NCD risk factor surveillance in the low and middle-income settings by integrating the chronic NCDs risk factor surveillance into an existing HDSS data collection and management setting. This collaborative work has provided reliable epidemiological data as a basis for developing chronic NCD prevention and control activities.
Introduction
Chronic non-communicable diseases (NCDs), including heart disease, stroke, diabetes, cancer, and chronic obstructive pulmonary disease (COPD), have become the leading cause of morbidity, mortality, and disability worldwide. Chronic NCDs accounted for 60% of global death in 2005, including cardiovascular diseases and diabetes (32%), cancers (13%), and COPD (7%) Citation1. Of concern, available data suggests that the burden of chronic NCD is greater in low and middle-income countries than that in high-income countries Citation2. More than 80% of the 5.9 million deaths in 2005 occurred in low-income and middle-income countries where resources allocated for prevention and control of NCD are scarce Citation1.
The myth that chronic NCDs are ‘diseases of affluence,’ has led health authorities, particularly in low and middle-income countries, to be unaware of this threatening burden of chronic NCDs which is largely driven by the aging of populations and changing of the lifestyles. Globally, health budgets allocated for chronic NCD prevention and control are insufficient. The misguided belief that interventions for chronic NCD prevention and control are less cost-effective than those for acute infectious diseases discourages health authorities from investing in chronic NCD prevention Citation2. Most chronic diseases are caused by a few modifiable risk factors (tobacco use, unhealthy diet, and lack of physical activity) that can be prevented and controlled with existing cost-effective interventions Citation3.
To date, most chronic diseases surveillance systems have been conducted in high-income countries, among which are: the World Health Organization (WHO) MONICA (MONItoring of trend and determinants in CArdiovascular diseases) Project which measured the trends and determinants in CVD mortality and cerebrovascular disease morbidity across populations in 21 countries, mainly in Europe Citation4, the Framingham Heart Study in the USA, which started in 1948 and has since contributed to a huge body of knowledge on CVD risk factors from the so-called ‘classical risk factors’ such as cigarette smoking, high blood cholesterol level, and high blood pressure, to the emerging risk factors, such as homocysteine, lipoprotein A, and apolipoprotein E, as well as to the study of chromosomes and genes Citation5, and the Västerbotten Intervention programme, which started in Västerbotten County, Sweden in 1990 and has since delivered intervention in reducing chronic disease risk factors among people aged 40, 50, and 60 years old Citation6. Surveillance on chronic disease requires ongoing commitment in order to measure trends and can be resource-demanding. Ideally, chronic disease surveillance requires population level data on morbidity and mortality patterns. Measuring the incidence of most chronic diseases, except perhaps for stroke which is based on a clinical definition, often requires diagnostic techniques which are not readily available. Few low and middle-income countries have adequate death registration systems. The surveillance of chronic NCD risk factors, which is less technological and resource intensive, is more feasible in low-middle income countries compared with disease surveillance. From a public health point of view, the surveillance of risk factors is more justifiable for two reasons. Firstly, current trends in risk factor status can predict future disease patterns, and secondly, most chronic disease can be explained by a few modifiable risk factors Citation7. Prevention is the key to controlling the increasing burden of chronic disease and this in turn will have a favorable impact on national development.
Efforts also need to be strengthened to provide high-quality epidemiological data in order to understand the unfolding epidemiological transition. In most low-income countries where population registration is not well-established, the majority of demographic events occur unregistered Citation8. During the last few decades, efforts and resources have been invested in strengthening the demographic surveillance and surveillance of major communicable diseases such as malaria, HIV/TB, and tuberculosis. Health and Demographic Surveillance Systems (HDSSs) have been established in different countries as platforms to monitor population dynamics. In 1998, the INDEPTH Network (an International Network of field sites for continuous Demographic Evaluation of Populations and Their Health in developing countries; www.indepth-network.org) was founded to facilitate linkage of existing HDSSs through a focused network Citation9. The network has since expanded their focus from HIV/AIDS and malaria to include adult health and aging and NCD. In recognition of the changing patterns of the burden of disease, at its 10th anniversary in 2008, the INDEPTH Network reaffirmed its commitment to develop its capacity and strengthen its effort from knowledge generation to improved health policy and practice.
Lack of high-quality epidemiological data on the chronic NCDs burden and the major risk factors that give rise to them is a barrier when advocating that health authorities should invest resources in chronic NCD prevention and control. Epidemiological data is also required so that interventions for chronic NCDs and their risk factors can be evaluated. The paper presents the development of chronic NCDs risk factor surveillance within the HDSS settings in Asia, and discusses the potential of HDSS to provide accurate and timely epidemiological data as the basis of chronic NCDs prevention and control policies.
