Abstract
Background: Low fruit and vegetable consumption is among the top 10 risk factors contributing to mortality worldwide. WHO/FAO recommends intake of a minimum of 400 grams (or five servings) of fruits and vegetables per day for the prevention of chronic diseases such as heart diseases, cancer, diabetes, and obesity.
Objective: This paper examines the fruit and vegetable consumption patterns and the prevalence of inadequate fruit and vegetable consumption (less than five servings a day) among the adult population in rural surveillance sites in five Asian countries.
Data and methods: The analysis is based on data from a 2005 cross-site study on non-communicable disease risk factors which was conducted in nine Asian INDEPTH Health and Demographic Surveillance System (HDSS) sites. Standardised protocols and methods following the WHO STEPwise approach to risk factor surveillance were used. The total sample was 18,429 adults aged 25–64 years. Multivariate logistic regression analysis was performed to assess the association between socio-demographic factors and inadequate fruit and vegetable consumption.
Results: Inadequate fruit and vegetable consumption was common in all study sites. The proportions of inadequate fruit and vegetable consumption ranged from 63.5% in men and 57.5% in women in Chililab HDSS in Vietnam to the whole population in Vadu HDSS in India, and WATCH HDSS in Bangladesh. Multivariate logistic regression analysis in six sites, excluding WATCH and Vadu HDSS, showed that being in oldest age group and having low education were significantly related to inadequate fruit and vegetable consumption, although the pattern was not consistent through all six HDSS.
Conclusions: Since such a large proportion of adults in Asia consume an inadequate amount of fruits and vegetables, despite of the abundant availability, education and behaviour change programmes are needed to promote fruit and vegetable consumption. Accurate and useful information about the health benefits of abundant fruit and vegetable consumption should be widely disseminated.
Introduction
Fruits and vegetables are important components of a healthy diet, since they have low energy density and are sources of micronutrients, fiber, and other components with functional properties Citation1. Increased fruit and vegetable consumption can also help displace food high in saturated fats, sugar or salt. Low fruit and vegetable intake is among the top 10 risk factors contributing to mortality Citation2. Up to 2.7 million lives could potentially be saved each year with sufficient global fruit and vegetable consumption Citation3. Increased fruit and vegetable intake as part of the daily diet, could help prevent major chronic non-communicable diseases (NCDs). Worldwide, low intake of fruits and vegetables is estimated to cause about 31% of ischemic heart disease, 11% of strokes, and about 19% of gastrointestinal cancer Citation3Citation4. Of the global disease burden attributed to low fruit and vegetable consumption, about 85% is due to cardiovascular diseases and 15% to cancer Citation4. The estimated levels of current fruit and vegetable intake vary considerably from less than 100 grams per day in less developed countries to about 450 grams in Western Europe Citation4.
WHO/FAO recommends intake of a minimum of 400 grams or five servings of fruits and vegetables per day for the prevention of chronic diseases such as heart diseases, cancer, diabetes, and obesity. There is convincing evidence that consumption of fruits and vegetables decrease the risks of cardiovascular disease, obesity, and diabetes Citation3. In spite of the growing body of evidence which highlights the protective effect of fruits and vegetables, their intakes are still inadequate in many low and middle-income countries Citation5Citation6. The World Health Survey in 2002–2003 showed that over three-fourth of men and women from 52 low and middle-income countries consumed less than the minimum recommended five daily servings of fruits and vegetables Citation5. The fruit and vegetable intake among the population in India, Mali, and Pakistan is about 100 gram per capita per day or less, compared to 300 grams consumed in Australia, several European countries, and the USA. Even so, the fruit and vegetable consumption in these high income countries are still less than the WHO/FAO recommended level of 400 grams or five servings per day Citation7.
