Abstract
Background: NovelFootnote1
1This study was performed on behalf of the Community Interventions for Health (CIH) collaboration.
efforts and accompanying tools are needed to tackle the global burden of chronic disease. This paper presents an approach to describe the environments in which people live, work, and play. Community Health Environment Scan Survey (CHESS) is an empirical assessment tool that measures the availability and accessibility, of healthy lifestyle options lifestyle options. CHESS reveals existing community assets as well as opportunities for change, shaping community intervention planning efforts by focusing on community-relevant opportunities to address the three key risk factors for chronic disease (i.e. unhealthy diet, physical inactivity, and tobacco use).Methods: The CHESS tool was developed following a review of existing auditing tools and in consultation with experts. It is based on the social-ecological model and is adaptable to diverse settings in developed and developing countries throughout the world.
Results: For illustrative purposes, baseline results from the Community Interventions for Health (CIH) Mexico site are used, where the CHESS tool assessed 583 food stores and 168 restaurants. Comparisons between individual-level survey data from schools and community-level CHESS data are made to demonstrate the utility of the tool in strategically guiding intervention activities.
Conclusion: The environments where people live, work, and play are key factors in determining their diet, levels of physical activity, and tobacco use. CHESS is the first tool of its kind that systematically and simultaneously examines how built environments encourage/discourage healthy eating, physical activity, and tobacco use. CHESS can help to design community interventions to prevent chronic disease and guide healthy urban planning.
Chronic diseases such as cardiovascular disease, diabetes, cancer, and chronic respiratory diseases, caused by three main risk factors (unhealthy diet, physical inactivity, and tobacco use), are responsible for 60% of the global burden of diseases Citation1. This chronic disease burden is escalating, especially in developing countries, and can be largely attributed to changing lifestyles, a result of rapid urbanization and globalization, and the nutrition transition Citation2 Citation3 Citation4 Citation5 .
Knowledge gained over the last 30 years has demonstrated that individual behavior is influenced by complex, interconnected social, environmental, and psychological factors. The development of effective chronic disease intervention programs requires that each layer of influence is addressed Citation6.
Decades of research have demonstrated that targeted behavioral interventions are not sustainable beyond program activities Citation7 Citation8. A more comprehensive approach that addresses the environmental factors in addition to individual behaviors change is required to ensure sustainability of change. The new emphasis on prevention and intervention science is to target societal factors influencing lifestyles; for example, food pricing policies, built environments, and smoke-free regulations Citation3 Citation6 Citation8 Citation9 Citation10 Citation11 Citation12 Citation13 .
Early successes in tobacco control reinforce the effectiveness of moving from individual behavior change intervention strategies to broader community-wide structural changes, making healthier choices easier ones. In tobacco control, the single most effective intervention has been increasing the unit price of tobacco products via excise taxes Citation14. However, taxes alone cannot explain population-wide decreases in tobacco consumption, but rather coordinated efforts across all sectors has made tobacco control one of the most successful public health interventions to date Citation11.
Lessons learned from tobacco control can be translated into efforts to address unhealthy diet and physical inactivity and reduce global obesity rates Citation11 Citation15. Obesity is caused by an imbalance in energy intake and expenditure Citation1 Citation13. Although seemingly straightforward, societal factors that influence this energy imbalance are extremely complex, as illustrated in the Foresight obesity system map, and require a system-wide, multi-stakeholder approach that involves key players who influence what we eat and how physically active we are – nutrition scientists, agriculture specialists and policy-makers, food companies, urban planners, and architects Citation16.
Key policy levers and specific levels of influence are not yet well understood; more research that focuses on the exact role of environmental factors in the energy balance equation is needed Citation17 Citation18. Furthermore, new innovative research tools are needed to build effective interventions targeting unhealthy diet (energy in) and physical inactivity (energy out) and to improve our understanding of the effects of environmental attributes on individuals, families, communities, and societies.
The interactions between chronic diseases and their associated lifestyle risk factors are complex and go beyond the traditional cause-and-effect models and/or germ theory. A social ecological model has been the preferred theoretical framework used to understand the influences of behavioral risk factors associated with chronic diseases Citation9. The traditional social ecological model describes different levels of influence on individual behaviors that includes the following factors: Citation1 individual (biological, psychological), Citation2 social/cultural, Citation3 organizational, Citation4 community, Citation5 physical environment, and Citation6 political Citation19.