2 The INDEPTH Network
Lack of vital statistics, lack of representative data at the population level, poor data quality control, and lack of comparable data are among concerns when dealing with data from low-middle income countries. Low priority is given to chronic disease surveillance in national health systems, including morbidity, mortality, and risk factor surveillance. Surveillance is ‘the tool underpinning health promotion and disease prevention efforts and it is a fundamental, but often neglected, component of public health practice’ Citation10. For low and middle-income countries, vital registration is often the starting point in fieldwork Citation11. HDSS established in different countries are used to monitor population dynamics and to test and evaluate various health interventions to promote population health. To date, 34 HDSSs in 17 different countries, scattered in Africa (23 sites), Asia (10 sites), and Oceania (one site), are participating in the INDEPTH Network (9).
An initial census defines and registers the target population in each of the HDSS. Regular subsequent rounds of data collection are carried out to register all new individuals, households and residential units, and to update key variables and attributes of existing subjects. This core system provides information on population dynamics. In addition, complementary data covering health, social, and economic indicators, are occasionally collected. Regular core data collection maintains accurate denominators for estimation of age, sex, and cause-specific death rates Citation9.
The INDEPTH Network mostly covers countries in low and middle income countries where data on chronic disease risk factors are still lacking. These countries are also experiencing different stages of demographic, economic, and epidemiological transitions. Therefore the HDSS creates an opportunity to provide insights into the epidemiological transition processes in countries with different levels of economic development. The well-established population in the HDSS also creates the possibility of monitoring risk factor changes over time, and thus offers an opportunity to evaluate the effectiveness of community interventions conducted within the HDSS Citation12.
3 Methods – chronic non-communicable disease (NCD) risk factor surveillance in INDEPTH Health and Demographic Surveillance System (HDSS)
3.1 Study setting, study population, and sampling
The study, upon which this series of papers is based, was designed as a multi-site cross-sectional survey. The purpose was to provide baseline data for the chronic NCD risk factors burden in these defined populations. The studies were conducted during June–November 2005 in all nine Asian HDSS within the INDEPTH Network. The HDSSs, which are all in rural settings, cover a representative sample of population at a district level. The HDSSs are, however, self-selected, and therefore do not necessarily represent the entire region or country. outlines differences in the population structure of each district from which the HDSS was established and the number of men and women included in the risk factor survey.
Table 1. Population distribution in the nine rural INDEPTH HDSS and the risk factor survey
The study was conducted among adult men and women aged 25–64 years. In each HDSS site, a sample of 250 individuals was randomly selected in each sex and 10-year age interval strata from the HDSS sampling frame. More than one individual can be selected from each household. The following assumptions were used for sample size calculation: level of confidence 95%; margin of error 6%; baseline level of risk factors 35%; and expected response rate 95%. Sampling probability weights were used to ensure representativeness of statistics generated from this study to the HDSS population. The weight was obtained as proportion of study sample in each sex and 10 years age group to each HDSS population in the same group.
3.2 Instruments and measurement
3.2.1 Demographic information
Basic demographic information, such as age, sex, and education achievement, were extracted from the HDSS databases for each of the selected participants. The information on highest education level achieved is used as a proxy of socio-economic status. We used four standard education categories for further analysis, and these included: Citation1 no schooling or not graduated from primary school (equivalent to less than six years of education); Citation2 graduated from primary school (at least six years of education); Citation3 graduated from secondary school (at least nine years of education); and Citation4 graduated from high school or university (at least 12 years of education).
The modules for each of the key risk factors were based on the WHO STEPwise approach to Surveillance (STEPS) for NCDs risk factors Citation7 Citation13 Citation14 Citation15 . STEPS uses different levels of risk factor assessment of increasing complexity and cost, including collecting information using questionnaires (Step 1), taking physical measurements (Step 2), and taking blood samples for biochemical assessment (Step 3). Each step contains core, expanded, and optional items that can be added as needed and as resources allow Citation7. This study utilised the core and some expanded items of Steps 1 and 2. The risk factors collected and analysed in this study included self-reported tobacco use, alcohol use, fruit and vegetable consumption, physical activity patterns, and measured body weight, height, waist circumference, and blood pressure( Citation16 Citation17 Citation18 Citation19 Citation20 Citation21 Citation22 ).
3.2.2 Tobacco use
The core questions on tobacco use assess current and current daily tobacco users. For those who smoked daily, information on the age at which the respondent started smoking and the types and number of tobacco products smoked each day were also collected. Smokers were defined as those who smoked manufactured, hand-rolled cigarettes, cigars, cheroots, cigarillos, or pipes full of tobacco. The optional module on smokeless tobacco, relevant for the sites selected for this survey, provided information on the proportion of current and current daily smokeless tobacco users or chewers. Chewers were defined as those who chewed betel leaf with sliced betel nut or areca nut and slaked lime, or those who placed sun dried tobacco leaf with slaked lime on the gum, or those who snuffed tobacco.
