Aim
The Västerbotten Intervention Programme (VIP) addresses cardiovascular disease and diabetes in the middle-aged population of Västerbotten County, Sweden. Self-reported health (SRH) is one of the risk factors for both conditions. The aim of this study was to analyse the development patterns of SRH among the VIP participants.
Methods
Cross-sectional data from 1990 to 2007 were used to analyse the prevalence of poor SRH among 101,396 VIP participants aged 40–60 years. Panel data were used to study the change in SRH among 25,695 persons aged 30–60 years, who participated in the VIP twice within a 10-year interval.
Results
Prevalence of poor SRH fluctuated between 1990 and 2007 in Västerbotten County. There was a temporary decline around 2000, with SRH continuously improving thereafter. The majority of panel participants remained in good SRH; over half of those with poor or fair SRH at baseline reported better SRH at follow-up. SRH declined in 19% of the panel participants, mostly among those who had good SRH at the baseline. The decline was common among both women and men, in all educational, age and marital status groups.
Conclusions
The SRH improvement among those with poor and fair SRH at baseline suggests that VIP has been successful in addressing its target population. However, the deterioration of SRH among 21% of the individuals with good SRH at baseline is of concern. From a public health perspective, it is important for health interventions to address not only the risk group but also those with a healthy profile to prevent the negative development among the seemingly healthy participants.
Self-reported health (SRH) is a valid Citation1 and reliable Citation2 predictor of various health outcomes, including mortality Citation3, development of functional decline and numerous chronic conditions Citation3–Citation5, particularly cardiovascular disease (CVD) Citation6–Citation10. By virtue of this, a question on SRH is included in the Västerbotten Intervention Programme (VIP) survey, part of an intervention programme designed to prevent CVD and diabetes among the population in Västerbotten County, Sweden Citation11.
It has been demonstrated earlier that public health interventions influence individual's SRH. In the North Karelia study, the SRH ratings have improved significantly more in the intervention than in the reference area and the perceived risk of developing CVD decreased Citation12. Similarly, the evaluation of the Norsjö intervention programme Citation13 has shown a reduction in a CVD risk factor load and an improvement in the SRH ratings in the intervention area. Hence, the SRH was suggested as a suitable outcome measure for the evaluation of public health interventions Citation13.
The evaluation of the VIP is ongoing. The development of the risk factor burden among the VIP participants is being studied through the assessment of the change in health behaviours Citation14 and the biometrical measurements such as cholesterol, blood sugar, body mass index, etc. (manuscripts are under development). The aim of this study was to assess the development of the SRH among the VIP participants. The specific objectives were Citation1 to describe the SRH development over time by using VIP data from 1990 to 2007 and Citation2 to analyse the patterns of the SRH change in individuals who participated twice in the VIP.
Methods
All Västerbotten residents are invited to participate in the VIP upon becoming 40, 50 or 60 years old, thus having a chance to participate in the VIP once every 10 years. Individuals aged 30 were also invited to participate until 1995. The participation is voluntary and the participation rate is typically about 60%. VIP is conducted by medical personnel at local healthcare centres. First, some biometrical measurements are taken and then the participants fill in a questionnaire concerning their socioeconomic status, SRH, life satisfaction, social support, lifestyle (eating habits, alcohol intake and smoking, physical activity), personal history and family history of CVD and diabetes. Finally, individual counselling by means of a motivational interview based on the results of the medical examination and the questionnaire takes place regarding individual's risk factors and required lifestyle changes. A more detailed description of the VIP survey design can be found elsewhere Citation11.
The current study was based on the VIP questionnaire data obtained during 1990–2007 and analysed both cross-sectionally and longitudinally (a 10-year panel).
Participants
Cross-sectional sample
The cross-sectional sample included 101,396 individuals who were 40, 50 or 60 years old and participated in the VIP at least once during 1990–2007. The 30-year olds were excluded since data were not available for the entire study period.
Panel sample
The panel analysis included all 25,695 individuals aged 30, 40 or 50 years at the initial survey (1990–1997) who participated in a 10-year follow-up study when they turned 40, 50 or 60 years, respectively, during 2000–2007.
Classification of variables
SRH was determined by response to the question ‘How would you describe your health status during the past year: very good, rather good, fair, rather poor or poor?’ Individuals who responded ‘very good’ or ‘rather good’ were considered to have ‘good’ SRH. Those who responded ‘fair’ were considered to have ‘fair’ SRH and those who responded ‘rather poor’ or ‘poor’ were considered to have ‘poor’ SRH.