This paper describes the patterns of fruit and vegetable consumption in adults 25–64 years in nine health and demographic surveillance system (HDSS) sites in five Asian countries and examines their relationships with socio-demographic characteristics. Results from this study will be used to provide a basic knowledge of the great differences in fruit and vegetable consumption seen in the different areas as a basis for future studies on disease endpoints, as well as providing information to help guide future policy initiatives to promote greater consumption of fruit and vegetable consumption in Asia.
2 Methods
2.1 Data sources
The study was conducted in 2005 in nine HDSS sites in Asia, namely Matlab, Mirsarai, Abhoynagar, and WATCH (Bangladesh), Vadu (India), Purworejo (Indonesia), Kanchanaburi (Thailand), Filabavi and Chililab (Vietnam). All sites are members of the INDEPTH Network which was founded to facilitate linkage of existing HDSS through a focused network on HIV/AIDS, malaria, adult health, and NCDs Citation8. The HDSSs, which are all in rural settings, cover a representative sample of population at a district level. The HDSS are however self-selected, and do not represent the entire region or country.
Taking advantage of the HDSS's sampling frame, a minimum of 250 individuals aged 25–64 years in each sex and 10-year age group were randomly selected from each site.
The methods and materials have been described elsewhere Citation9Citation10. Briefly, data were collected through a personal household interview conducted by the trained data collectors. To ensure the quality of the data collected, respective sites organised training for data collectors before the field work started. During the trainings, the study protocol and instruments were discussed thoroughly. Data collectors were also given the opportunity to practice in administering the questionnaire using the fruit and vegetable show-cards and standard measures (cups, serving portions) when asking questions on fruit and vegetable consumption. Field supervisors were employed to conduct spot-checks, re-checks, and data validation procedures, including accuracy and completeness of data obtained. Field meetings were held regularly to enable researchers, supervisors, and surveyors to identify and discuss problems encountered during the data collection processes.
2.2 Survey instrument and measurements
The pre-tested WHO STEPS questionnaires for chronic NCD risk factors were used to collect core information on the number of days fruits and vegetables are eaten in a typical week and number of fruit and vegetable servings in one of those days Citation10. An average number of fruit and vegetable servings per day was then calculated by using the information on the number of days fruits and vegetables are eaten in a typical week and the number of servings in one of those days.
The show-cards on typical fruits and vegetables and serving sizes were developed and used when asking questions on fruit and vegetable consumption. In addition, standard cups of different serving sizes were also shown while asking the questions on the number of servings.
Following the WHO/FAO recommendation, inadequate fruit and vegetable consumption in this study was defined as consuming less than five servings (or 400 grams) of fruits and vegetables per day, and adequate fruit and vegetable consumption was defined as consuming five or more servings of fruits and/or vegetables per day Citation3.
2.3 Statistical methods
Both descriptive and analytical statistics were carried out using STATA 10 software (Stata Corporation). Means, standard errors and proportions of variables of interest, together with corresponding 95% confidence interval (CI), were calculated. Multivariable logistic regression analyses were performed to examine the association between socio-demographic characteristics and inadequate fruit and vegetable consumption and their associated odd ratios (ORs) and 95% CI were presented. To take into account the different population structure across sites, sampling weights were applied in the data analysis.
2.4 Ethical considerations
The study protocol was approved by the scientific board of the INDEPTH Network. All human subjects in the study were asked for their consents before collecting data, and all had complete rights to withdraw from the study at any time without any threats or disadvantages.
3 Results
A total of 18,429 adults aged 25–64 years, 9,208 men and 9,221 women, were interviewed in this study. Detailed information on the demographic characteristics which were extracted from the overall database is reported in the first paper of this issue Citation9.