3.2.3 Alcohol use
Alcohol use was defined as consumption of alcoholic drinks such as beer, wine, spirit, as well as other local drinks such as arak or tuak in Indonesia, ruou gao in Vietnam, sonti in India, and Satoh, Ou, and Krauche in Thailand. Lifetime abstainers were defined as those who had never consumed any alcoholic drink. Respondents were asked about the number of standard drinks of alcohol consumed in each of the last seven days. A show card which has been tailored to show various local alcoholic drinks were shown to the respondents. The numbers of local drink consumed were later standardised across sites. Respondents who engaged in heavy episodic drinking were men who had five or more drinks or women who had four or more drinks on any day in the past 30 days.
3.2.4 Fruit and vegetable consumption
The core module on fruit and vegetable consumption included information on the number of days fruits and vegetables were consumed in a typical week in the last year, as well as the number of servings of fruit/vegetable consumed in one of those days. Respondents were shown a show card with different local fruits and vegetables, with the size of a serving. The size of the serving referred to in the show cards were calibrated across sites. Those who ate less than five servings of fruit and/or vegetables on average per day were defined as those with did not meet fruit/vegetable consumption recommendation.
3.2.5 Physical activity patterns
The physical activity was measured using the Global Physical Activity Questionnaire Version 2/GPAQ2 (15). GPAQ assesses: Citation1 physical activity in three different domains (work, transport, and leisure time); as well as Citation2 sitting time. The interviewer read introductory statements, which explain what is meant by vigorous and moderate activities, to respondents. The respondents were asked to detail time spent in a typical week on: Citation1 vigorous and moderate activities at work; Citation2 vigorous and moderate activities during recreational/leisure time activities; and Citation3 activities when travel to and from places. Vigorous activities were defined as those that required hard physical effort and caused large increases in breathing or heart rate. Respondents were asked to only consider activities for 10 minutes or more. Information on the number of days in a week spent and time spent in a typical day for each activity were recorded. Time spent sitting or reclining, either at work, at home, or on travel, excluding sleeping time, on a typical day was gathered. Show cards of various local physical activities were developed and shown to the respondents during interview.
The following individuals were excluded from the physical activity analysis: those who reported activities for at least one sub-domain more than 16 hours per day; those who reported more than seven days of activity in a week; and those who reported minutes spent on activities following a zero day of conducting activity. Activities less than 10 minutes were recorded as missing data. All durations were converted to minutes. In addition to the total minutes of activity, the activity volume was also computed by weighting each type of activity by its energy requirement in metabolic equivalents (METs). One MET is defined as the energy cost of sitting quietly, and is equivalent to a caloric consumption of 1 kcal/kg/hour. A MET minute showed the total activity volume on weekly basis, and calculated by multiplying time spent on each activity during a week by the MET values of each level of activity. MET values for different activities level were established based on the Compendium of Physical Activities and were set as four MET for moderate-intensity physical activity, eight MET for vigorous physical activity, and four MET for transport-related walking or cycling. The total activity for GPAQ was calculated as the sum of total moderate, vigorous, and transport-related activities per week. The number of days and total physical activity MET minutes per week were used to classify respondents into three categories of low (less than 600 MET minutes per week), moderate, and high level (over 3,000 MET minutes per week) of physical activities Citation15.
3.2.6 Body mass index (BMI)
Weight and height were measured with the participant wearing lightweight clothing and standing barefoot on instruments placed on a flat surface. Weight was measured to the nearest 10 grams using an electronic scale (Seca Gmbh, Hamburg, Germany). These scales were purchased centrally and provided to each of the participating HDSS during the training course. Height was measured to the nearest 0.1 cm using a portable stadiometer. Body mass index (BMI) was calculated as weight in kilograms divided by height in metres squared. Participants were classified as being overweight or obese if they had a BMI ≥25. We defined obese participants as those who had a BMI ≥30. Waist circumferences were measured using non-elastic tape (Seca Gmbh, Hamburg, Germany) to the nearest 0.1 cm; these tapes were purchased centrally and provided to each of the participating HDSS during the training course. Waist circumference was measured at the midpoint between the lower margin of the last rib and the top of the hip bone at the end of expiration, with the measuring tape put at umbilicus level.
3.2.7 Blood pressure
Blood pressure was measured using digital blood pressure measurement device (Omron M4-I, Omron Healthcare Europe BV, Hoofddorp, the Netherlands). These devices were purchased centrally and provided to each of the participating HDSS during the training course. Blood pressure was measured at the right arm at heart level after a period of 10 minutes of rest following the STEPS methods, three measurements were taken and the averages of the last two readings were used in the analysis. Raised blood pressure was defined as those with systolic blood pressure ≥140 mmHg and/or diastolic pressure ≥90 mmHg, or under any anti-hypertensive drugs medication. More detailed analyses are undertaken to compare the burden of raised blood pressure by excluding treatment with anti-hypertension drugs from the definition to explore the impact of different treatment patterns across the sites.