SRH at follow-up was compared with SRH at baseline. Those who reported the same SRH at follow-up as at baseline were categorised as ‘remained’; those who reported poorer SRH at follow-up were categorised as ‘deteriorated’; and those who reported better SRH at follow-up were categorised as ‘improved.’
Sex was categorised as ‘man’ or ‘woman.’
Age was categorised as ‘30’, ‘40’, ‘50’ or ‘60’ years.
Educational level was categorised into ‘basic’ (elementary and comprehensive compulsory school), ‘mid-level’ (residential college for adult education or high school) and ‘high’ (college or higher) educational levels.
Marital status was dichotomised into ‘married/cohabiting’ with or without children or ‘single’ with or without children. The latter group also included divorced, separated or widowed individuals.
Marital status at follow-up was compared with marital status at baseline. Respondents were categorised accordingly into ‘remained married/cohabiting,’ ‘remained single,’ ‘became single’ or ‘became married/cohabiting.’
Statistical analyses
Prevalence of good, fair and poor SRH was determined over 18 years of observations in the cross-sectional sample (n = 101,396). Ten-year changes in SRH were evaluated using the panel data (n=25,695). Individuals with incomplete information on SRH and/or the demographic variables of interest listed earlier comprised approximately 2% of the samples and were excluded. All tables and figures were adjusted for sex, age, educational level and marital status, unless otherwise stated. The differences between the groups were assessed with the Pearson's chi-square test (p< 0.05). Data analyses were performed using STATA Version 10.1 Citation15.
Ethical considerations
This study was approved by the Regional Research Ethics Board in Umeå, Sweden (Dnr 08-131 M). Individuals provided written consent prior to each survey and health screening.
Results
The results of the cross-sectional and panel data analyses are presented separately in the following sections. The descriptive characteristics of both samples are presented in .
Table 1. Descriptive characteristics of the cross-sectional and panel samples
Cross-sectional data
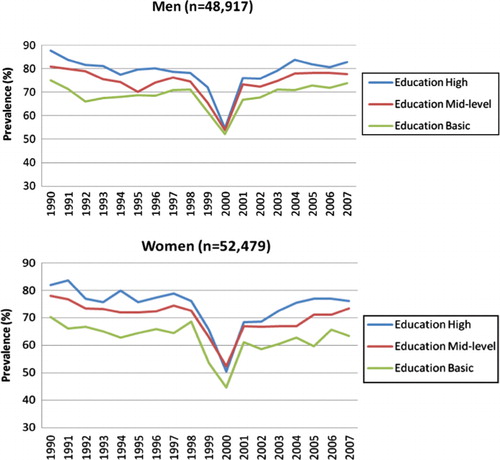
On average, 71% of individuals reported good SRH, 22% reported fair SRH and 7% reported poor SRH in 1990–2007 (). Poor SRH was more likely to be reported by women than men, older than younger adults, single than married individuals and by those in the lowest educational category ().
Table 2. Distribution of good, fair and poor self-reported health in the cross-sectional sample (N=101,396) during 1990–2007
There was deterioration in SRH around 2000 for both men and women of all educational levels. The deterioration remained significant after adjustment for age and marital status (). The fall in good SRH was most pronounced among women with basic education. The recovery was gradual, and in 2007, the prevalence of good SRH was still lower than in 1990 among all groups.
Fig. 1. Self-reported health in men and women by educational level, Västerbotten County, 1990–2007 (the cross-sectional sample N=101,396). The figure is adjusted for age and marital status.
Panel data
At follow-up, 70% of respondents reported the same SRH as at baseline, 19% reported poorer SRH and 11% reported better SRH. The most pronounced deterioration was among persons with good SRH at baseline (). In general, 21% (n = 4,236) of individuals with baseline good SRH had poorer SRH at follow-up (fair or poor). On the other hand, 71% of those with poor SRH at baseline reported better SRH at follow-up. However, this group constituted only 3% (869) of the panel sample.
Table 3. Change in the self-reported health at 10-year follow-up, stratified by self-reported health at baseline (the panel sample N=25,695)*
The deterioration of SRH was significantly (p< 0.05) more prevalent in women than in men, in older than in younger adults, among those with basic education than among those with high- or mid-level education at baseline ().