The overall fruit consumption pattern of each HDSS site is shown in . The adult population in almost all study sites consumed small amounts of fruit and not frequently. Study subjects in South East Asian HDSSs consumed fruit more frequently, at least three days in a typical week, compared to those in South Asian HDSSs. There were only two sites, Chililab HDSS in Vietnam and Kanchanaburi HDSS in Thailand, where the average numbers of days per week when adults consumed fruits exceeded three days; the average number of fruit servings on the day when fruit was consumed in these two HDSSs ranged between 3.5–3.8 daily servings in men and 3.4–4.1 daily servings in women. These patterns, while less than ideal, were substantially higher than in the other sites. In the other seven HDSSs, the average number of fruit servings on the day when fruit was consumed ranged from almost none in WATCH HDSS, Bangladesh to two daily servings in one of the HDSS in Vietnam (Filabavi). The average number of days per week adults consumed fruit in these seven sites was lowest in WATCH HDSS; the highest average number of days per week when fruit was consumed was in adult women in Purworejo HDSS.
Table 1. Patterns of fruit consumption (95% CI) in nine HDSS sites by gender and age-groups
Gender differences in the average number of days per week adults consumed fruits can be found in almost all sites, except in WATCH in Bangladesh and Vadu in India. Men in three sites (Matlab, Mirsarai, and Abhoynagar) consumed fruit more frequently than women (2.1, 1.2, and 2.8 days among men and 1.1, 0.9, and 2.2 days among women, respectively), whereas men in the sites in Vietnam, Indonesia, and Thailand (Chililab, Filabavi, Purworejo, and Kanchanaburi) consumed fruit less often than women (3.2, 2.5, 2.5, and 3.1 days among men and 3.7, 2.8, 3.1, and 3.7 days among women, respectively). In contrast, there was no gender differences in the average numbers of servings of fruit consumed per day in all sites, with the exception of Chililab, in Vietnam where the average amount of fruit women consumed per day was slightly more than men (4.1 and 3.8 servings, respectively).
Age differences in fruit consumption can also be seen in six of the nine HDSS. Older men and women aged 55–64 years consumed fruit less frequently than younger adults (25–54 years). On the other hand, in almost all sites, the average number of servings of fruit per day did not vary greatly across different age groups with the exception of older women in Chililab and Kanchanaburi and older men in South East Asian HDSSs who consumed smaller amounts of fruit than the other age groups.
As shown in , the adult population consumed more vegetables than fruit in almost all sites. The average number of days vegetables were consumed in a typical week was higher than the average number of days fruit was consumed in a typical week in all sites. Both men and women in the two sites in Vietnam, Chililab, and Filabavi, consumed vegetables every day, whereas in Vadu HDSS in India, vegetables were consumed only 2.4 days per week on average. The average number of vegetable servings on the day when vegetables was consumed were highest in Matlab (3.4 and 3 servings in men and women, respectively), and lowest in Vadu and WATCH (1.3 and 1.5 servings among men and 1.3 and 1.1 servings among women, respectively).
Table 2. Patterns of vegetable consumption (95% CI) in nine HDSS sites by gender and age
Gender differences in vegetable consumption were noted in all four sites in Bangladesh where men consumed more vegetables, both in quantity and frequency, than women. Age difference in quantity and frequency of vegetable consumption can also be observed in many sites. The oldest women in six sites and the oldest men in Vadu and Kanchanaburi consumed vegetables less often than the other adults. They also, on the whole, consumed smaller quantity of vegetables than the younger age groups.
The prevalence of inadequate fruit and vegetable consumption (less than five servings of fruits and vegetables per day) was high in seven sites, as shown in and . In two sites, one in Bangladesh (WATCH) and one in India (Vadu), virtually no one consumed sufficient amount of fruits and vegetables. The highest proportion of adequate fruit and vegetable consumption was observed in Chililab.
Figure 1. Prevalence of population with low fruits and vegetables consumption.