3.2.8 Data collection and quality control
The questionnaires were translated into local language, and back-translated into English to ensure its validity. Instruments for anthropological and blood pressure measurements were standardised and calibrated routinely in the field in each HDSS. To ensure high quality of data, the group conducted several training sessions. In February 2005, the principal investigators of the selected HDSS met in Ballabgarh HDSS, India, to discuss and finalise the research protocol and instruments. Discussion focused on the adaptation of the WHO STEPS instrument to respective sites’ settings while maintaining comparability of expected results. A show card for standard alcoholic drinks was developed to ensure the comparability of alcoholic drinks measured. A show card for different local fruits and vegetables available, as well as different local physical activities were also developed for similar reasons. In May 2005, each HDSS organised several trainings for field data collectors and supervisors. In each training workshop, the standardised study protocol and instruments were discussed thoroughly, and data collectors conducted pilot tests of both interviews using the standardised questionnaire as well as of physical measurements. During the data collection period, field supervisors conducted regular spot checks, re-checks and data validation procedures to ensure the accuracy and completeness of data obtained. Weekly field meetings were held to enable researchers, supervisors, and surveyors to identify and discuss problems encountered during the data collection processes. Completed questionnaires were sent to the data entry manager.
3.2.9 Data management and analysis
A standardized data entry programme using EPIDATA software was used in each site for data entry to ensure uniform database structure across sites. In some sites, additional questionnaires were employed, and sites updated their database structure accordingly but kept the common core STEP data structure intact. Plausible values for each variable were set in the data entry programme to prevent any possible mistakes during data entry process. Double entry for 10% of data was also done in each site. Each site was responsible for cleaning their data, and the cleaned data was sent to the group coordinator. The site data were later merged into a cross-site dataset to facilitate further cross-site analysis. Further cleaning process of outliers were undertaken in the pooled data, and uniform indicators on various risk factors (for example, variables on the level of physical activity or overweight, etc.) were developed for all sites to ensure consistency and comparability. Following the WHO STEPS model, we also constructed a new variable for combined risk factors, which showed the clustering of the following risk factors: current daily smokers, less than five servings of fruits and vegetables per day, low level of physical activity, overweight, and raised blood pressure. The data merging and pooled analysis were done centrally by the group coordinator using STATA Version 10.
All analyses were stratified by sex and adjusted for age. All categorical risk factors were presented as proportion in percentages with their 95% confidence interval (CI). The mean values of all continuous risk factors were also presented with their 95% CI. We complied with the WHO STEPS reporting format in preparing the descriptive section of the papers, which mainly show the proportion of study subject with risk factors with its 95% CI, or the mean value of risk factors with their 95% CI Citation7.
3.2.10 Ethical consideration
Ethical approval was obtained from the Ethical Committee in each HDSS site. Prior to sharing their data for merging, each site removed individual identification from their database to ensure confidentiality of the data. The merged file was then shared among the sites based on the cross-site data sharing agreement.
4 Results
A total of 18,932 individuals were randomly selected from the nine HDSSs sampling frame. A total of 18,494 individuals were successfully interviewed, a pooled response rate of 98% (ranging from 95% in Matlab HDSS, Chililab HDSS, and Purworejo HDSS to 100% in Kanchanaburi HDSS). A high response rate for this study, taking into consideration that it was embedded in a well-functioning HDSS, has been expected. Only less than 1% of data (65 individuals) were lost due to cleaning.
Respondents from HDSSs in Vietnam, Thailand, and Indonesia had higher education level compared to those from Bangladesh and India. Overall, men had higher level of education than women. These discrepancies were prominent in Bangladesh, where less than 7% of women had ever attended high school or university (). In many of these countries, education was not compulsory until the last two decades; level of education has been used in many HDSSs in measuring socio-economic status of the population. A significant proportion of study subjects had no schooling experience, and did not even finish their primary school, and this group of population was regarded as the least favorable group in terms of socio-economic development.
Table 2. Education level of participants in the risk factor survey in nine rural INDEPTH HDSS
This study showed that chronic NCDs risk factors were prevalent in most HDSS sites (). Smoking was prevalent among men in all HDSSs, and chewing was also common among women and men in HDSSs in Bangladesh and India. Overweight was also a significant public health issue particularly among women in most HDSSs, with an overall 13% of women in this study were overweight. In both Purworejo HDSS (Indonesia) and Kanchanaburi HDSS (Thailand), the proportions of overweight women have reached 25 and 44%, respectively. About 22% of the people have raised blood pressure, and there were no significant differences observed between men and women. A detailed analysis of each risk factor will be presented in subsequent papers in this series Citation16 Citation17 Citation18 Citation19 Citation20 Citation21 Citation22 .