The Community Intervention for Health (CIH) program of the Oxford Health Alliance is based on the social ecological framework of health promotion and disease prevention. CIH is a combined research and intervention project with an extensive evaluation component. CIH is focused on addressing the three main risk factors for chronic disease in four settings – schools, workplaces, health care facilities, and neighborhoods – using four intervention strategies: Citation1 community coalition building, Citation2 structural change, Citation3 health education, and Citation4 social marketing. CIH is the first comprehensive community intervention program of its kind, addressing chronic disease risk factor reduction and prevention in developed and developing countries. A 3-year pilot study is currently underway in China, India, Mexico, and the United Kingdom. Lessons learned from the CIH pilot study will help build a roadmap of strategies for effectively addressing chronic disease risk factors in both developing and developed country settings (i.e. determining what works and does not work for chronic disease prevention).
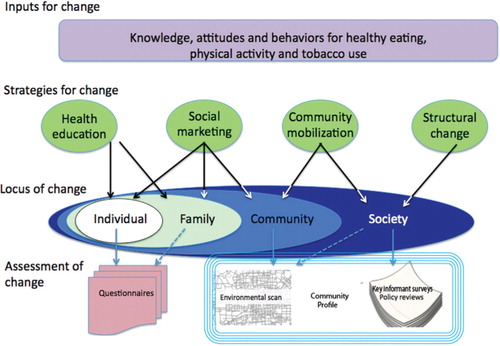
The evaluation of the effectiveness of the CIH interventions includes three components: Citation1 individual assessments (measured with surveys), Citation2 assessment of the community context (measured with the CIH Community Profile), and Citation3 assessment of the process required to implement the activities (measured by CIH Process Evaluation) ().
Fig. 1. CIH evaluation framework. In the CIH multilevel framework, the concentric circles illustrate the ecological model and the various layers that influence behavior. The upper arrows illustrate the CIH intervention strategies influencing both the proximal and distal factors related to behavior. The evaluation framework includes individual assessments and the community profile that informs the impact of the interventions. The environmental scan captures the community environment as well as structural changes and some aspects of health education and social marketing. Key informant interviews and policy review add another layer of analysis and provide a deeper understanding of the community context.
The CIH Community Profile was developed as a tool to understand the community context and to inform interventions, as well as to measure the effectiveness of the intervention strategies at the 2-year follow-up. The Community Profile includes policy reviews, key informant interviews, facility scans for use in schools, workplaces, and health care facilities, and the environmental scan (the Community Health Environmental Scan Survey – CHESS). The methods presented in this research paper are focused on CHESS, the environmental scan component of the CIH community profile. For a more detailed explanation of the CIH evaluation framework see (O'Connor-Duffany, K. et al. to be published in the Journal of Prevention and Control).
The development of CHESS and the analysis strategies presented in this paper focus on understanding the community context for behaviors in a way that is novel, innovative, and easy to understand. This tool has the potential to be utilized by academics, policy-makers, urban planners, non-governmental organizations, government officials, among others. Tackling the multifaceted nature of chronic disease requires major rethinking of the role of the built environment and the factors that influence decision-making at the individual level around the availability, accessibility, and affordability of opportunities to impact unhealthy diet, physical inactivity, and tobacco use.
One of the major challenges in developing an environmental audit tool like CHESS is ensuring the applicability of a tool that can be used in both developed and developing country settings. In the developed world there is access to pre-populated data on some built environment features such as stores, restaurants, and parks. However, even this data is problematic given the infrequency within which information is updated. In the developing world, obtaining information down to the community level is even more problematic as there is limited GIS mapping and almost non-existent data on built environment factors. Therefore, methods and tools that can assess community attributes in ‘real-time’ are needed.
Methods
The Community Health Environmental Scan Survey (CHESS) is an empirical tool developed by the CIH evaluation team to systematically document, map (via GPS), and assess the environments in which people, shop, live, work, and play as they relate to diet, physical activity, and tobacco use. The main objective of CHESS is to improve our understanding of the environment's that we live in that promote healthy eating, physical activity, and tobacco use and the link between this and a population's health behaviors and resulting health outcomes. The information gathered is also used to guide intervention planning efforts.
We first performed a literature search of available tools that assess community environments related to diet, physical activity, and tobacco use. Prior to CHESS, there were no tools addressing all three risk factors simultaneously; however, separate tools were found that assess stores Citation20, restaurants Citation21, farmer's markets, schools, workplaces, and the built environment supporting physical activity Citation22 Citation23 Citation24 . We also consulted with international experts in the fields of diet, physical activity, and tobacco use in order to develop a framework for assessing each risk factor. Some aspects of accessibility are measured using GIS mapping as well as other key attributes (e.g. hours of operation). Affordability could not be systematically measured, although some aspects of cost data are collected.