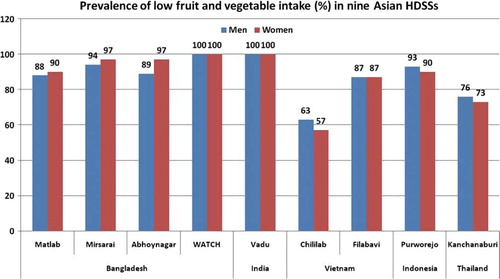
Table 3. Percentages of individual ate less than five servings of fruit and/or vegetable a day (95% CI) in nine HDSS sites by gender and age
The multivariable logistic regression models were constructed to further analyse the association between inadequate fruit and vegetable consumption and socio-demographic characteristics of the adult population. Since the proportions of inadequate fruit and vegetable consumption were 100% in WATCH and Vadu, these were excluded in the models. Table 4 shows the association between gender, age, and education with inadequate fruit and vegetable consumption. Men in Chililab, Purworejo, and Kanchanaburi had higher odds of inadequate fruit and vegetable consumption compared to women, in contrast to men in Mirsarai and Abhoynagar who had lower odds. In addition, the oldest population aged 55–64 years in Matlab, Abhoynagar, and Kanchanaburi as well as the less educated adults in Matlab, Chililab, Filabavi, Purworejo, and Kanchanaburi had higher odds compared to the youngest adults aged 25–34 years and the more educated adults, respectively.
Table 4. Logistic regression of demographic variables on inadequate fruit and vegetable consumption (95% CI) in nine HDSS sites
4 Discussions
This multi-site study examines the pattern of fruit and vegetable consumption and the relationships with socio-demographic characteristics of adult population in nine, largely rural, sites in Asia, and inadequate consumption of fruits and vegetables. This low consumption pattern, particularly fruit consumption, in these Asian populations was also demonstrated in the World Health Survey Citation5. This result is consistent with other studies which have examined population levels of fruit and vegetable intake in countries as diverse as the USA, Brazil, sub-Saharan countries, and India where consumption of fruits and vegetables has been measured separately Citation11Citation12Citation13. Fruit is generally more expensive than vegetables and other common foods and this is reflected in the fact that people with higher income, are more likely to incorporate fruit in their diet Citation14.
The prevalence of inadequate fruit and vegetable consumption, defined as less than five servings a day, was high in all study sites, except for Chililab HDSS in Vietnam and Kanchanaburi HDSS in Thailand, a poor outcome compared with wealthier countries Citation15Citation16Citation17Citation18. Low fruit and vegetable consumption may be due to the nutrition transition in these countries. Over the past two decades, there is increasing evidence that the structure of dietary intake in low and middle income countries has been changing at an increasingly rapid pace. There are also major changes in personal and family lifestyles regarding food intake patterns. Eating patterns in Asia have shifted from a traditional Asian diet – cereal-based and low fat – to a more westernised diet high in animal meats, fats, sugar and refined foods and low in fiber, fruits and vegetables Citation19Citation20Citation21Citation22Citation23Citation24. Another explanation could be related to availability and accessibility of fruits and vegetables; the sites where fruits and vegetables consumption was more favorable were less rural than the other sites; Chililab is mainly peri-urban area and Kanchanaburi includes several urban areas in its catchment population. The results from previous studies and observations in HDSS can be used to explain this finding. The expansion and increasing sophistication of retail marketing together with the large number of local markets, has provided a steady, affordable supply of fruits and vegetables in many urban areas Citation12Citation25. On the contrary, availability and access to fruit and vegetable supplies for people living in rural areas is much more limited. Not all farmers grow vegetables or fruit trees for home consumption and even for those who do, only few varieties were usually grown; production is mainly cash crops for export and sale. Thus, fruits and vegetables may be available only in some seasons, not all year round Citation21Citation22. In addition, local markets in rural areas are more restricted in the variety of fruits and vegetables available for purchase Citation12Citation25.
The rural disadvantage in access to fresh fruits and vegetables also relates to income. Low-income groups of the rural population suffer issues of affordability as well as availability and access to fruits and vegetables; the cost of fruits and vegetables is related to store-types; they tend to be cheaper in supermarkets and larger markets than smaller local food stores or markets. When the cost of individual travel to the stores is included, this may also result in the perception that fruits and vegetables are more expensive. Cheap sources of energy such as grains and starchy staples become the staple diet. Once they have satisfied their basic energy needs, households start diversifying their diets by including animal source foods, dairy products and only then, fruit and vegetable consumption. Furthermore, different psychosocial, cultural and livelihood factors, such as food culture, nutrition knowledge, dietary attitudes, food habits, lifestyle choices, cooking skills, and level of farm activities in different study sites can also affect different levels of fruit and vegetable consumption Citation12Citation26.