Table 3. Prevalence of five major behavioural and biological risk factors (95% CI) adjusted by sex and age group in nine Asian HDSS sites
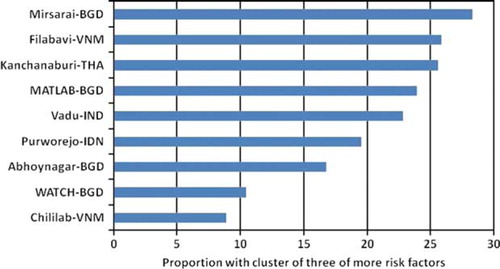
Overall, 20% of study subject had three or more risk factors (either smoking, low physical activity, overweight, raised blood pressure, or consumption of fruits and vegetables less than five servings per day). The proportion of risk factors clustering ranged from 9% in Chililab Vietnam to 28.3% in Mirsarai HDSS in Bangladesh (). Consumption of fruits and vegetables less than recommended was the main problem in many of the sites, and in WATCH HDSS in Bangladesh, all respondents did not meet the recommendation. About one in four of the respondents in Filabavi HDSS, Vietnam, had a number of risk factors; if heavy alcohol use were included, the proportion with risk factors cluster will surge because of the high alcohol consumption among Vietnamese men.
Figure 1. Cluster of risk factors in nine rural Asian HDSS sites.
5 Discussion
5.1 Main findings
The rural settings of HDSS within the INDEPTH Network are not spared from the chronic NCDs risk factor burden. This study shows that most of the chronic NCDs risk factors, in particular smoking among men, tobacco chewing among women, overweight among women, lack of physical activity, and consumption of fruit and vegetable below the recommendation levels, are prevalent in most of the HDSSs. Even though the risk factor burdens were more prevalent among respondents in older age group, we also observe a significant burden of these risk factors among young productive age groups below 55 years old. By using educational level as a socio-economic indicator, we observed that risk factor burdens are borne by all economic groups. Evidence from this study, which showed the existence of chronic NCDs risk factor burden in all economic and age-groups in men and women; suggest that chronic diseases do not mainly affect high-income countries, rich people, old people, and men Citation2.
6 Strengths of the study
This study demonstrates the added value of integrating the chronic NCDs risk factor surveillance into a well-functioning HDSS setting. Availability of a reliable sampling frame, established mutual trust, and good relationships between the researchers and the study respondents over time, possibilities of linking the risk factor data with other health and demographic data available in the HDSS, are among the advantages of integrating risk factor surveillance into HDSS routine operation from time to time Citation12.
Existing surveillance databases in each HDSS provides reliable sampling frame for the study subject selection, and it allows for random selection of a certain number of study subjects within each age-group strata. Availability of a sampling frame is a main constraint when conducting health surveys in low-middle income countries where vital registration systems are not well-developed. With the regular update of demographic events in the population under surveillance, the HDSS is able to catch the dynamics of its finite population, and therefore continuously have up-to-date and reliable sampling frame for conducting surveys and other epidemiological studies.
This collaborative work is among the first research collaborations within the INDEPTH Network utilising uniform study protocols and standardised instruments to achieve consistent and comparable research results across sites. Efforts to produce a global data repository on chronic NCDs risk factors are hampered by the lack of comparability of surveys done across different countries and across different times within the same country. Methodologies, sample sizes, and age groups differ; different questions and instruments to assess risk factors are used Citation23.
Integrating the risk factor surveys within an ongoing demographic surveillance in a finite population enhances the possibility of obtaining a better response rate in the study, thus a result with higher internal and external validity. Embedding this research into the ongoing surveillance mechanism ensures appropriate feedback to the study population through established dissemination channel built within the surveillance system in each site. Dissemination of chronic NCDs risk factor information to general population is an important step in raising public awareness and providing education to the public on chronic NCDs and putting forward the agenda for chronic NCDs risk factor prevention and control more visible and sustainable in the population Citation24.
The WHO STEPwise approach was developed to address the need for standardised data on a few key risk factors to allow countries to have small amounts of good quality data for comparison between and within countries, but also to have sufficient power to measure trends in these risk factors over time Citation7. The STEPS approach has been developed as a simple hierarchical system which allows some flexibility while maintaining comparability of core items over time and between countries Citation13. It has been constructed in such a way that add-on modules can be built into the information package to capture, on a population basis, emerging chronic disease risk factor patterns. In this study, we developed the STEPS baseline survey as part of the ongoing HDSSs routine surveillance at district level. Access to the HDSS has facilitated building reliable chronic NCD risk factors surveillance within the INDEPTH Network, with the plan to conduct a further cross-sectional survey in 2010 to measure changes over time. The use of standardised modules within this surveillance system, and adherence to minimum age and sex sampling, allows the assessment of risk factors trends over time.