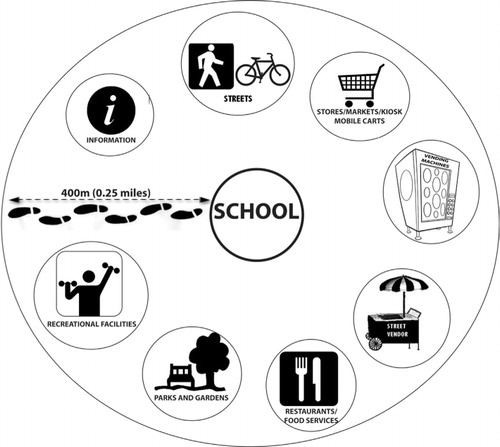
CHESS includes eight brief assessment tools that inventory streets, stores, restaurants, street vendors, recreational facilities, parks/gardens, vending machines, and the information environment. includes the main items of CHESS that are used in the analysis for this paper (the complete listing of CHESS components can be found in Appendix 1). The assessment of a community assessment using CHESS is conducted via a ‘neighborhood walk’, which initiates from selected schools within each community and extends in a 400 m radius. We used schools as the main focal point of interest because it is a common urban planning practice to define neighborhood units beginning with schools and other civic facilities Citation25 Citation26. Furthermore, schools tend to be more than just places of education for a narrow segment of the population; they are typically integral centers of communities Citation25 Citation27, and places of community growth and vitality. Using schools also allows for the collection of comparable data across the CIH pilot sites and provides a representative glimpse of the community.
Table 1. Components of CHESS
Table 5. Appendix 1. Full CHESS tool
depicts the overall strategy for the neighborhood walk, beginning with schools in each neighborhood. It shows how the various components of the scan dovetail in any given community.
Fig. 2. The neighborhood environmental scan includes walking a 400 m radius around each school and identifying and/or surveying all stores, vending machines, restaurants, recreational facilities, vendors, and so on.
The design of the CIH project within each community includes administering surveys to children (approximately 2,000 children between 12 and 14 years of age per intervention community).Footnote2 Maps of the areas to be scanned were created using Google Earth Pro, and the 400 m radii were created using a circular ruler program. CHESS data were collected using a personal digital device (PDA) with integrated GPS and camera (Magellan Mobile Mapper 6). CHESS was programmed using electronic survey software (Snap version 9).
CHESS was conducted around a minimum of 50% and a maximum of 100% of all sampled schools (with a minimum of 10 schools and a maximum of 20 schools in the intervention and control areas). To ensure reliability between raters, standard definitions were developed for categorization of the key features of each of the eight scan components and a training manual was created. Members of the evaluation team went to each site and worked with the local research teams to collect data over a 14–21 day period. For the first 3 days of each visit, the local researchers from each CIH site were trained on the scan and participated in country level adaptations with the evaluation team. Prior to the formal scanning of each community, all raters were trained using the training guidebook, practiced in the field in teams, and then one radius was completed by all raters to ensure reliability.
A preliminary inter-rater reliability study of the environmental scan was conducted in one community setting using four raters. In general, the agreement was consistently high overall for the main variables including number of stores, restaurants, and parks (Kappas and AC1 close to 1.0), as well as for the presence of fruits and/or vegetables (Kappa = 0.707, p<.049 and AC1=.901, p<.00) Citation2 and tobacco (Kappa = 1.000, p<.008 and AC1 = 1.000).
Results: scope and impact of the environmental scan
In order to demonstrate the scope and impact of the CHESS tool, we present the results along with baseline school level data from the CIH Mexico site. This data illustrates two important functions of CHESS: Citation1 to define the availability and accessibility of healthy food options, and Citation2 to guide the development and planning of interventions. Similar strategies and analyses can also be conducted to examine physical inactivity and tobacco use, but they are beyond the scope of this illustration.
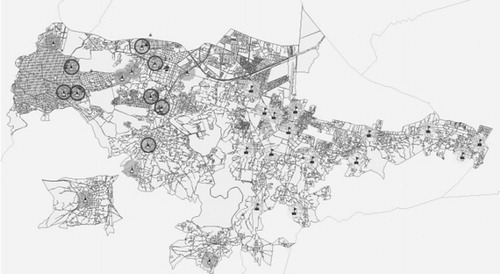
presents a map of the area assessed by CHESS in both the intervention and control areas. Each of the school radii are mapped, numbered, and noted as intervention or control area. Using the schools as our focal point gives us an understanding of the types of environments in which students interface in their daily lives as well as a representative sample of the entire community as schools are distributed throughout the area, and it allows us to capture the different types of settings – rural, semi-urban, and urban – in both the intervention and control areas.