The results also indicate that women are more likely than men to have an inadequate fruit and vegetable consumption, although there were notable exceptions in three Southeast Asian sites (Chililab HDSS in Vietnam, Kanchanaburi HDSS in Thailand, and Purworejo HDSS in Indonesia). This suggests that gender also plays a role in food patterns, possibly related to broader cultural differences within the sub-regions included for study. Studies in other countries, in contrast, shows that women tend to consume more fruits and vegetables than men Citation5Citation13Citation15Citation16Citation27Citation28 and researchers have attributed this phenomenon to women's awareness and willingness to follow a healthy diet. Our results suggest that men in South Asian HDSSs consumed fruits and vegetables more often than women, and these results are consistent with the findings from national representative survey in India Citation25. Lower intake of fruits and vegetables in women may be related to the dominant cultural concepts and their relationship with sex roles in the society Citation27. In addition, this study confirms other studies which identify that older and less educated adults in society are those who were more likely to consume fruits and vegetables inadequately Citation6Citation12Citation15Citation16Citation17Citation27Citation28.
In conclusion, effective policies, programmes, and initiatives to promote adequate consumption of fruits and vegetables in the population are urgently needed, given the high prevalence of population who consume less than the minimum recommended five daily servings of fruits and vegetables. Information on health benefits of sufficient fruit and vegetable consumption should be widely disseminated. Behavioural change communication programmes to promote fruit and vegetable consumption should be based on local knowledge regarding the demographic, cultural, and psychosocial factors that affect consumer choices. These should focus on translating accurate and useful information to consumers about the health benefits of sufficient fruit and vegetable consumption. Government policies to support availability, affordability, and accessibility are also urgently required.
5 Conflict of interest
The authors have declared no conflict of interest.
Acknowledgements
The authors would like to acknowledge the INDEPTH Network for financing this work, Dr. Anand Krishnan and Dr. S.K. Kapoor from Ballabgarh HDSS for organising training workshop for this project, the Umeå Centre for Global Health Research, Umeå University, Sweden for supporting the coordination of this supplement, and Dr. Ruth Bonita, who as guest editor for this series of papers, provided substantial and critical scientific input into earlier drafts of this paper.
Related Research Data
References
- Van Duyn MA, Pivonka E. Overview of the health benefits of fruit and vegetable consumption for the dietetics professional: selected literature. J Am Diet Assoc. 2000; 100: 1511–21.
- World Health Organization. World Health Report 2003: shaping the future. GenevaSwitzerland: World Health Organization. 2003.
- World Health Organization. Diet, nutrition, and the prevalence of chronic diseases. GenevaSwitzerland: World Health Organization. 2003. Contract No.: WHO Technical Report Series No. 916.
- Lock K, Pomerleau J, Causer L, Altmann DR, McKee M. The global burden of disease attributable to low consumption of fruit and vegetables: implications for the global strategy on diet. Bull World Health Organ. 2005; 83: 100–8.
- Hall JN, Moore S, Harper SB, Lynch JW. Global variability in fruit and vegetable consumption. Am J Prev Med. 2009; 36: 402–9 e5.
- International Agency for Research on Cancer. Changing structure of global food consumption and trade: agricultural and trade report. LyonFrance: IARC Press. 2001.
- Pollack SL. Consumer demand for fruits and vegetables: the US example. Economic Research Service. US Department of Agriculture. Washington DC, 2001
- INDEPTH Network. Population and health in developing countries. Global Health Action Supplement 1, 2009. DOI: 10.342/gha.V2i0.1988; 2002.