This multi-site study also acts as an example of south–south research collaboration within the INDEPTH Network, and an extension of north–south–south collaboration through communication and networks built to assist researchers build knowledge and skills in conducting chronic NCDs surveillance. This work should also be extended to INDEPTH sites in Africa, as chronic NCDs have become an imminent public health threat to the population in Sub-Saharan Africa as well Citation25. The multi-site study has also been an example of developing leadership capacity at all levels, gaining strong support from the community, and widening the network in achieving a successful chronic disease control programme Citation26. This collaborative study brings prospective researchers from developing countries together and the INDEPTH Network provides vast opportunities for this group to interact with other networks working in this field, such as the Oxford Health Alliance (OxHA; Citation27), or the Bloomberg Initiative for tobacco control Citation28.
This study opens the opportunity to build capacity and to develop leadership capacity in the field of chronic NCDs risk factor surveillance. The research team in this study includes researchers with different scientific backgrounds, i.e. epidemiologist and biostatisticians who contribute to study design and instrument developments, anthropologist and social scientist whose knowledge and expertise become the backbone in developing qualitative studies in identifying socio-cultural issues of life style and human behaviour related to the risk factors, as well as health promotion specialist whose experiences in developing community interventions in communicable disease control programme can be utilised and adapted to chronic disease control programme development. The development of such multi-disciplinary team in each HDSS setting will allow HDSS's scientists to conduct researches on chronic disease with holistic approach.
Linkage of the core risk factor data with the HDSS database allows the researchers to generate research questions and to test hypothesis relating the risk factors with other demographic and health indicators, such as migration, socio-economic, health status, physical and cognitive function, etc. This will allow investigators to explore issues in understanding the mechanisms of development and patterns of chronic NCDs risk factors in the study populations. The HDSS can also be a platform to test hypothesis related to local and cultural differences in risk factors, such as diet and physical activity patterns.
7 Limitation of the study
7.1 Representativeness of our results
Despite comparable results across all Asian sites within the INDEPTH Network, chronic NCD risk factors data from the cross-sites study need to be interpreted cautiously. The HDSS which participated in this study were initially developed as a district-level surveillance system in rural settings. It is not possible, therefore, to extrapolate our findings to a larger population at country level. However, findings from our study are in line with most of the findings from other sub-national or national surveys where each HDSS is located Citation23.
7.2 Comparability of results across sites
Most of the risk factors studies are contextually bound, stressing the important contribution of social, political, and cultural factors in shaping individual behaviour related to these risk factors. Differences in physical activity levels across sites should be interpreted with sufficient knowledge concerning agricultural work and occupational patterns, as well as seasonal physical activity patterns in each site. Interpretation of the proportion of population with raised blood pressure should be done carefully by considering differences in health care system and delivery of anti-hypertensive medications in each setting. The lower tobacco use rates in women in many of these Asian countries need to be explored in order to strengthen resistance to aggressive smoking campaigns launched by the tobacco industries in this region in the recent years. Why Asian populations consume little fruit and vegetables despite their vast availability, may need to be explored in a qualitative study to complement the quantitative results obtained in this study. Even though the studies were conducted in all nine HDSSs during the same period of time, potential seasonality impacts on fruit and vegetable intake, and the level of physical activity cannot be ignored. Some of the findings in the subsequent papers will require exploration of socio-cultural factors influencing individual behaviour, as well as potential influences of season on risk factors patterning in each setting. It is also important to understand the population awareness and knowledge on the importance of these risk factors in chronic NCDs prevention and control.
7.3 Methodological considerations
Some of the behavioural risk factors in this study (i.e. tobacco use, alcohol use, and physical activity) were self-reported which might raise questions about the validity of the level of risk factors reported. A systematic review, which assessed the accuracy of self-reported smoking against smoking status determined by biological fluid's cotinine measurement, has reported potential underestimation of self-reported smoking prevalence. However, the review is limited by the different definitions of smoker and different cut-off points of cotinine used across studies, and other unmeasured factors such as types of cigarettes used and metabolisms pattern which might contaminate the study results Citation29. We believe that results of smoking behaviour in our study are valid and the prevalence confirms the level reported in several other surveys in the study settings Citation23. Alcohol consumption is more likely to be underreported, especially in the Muslim HDSS where alcohol use is prohibited by religion, and drinking is not socially accepted. In the data analysis, we did not calculate standardised rates of risk factors; however, we presented proportion of risk factor in each HDSS, adjusted with sampling probability weight.