Fig. 3. Overview of the control and intervention area and distribution of the selected schools in both areas.
In addition to the school-centric, community-level data collected with CHESS, the individual-level survey data from students attending each of these schools allows for comparisons to be drawn between the community-level data and student-level behavioral data. These comparisons provide a comprehensive picture of the built environment including facilitators and barriers.
In our Mexico CIH site example, 15 neighborhoods were scanned in the intervention and control areas. Examining only the information collected relating to the food environment and the availability of cigarettes, a total of 583 stores/kiosk/fix care/mobile carts, and 168 restaurants were scanned and GIS mapped. The school surveys conducted on students living in the scanned radii included a total of 4,608 youth aged 12–14 years. For the modeling of environmental data and student behavior, student data was merged with environmental data that had 2,733 observations from 16 schools. For a summary of indicators used in this analysis and their descriptive statistics, refer to . More than half of the students reported eating at a fast food restaurant in the last week. The proportion of students smoking cigarettes was 14% and overall tobacco use was 17%; it was not surprising that the overwhelming majority of tobacco use was cigarette use.
Table 2. Summary of fast food and tobacco consumption indicators
In , the results of log-linear regression models are presented that explore the association between the types of restaurants scanned and the frequency of students eating at fast foodFootnote3 restaurants in the past 7 days. Similar associations were explored between the availability of tobacco products in stores and student's tobacco use behavior.
Table 3. Food environment and food behavior
The number of days of eating at fast food restaurants during the past 7 days was significantly associated with the percentage of restaurants providing fast foods, as was the percentage of restaurants providing both fast foods and healthier items (mixed restaurant) (). There was not a significant association between the number of days of fast food and the total number of restaurants. When the students were dichotomized into those who had and those who had not eaten in fast food restaurants in the last week, a different pattern of association was observed. There was a significant association between not eating fast food and the total number of restaurants and the proportion of restaurants serving fast foods. These negative associations mean that persons will be more likely to fast food where there are more restaurants and where a higher proportion of them sell fast food.
The relationship between the availability of tobacco products and student tobacco use behaviors is presented in . The odds of a student being a current cigarette smoker, smoking tobacco user, overall tobacco user, or ever having tried smoking cigarettes was greater in radii with a higher percentage of stores selling tobacco. However, a greater proportion of stores having ‘no sales to minor’ signs was significantly negatively associated with current smokeless tobacco use but not any other type of tobacco use.
Table 4. Tobacco use and tobacco environment
By comparing and contrasting the results from the environmental scan (CHESS) with student food consumption patterns and tobacco use behaviors from their surveys, we have a better understanding of the environments in which they are living. We observe that the types of restaurants and the availability of tobacco products does influence their consumption behavior. Moreover, we can accurately identify the specific communities to design targeted interventions to address tobacco use and unhealthy diet.
Discussion
Results from the CHESS tool highlight the importance of capturing data about the community environment. As additional layers of data are added, a more complete picture of the community can be developed in order to improve the understanding of the environmental determinates for unhealthy diet, physical inactivity, and tobacco use. The results of the information presented here can serve as a guideline for intervention development around healthy eating and tobacco use among youth. Specific examples include but are not limited to: Citation1 improving availability of fruits/vegetables by working with local food vendors including school canteens, creating farmers markets, encouraging fast food restaurants to provide fruits and vegetables; Citation2 providing educational interventions for youth about healthy food choices in restaurants and/or unhealthy aspects of tobacco use; and Citation3 instituting fines/penalties for selling tobacco to minors.
This is one example of many to illustrate the contribution of CHESS to understanding how a community's attributes affect health behaviors in order to design effective intervention programs. Other examples include but are not limited to: Citation1 locations of parks and recreational centers and reported physical activity, Citation2 types of retailers selling single cigarettes and tobacco use and Citation3 availability of low fat/salt/sugar food options and eating habits.