- Ng N, Minh HV, Juvekar S, Razzaque A, Bich TH, Kanungsukkasem U, et al.. Using the INDEPTH HDSS to build capacity for chronic non-communicable disease risk factor surveillance in low and middle-income countries. Manuscript for INDEPTH NCD Series, Global Health Action. 2009
- World Health Organization. WHO STEPS surveillance manual: the WHO STEPwise approach to chronic disease risk factor surveillance. GenevaSwitzerland: Noncommunicable Diseases and Mental Health, World Health Organization. 2005.
- Casagrande SS, Wang Y, Anderson C, Gary TL. Have Americans increased their fruit and vegetable intake? The trends between 1988 and 2002. Am J Prev Med. 2007; 32: 257–63.
- Ruel MT, Minot N, Smith L. Patterns and determinants of fruit and vegetable consumption in sub-Saharan Africa: a multicountry comparison. World Health Organization. GenevaSwitzerland, 2005
- World Health Organization South-East Asia Regional Office. WHO global strategy on diet, physical activity, and health: South-East Asia regional consultation meeting report. New Delhi: World Health Organization South-East Asia Regional Office. 2003.
- Padilla L. Fruit consumption: dietary health and policy implications. Paper presented at 2001 Agricultural and Applied Economics Association Annual Meeting. Chicago: Illinois. 2001, 5–8 August .
- Thompson B, Demark-Wahnefried W, Taylor G, McClelland JW, Stables G, Havas S, et al.. Baseline fruit and vegetable intake among adults in seven 5 a day study centers located in diverse geographic areas. J Am Diet Assoc. 1999; 99: 1241–8.
- Roos G, Johansson L, Kasmel A, Klumbiene J, Prattala R. Disparities in vegetable and fruit consumption: European cases from the north to the south. Public Health Nutr. 2001; 4: 35–43.
- Giskes K, Turrell G, Patterson C, Newman B. Socio-economic differences in fruit and vegetable consumption among Australian adolescents and adults. Public Health Nutr. 2002; 5: 663–9.
- O'Brien MM, Kiely M, Galvin M, Flynn A. The importance of composite foods for estimates of vegetable and fruit intakes. Public Health Nutr. 2003; 6: 711–26.
- Popkin BM. Part II. What is unique about the experience in lower-and middle income less-industrialised countries compared with the very-high-income industrialised countries? The shift in stages of the nutrition transition in the developing world differs from past experiences!. Public Health Nutr. 2002; 5: 205–14.
- Astrup A, Dyerberg J, Selleck M, Stender S. Nutrition transition and its relationship to the development of obesity and related chronic diseases. Obesity Rev. 2007; 9: 48–52.
- Kosulwat V. The nutrition and health transition in Thailand. Public Health Nutr. 2002; 5: 183–9.
- Shetty PS. Nutrition transition in India. Public Health Nutr. 2002; 5: 175–82.
- Popkin BM, Gordon-Larsen P. The nutrition transition: worldwide obesity dynamics and their determinants. Int J Obes. 2004; 28: 52–9.
- Popkin BM. An overview on the nutrition transition and its health impacations: the Bellagio meeting. Public Health Nutr. 2002; 5: 93–103.
- Ministry of Human Resource Development GoI. India nutrition profile. New Delhi: Department of Women and Child Development. 1998.
- James S. A study of fruit and vegetable accessibility in rural areas of England: The University of Reading. Available from: http://www.regroningen.nl/summerschool/ppt/James%20Sully.ppt; 2009. [cited 25 June 2009].
- Baker AH, Wardle J. Sex differences in fruit and vegetable intake in older adults. Appetite. 2003; 40: 269–75.
- Subar AF, Heimendinger J, Patterson BH, Krebs-Smith SM, Pivonka E, Kessler R. Fruit and vegetable intake in the United States: the baseline survey of the Five A Day for Better Health Programme. Am J Health Promot. 1995; 9: 352–60.