7.4 Ethical considerations
We faced ethical considerations when identifying the NCD risk factor burden in the community without the ability to provide any sustainable intervention for their long-term control. However, each HDSS worked closely with the governmental health care service providers, for example, primary health care centres in the study area, to whom we referred study subjects who were identified with elevated blood pressure. Elevated blood pressure has been erroneously used as the most common known risk factors to be referred to public health centre. Smoking, alcohol abuse, obesity, and lack of physical activity have not received the same attention, and unfortunately many health care services are not ready to provide behavioral counselling to patients with NCD risk factors. Brief health education was given to each household after all measurements were completed. Even though this might not be an optimal solution in a setting in which chronic diseases prevention and control are not yet prioritised by the government, this is the least the researchers in the HDSSs can do.
8 Implication of the study
This study provides baseline population data on chronic NCDs risk factors which are not readily available in many low-middle income countries. These epidemiological data are of value if presented and used by the health policy maker in developing interventions for chronic disease risk factor prevention and control in respective countries. The study also provides strong evidence that populations in low-middle income countries are not spared from the threatening burden of chronic NCDs risk factor and their future emerging disease burdens. The existence of double burden of diseases in many of these countries should be treated as important pressure to governments in these countries to re-orient their health system and to develop concrete action plans for short-term and long-term chronic disease prevention and control programme Citation2 Citation30 Citation31. If this surveillance is maintained, it will be possible to assess the changes in pattern of risk factors over time, and associate the changes with incidence rates of chronic NCDs.
Effective population-level interventions for primary prevention such as population-based intervention on tobacco control and salt reduction have been showed to be cost-effective in reducing the population level of risk factors in low and middle-income countries Citation32 Citation33. However, the feasibility and the success of such interventions are highly dependent on how the programs are tailored into different socio-cultural–political settings, in order to make the programs credible for policy maker and acceptable by the community in large Citation31. The HDSSs in the INDEPTH Network offer a good platform to develop and to test such interventions within uniquely diverse population in Asia and Africa. HDSS, in addition to their primary purpose, can measure changes in population levels of risk over time, and use them to measure the effectiveness of any population wide intervention for risk factors prevention and control.
4 Conclusion
Linking the core chronic NCDs risk factors data to a multi-site surveillance database allows researchers to test hypothesis on the association between risk factors and different demographic and health indicators. Good quality epidemiological data on chronic NCDs risk factor, supported by an understanding of how individuals and populations adapt with different habits related to chronic NCDs are an essential component in designing appropriate interventions at the population level for preventing and controlling chronic NCDs. This multi-site study builds south–south research collaboration within the INDEPTH Network and it aims in developing leadership capacity at all levels, gaining strong support from the community, and widening the network in achieving a successful chronic disease control programme.
5 Conflict of interest
The authors have no conflict of interest.
Acknowledgements
The authors would like to acknowledge the INDEPTH Network for financing this work, Dr. Anand Krishnan and Dr. S.K. Kapoor from Ballabgarh HDSS for organising training workshop for this project, the Umeå Centre for Global Health Research, Umeå University, Sweden for supporting the coordination of this supplement, and Dr. Ruth Bonita, who as guest editor for this series of papers, provided substantial and critical scientific input into earlier drafts of this paper.
Related Research Data
References
- Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet. 2007; 370: 1929–38.
- World Health Organization. Preventing chronic diseases – a vital investment. Geneva: World Health Organization. 2005.
- Asaria P, Chisholm D, Mathers C, Ezzati M, Beaglehole R. Chronic disease prevention: health effects and financial costs of strategies to reduce salt intake and control tobacco use. Lancet. 2007; 370: 2044–53.
- World Health Organization. MONICA monograph and multimedia sourcebook. Geneva: World Health Organization. 2005.
- National Heart Lung and Blood Institute, Boston University. Framingham Heart Study. Available from: http://www.framinghamheartstudy.org/; 2009. [cited 4 June 2009].
- Weinehall L, Hellsten G, Boman K, Hallmans G. Prevention of cardiovascular disease in Sweden: the Norsjo community intervention programme – motives, methods and intervention components. Scand J Public Health Suppl. 2001; 56: 13–20.
- World Health Organization. WHO STEPS surveillance manual: the WHO STEPwise approach to chronic disease risk factor surveillance. Geneva: World Health Organization. 2005.
- Chandramohan D, Shibuya K, Setel P, Cairncross S, Lopez AD, Murray CJ, et al.. Should data from demographic surveillance systems be made more widely available to researchers?. PLoS Med. 2008; 5: e57.
- INDEPTH Network. Population and health in developing countries. Ottawa: INDEPTH Network, IDRC. 2002.
- Beaglehole R, Bonita R. Challenges for public health in the global context – prevention and surveillance. Scand J Public Health. 2001; 29: 81–3.