There are few empirical tools available that systematically and simultaneously assess opportunities for healthy eating, physical activity, or reduced tobacco use in neighborhood environments. Tools that do exist focus on physical activity levels Citation22 Citation24 Citation28 or specific aspects of food habits Citation20 Citation21 and have been developed for use in developed countries. CHESS is the first tool to address all three risk factors for chronic disease simultaneously. The multifactorial nature of chronic disease and its risk factors warrants the development of tools to address proximal factors that influence unhealthy diet, physical inactivity, and tobacco use. Many of the components of these tools are context specific and do not easily translate to non-western and developing country settings.
The CHESS tool and overall methodology was created to address the gap in our current knowledge regarding community context. It is possible to identify secondary data sources and map some information about communities such as parks, stores, and restaurants. However, it is not possible to obtain reliable data on what stores sell, what restaurants sell, what vendors are selling surrounding schools, and/or type of recreational facilities available without actually physically walking and assessing the community. Moreover, the availability of community GIS data is limited to developing countries and they do not take into consideration the sometimes rapid changes in communities (e.g. closing of stores, restaurants). One of the advantages of applying CHESS in the community is that it enriches one's understanding and engagement of the community environment, which is an important factor in developing successful interventions.
All western countries have recognized that the strain on health systems attributed to chronic diseases cannot be sustained if the rates of chronic disease remain unabated. One of the most cost-effective investments is to implement effective prevention programs Citation29. The environments in which people live, play, and work are important agents in determining their diet, physical activity, and tobacco use. In order to develop effective interventions for the future and scaling up of successful programs, an improved understanding of the complex interplay between environmental determinates and individual behavior is needed.
Limitations
A potential limitation of the environmental scan is that it provides a community snapshot and may not capture the dynamic nature of communities. The street markets and mobile vendors are important sources for where people buy their foods in some communities and may not be captured at the time or on the day the scan is conducted. Another limitation is the ability to measure affordability, given the variability of units in how fruits and vegetables were sold, it was difficult to collect cost data that can be compared across different types of food vendors. However, the pricing data collected is informative in understanding cost of fruits and vegetable for communities where the CHESS was applied. The process of conducting the neighborhood walk is labor intensive; however, once completed it serves as an important resource to the community as long as data sharing strategies are presented and discussed. Although CHESS has face validity, it is clear that it will need to be tested in a variety of settings and further reliability and validity studies are needed.
Conclusion
CHESS is the first environmental assessment tool of its kind to simultaneously assess the three key primary risk factors for chronic disease. The results of the CIH research project using the CHESS will provide the first set of evidence of its kind on the complex interplay between behavior and environmental determinants on food consumption patterns, tobacco use, and physical activity levels.
Chronic disease is emerging as the greatest public health challenge of the twenty-first century. Although much of the burden could be prevented through known interventions – eating a healthy diet and increasing physical activity Citation30 – little is known about how to address the causes within a complex web of behavioral and societal factors. Despite some successes in intervention programs, there remains limited evidence available on how to translate best and promising practices for chronic disease prevention into different settings. Research in North America and Europe has demonstrated the correlation between environmental determinants and physical activity levels and food consumption patterns Citation13. The evidence generated by this research is now being translated into the development of policies around urban planning, education, health care, and social services. However, research on environmental determinants of physical activity levels and food consumption patterns in developing countries is absent.
Finite resources for tackling today's pressing global health challenges mean that it is important for policy- and decision-makers to be armed with the most up-to-date data in order to efficiently and effectively allocate resources. As developing countries continue rapid modernization, a greater understanding of how the health and well-being of their citizens are affected by these changes is required. CHESS is one tool that can help.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study. Community Interventions for Health (CIH) is supported by a registered UK charity, the Oxford Health Alliance (OxHA), and facilitated by MATRIX Public Health Solutions Inc. For a full list of donors supporting OxHA please go to www.oxha.org.
Notes
1This study was performed on behalf of the Community Interventions for Health (CIH) collaboration.
2At least 75% of all streets within the 400 m had to be covered in order for the scan to be complete for each radius.
3In consultation with a local researcher from Mexico City, fast food was defined as Americanized fast food, those outlets selling hamburger, pizza, hot dogs, and so on. Local researchers were not interested in looking at indigenous fast foods.
Related Research Data
References
- Joint WHO/FAO expert consultation on diet, nutrition and the prevention of chronic diseases. Geneva: World Health Organization. 2003.
- Beaglehole R, Yach D. Globalisation and the prevention and control of non-communicable disease: the neglected chronic diseases of adults. Lancet. 2003; 362: 903–8.
- WHO. 2008–2013 action plan for the global strategy for the prevention and control of noncommunicable diseases. Geneva: World Health Organization. 2008.