- Byass P. Person, place and time – but who, where, and when?. Scand J Public Health. 2001; 29: 84–6.
- Ng N, Van Minh H, Tesfaye F, Bonita R, Byass P, Stenlund H, et al.. Combining risk factors and demographic surveillance: potentials of WHO STEPS and INDEPTH methodologies for assessing epidemiological transition. Scand J Public Health. 2006; 34: 199–208.
- Armstrong T, Bonita R. Capacity building for an integrated noncommunicable disease risk factor surveillance system in developing countries. Ethn Dis. 2003; 13: S13–8.
- Bonita R, Douglas K, Winkelmann R, De Courten M. The WHO STEPwise approach to surveillance (STEPS) of noncommunicable disease risk factors. Global risk factor surveillance. McQueen D, Puska PKluwer Academic/Plenum. London, 2003; 9–12.
- World Health Organization. Global Physical Activity Surveillance. Available from: http://www.who.int/chp/steps/GPAQ/en/index.html; 2009. [cited 4 June 2009].
- Ashraf A, Quaiyum MA, Ng N, Minh HV, Razzaque A, Ahmed SM, et al.. Prevalence of self reported use of tobacco products and their relationship with selected socio-economic characteristics in the Asian region of INDEPTH Network. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- Bich TH, Nga PTQ, Quang LN, Minh HV, Ng N, Juvekar S, et al.. Patterns of alcohol consumption in Asian region and their relationships with socio-demographic status. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- Kanungsukkasem U, Ng N, Minh HV, Razzaque A, Ashraf A, Juvekar S, et al.. Patterns of fruit and vegetable consumption: a multi-site survey in Health And Demographic Surveillance sites in Asia. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- Ng N, Hakimi M, Minh HV, Juvekar S, Razzaque A, Ashraf A, et al.. Prevalence of physical inactivity in nine Health And Demographic Surveillance Systems (HDSSs) in Asia. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- Razzaque A, Nahar L, Minh HV, Ng N, Juvekar S, Ashraf A, et al.. Social factors and overweight: evidence from nine Asian INDEPTH Network sites. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- Minh HV, Soonthornthada K, Ng N, Juvekar S, Razzaque A, Ashraf A, et al.. Patterns of raised blood pressure and, its treatment in nine Health And Demographic Surveillance sites in Asia. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- Ahmed SM, Hadi A, Razzaque A, Ashraf A, Juvekar S, Ng N, et al.. Clustering of chronic NCD risk factors among selected Asian populations: levels and determinants. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- World Health Organization. WHO Global NCD Infobase. Available from: http://www.who.int/ncd_surveillance/infobase/en/; 2009. [cited 30 May 2009].
- Krishnan A, Baridaylne N, Kapoor SK, Pandav CS. A role for INDEPTH Asian sites in knowledge generation and translation for non-communicable disease prevention and control: a case study of Ballabgarh, India. Global Health Action. 2009; Manuscript for INDEPTH NCD Series.
- Tollman SM, Kahn K, Sartorius B, Collinson MA, Clark SJ, Garenne ML. Implications of mortality transition for primary health care in rural South Africa: a population-based surveillance study. Lancet. 2008; 372: 893–901.
- Brownson RC, Bright FS. Chronic disease control in public health practice: looking back and moving forward. Public Health Rep. 2004; 119: 230–8.
- Oxford Health Alliance. Oxford Health Alliance. Available from: www.oxha.org; 2009. [cited 30 May 2009].
- Bloomberg Initiative. Tobacco Control Grants. Available from: http://www.tobaccocontrolgrants.org/; 2009. [cited 30 May 2009].
- Gorber SC, Schofield-Hurwitz S, Hardt J, Levasseur G, Tremblay M. The accuracy of self-reported smoking: a systematic review of the relationship between self-reported and cotinine-assessed smoking status. Nicotine Tob Res. 2009; 11: 12–24.
- Daar AS, Singer PA, Persad DL, Pramming SK, Matthews DR, Beaglehole R, et al.. Grand challenges in chronic non-communicable diseases. Nature. 2007; 450: 494–6.
- Miranda JJ, Kinra S, Casas JP, Davey Smith G, Ebrahim S. Non-communicable diseases in low- and middle-income countries: context, determinants and health policy. Trop Med Int Health. 2008; 13: 1225–34.
- Lim SS, Gaziano TA, Gakidou E, Reddy KS, Farzadfar F, Lozano R, et al.. Prevention of cardiovascular disease in high-risk individuals in low-income and middle-income countries: health effects and costs. Lancet. 2007; 370: 2054–62.
- Gaziano TA, Galea G, Reddy KS. Scaling up interventions for chronic disease prevention: the evidence. Lancet. 2007; 370: 1939–46.