- Huynen MM, Martens P, Hilderink HB. The health impacts of globalisation: a conceptual framework. Globalization and Health. 2005; 1: 14.
- Popkin BM. Urbanization, lifestyle changes and the nutrition transition. World Development. 1999; 27: 1905–16.
- Booth SL, Mayer J, Sallis JF, Ritenbaugh C. Environmental and societal factors affect food choice and physical activity: rationale, influences, and leverage points. Nutrition Review. 2001; 59: S21–S29.
- Sha E, Smith GD. Exporting Failures? Cornary heart disease and stroke in developing countries. Int J Epidemiol. 2001; 30: 201–5.
- Katan MB. Weight-loss diets for the prevention and treatment of obesity. N Engl J Med. 2009; 360: 923–25.
- Sallis JF. Measuring physical activity environments: a brief history. Am J Prev Med. 2009; 36: S86–S92.
- WHO. A framework to monitor and evaluate implementation: WHO global strategy on diet, physical activity and health. Geneva: World Health Organization. 2008.
- Mercer SL, Green LW, Rosental AC, Husten CG, Khan LK, Dietz WH. Possible lessons from tobacco experience for obesity control. Am J Clin Nutr. 2003; 77: 1073S–82S.
- French SA, Story M, Jeffery RW. Environmental influence on eating an physical activity. Annu Rev Public Health. 2001; 22: 309–35.
- James PT, Rigby N, Leach R, International Obesity Task Force. The obesity epidemic, metabolic syndrome and future prevention strategies. Eur J Cardiovasc Prev Rehabil. 2004; 11: 3–8.
- Adeyi O, Smih O, Robles S. Public policy and the challenges of chronic noncommunicable diseases. World Bank. Washington DC, 2007
- Yach D, McKee M, Lopez AD, Novotny T, for Oxford Vision 2020. Improving diet and physical activity: 12 lessons from controlling tobacco smoking. BMJ. 2005; 330: 898–900.
- Tackling obesities: the foresight report. London: Local Government Improvement and Development. 2007.
- Kremer SP, de Bruijin G-J, Visscher TL, van Mechelen W, De Vries NK, Bruge J. Environmental influence on energy balance-related behaviors: a dual-process view. Int J Behav Nutr Phys Activity. 2006; 3: 1–10.
- Jeffery RW. How can health behavior theory be made more useful for intervention research?. Int J Behav Nutr Phys Activity. 2004:1–5.
- Sallis J, Owen N, Fisher EB. Ecological models of health behaviour. Health behavior and health education: theory, research and practice. Glanz K, Rimer BK, Viswanath KJossey-Bass. San Francisco CA, 2008; 465–82.
- Karen G, James FS, Brian ES, Lawrence DF. Nutrition Environment Measures Survey in Stores (NEMS-S): development and evaluation. Am J Prev Med. 2007; 32: 282–89.
- Brian ES, Karen G, James FS, Lawrence DF. Nutrition Environment Measures Study in Restaurants (NEMS-R): development and evaluation. Am J Prev Med. 2007; 32: 273–81.
- Day K, Boarnet M, Alfonzo M, Forsyth A. The Irvine–Minnesota inventory to measure built environments: development. Am J Prev Med. 2006; 30: 144–52.
- Pikora TJ, Giles-Corti B, Knuiman M, Bull FC, Jamrozik K, Donovan RJ. Neighborhood environmental factors correlated with walking near home: using SPACES. Med Sci in Sports Exerc. 2006; 38: 708–14.
- Cunningham GO, Michael YL, Farquhar SA, Lapidus J. Developing a reliable senior walking environmental assessment tool. Am J Prev Med. 2005; 29: 215–17.
- Lawhon LL. The neighborhood unit: physical design or physical determinism?. J Plann Hist. 2009; 8: 111–32.
- Krizek K. Neighborhood services, trip purpose, and tour-based travel. Transportation. 2003; 30: 387–400.
- LEED for Neighborhood Development Rating System (Pilot Version). WashingtonDC: USGBC. 2007.
- Pikora TJ, Bull FCL, Jamrozik K, Knuiman M, Giles-Corti B, Donovan RJ. Developing a reliable audit instrument to measure the physical environment for physical activity. Am J Prev Med. 2002; 23: 187–94.
- Suhrcke M, Nugent RA, Stuckler D, Rocco L. Chronic disease: an economic perspective. Oxford Health Alliance. London, 2006
- Diabetes Prevention Program Research Group. 2002; 346: 393–403.