Table 4. Deterioration of self-reported health at 10-year follow-up by sample characteristics (the panel sample N=25,695)
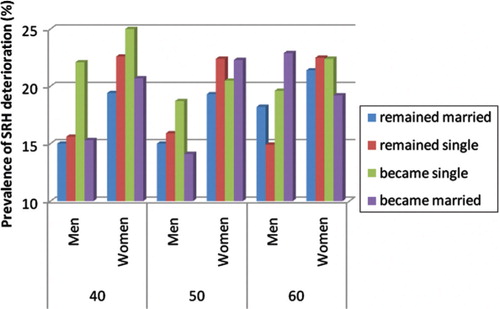
Over 3,500 persons had changed their marital status during the follow-up period. We, therefore, analysed the association between SRH deterioration and change in marital status. Change in marital status was associated with change of SRH. Interestingly, any change of marital status (becoming married/cohabiting or single/divorced) was associated with a greater deterioration of SRH than remaining in the same marital status at follow-up. As shown in , becoming single was associated with greater deterioration in younger than in older adults, and in women more than men. However, even a change to being married/cohabiting was associated with greater deterioration of SRH in men who turned 60 at follow-up.
Fig. 2. Deteriorated self-reported health at 10-year follow-up (the panel sample N=25,695). This figure is stratified by follow-up sex, age and change in marital status and is adjusted by educational level at follow-up.
Discussion
SRH of middle-aged men and women fluctuated between 1990 and 2007 in Västerbotten County. There was a temporary deterioration in the overall SRH around 2000, but this trend reversed, and SRH continuously improved thereafter. Panel data showed that the majority of the VIP participants remained in good SRH at follow-up and over half of those with poor or fair SRH at baseline reported better SRH at follow-up. SRH declined in 19% of participants, mostly among those who had good SRH at baseline. The decline was common among both women and men, in all educational, age and marital status groups.
The overall SRH level observed in the cross-sectional data (71% good, 22% fair and 7% poor) corresponded well with national figures. According to Swedish National Statistical Bureau, 75% of adults aged 18–84 years had good SRH and 6% had poor SRH in Sweden during 1996–2005 Citation16. Also, in line with previous research Citation17 Citation18, women, individuals with basic education, single and older persons had poorer SRH than their comparison groups.
The SRH deterioration around 2000 was not unique for Västerbotten County. A similar temporary decline in SRH was observed in Stockholm County Citation19 Citation20 and at the national level Citation21. According to the National Board of Health and Welfare, self-reported prevalence of psychological problems, pain, sleeping problems and long-standing illness also increased during the same period across the whole country Citation21. An increase in the number of people on long-term sickness pension, disability pension and sickness allowance in Sweden and in Västerbotten County, in particular, were also seen at this time Citation22–Citation24. However, the causality behind this decline and the consequent improvement of SRH are yet to be understood. These questions are addressed in detail elsewhere by Blomstedt et al Citation25.
The panel data showed that the majority of the VIP participants remained in the same SRH at follow-up as at baseline. Moreover, 71% of those with poor SRH and 47% of those with fair SRH at baseline experienced improvement in their SRH. In total, 11% (n=2,898) of the sample (n=25,695) had better SRH at follow-up. This is in line with a previous study of SRH changes in a sub-sample of the VIP population followed between 1986 and 1996 Citation13.
The panel data also revealed a deterioration of SRH among 17% of men and 21% of women over a 10-year period. The deterioration was common for all respondents, but was more pronounced among the 50 years old and those with the basic educational level at baseline. The change of marital status was also associated with the change in SRH. Becoming single was associated with a decline in SRH among younger persons (30 years old at baseline), and surprisingly, becoming married/cohabiting was also associated with a decline in SRH, mainly in older men (50 years at baseline).
The decline of SRH with age is well-known and has been widely discussed in the literature Citation26 Citation27. In line with our observations, other follow-up studies in European populations have also shown a decline of SRH with time Citation28 Citation29. A previous 10-year follow-up study of a VIP sub-sample (n=174) found the same deterioration rate. Nineteen percent of those with good SRH at baseline in 1986 reported fair or poor SRH in 1996 Citation13.
SRH at baseline is usually the strongest predictor of SRH at follow-up Citation30. Unexpectedly, in our study, the proportion of participants with poorer SRH at follow-up was higher among those who had good rather than fair SRH at baseline (21% vs. 14%). This is a concern and suggests the possibility that those who were healthier at the baseline did not benefit from the intervention programme as much as those who were less healthy.
Poor SRH is a risk factor itself, as well as one that accompanies CVD and diabetic conditions. Being designed to target persons at risk for developing or already having CVD or diabetes, VIP is successful in helping persons to reduce their risk factor burden and improve their SRH Citation13 Citation31–Citation34. This is also confirmed in the current study by the improvement in SRH of the majority of those with poor SRH and almost half of those with fair SRH at baseline. Since 2009, the healthcare personnel within VIP have been specifically educated to give particular attention to persons who have poor or fair SRH along with other CVD risk factors. This recommendation is based on findings from Weinehall et al Citation35 and Emmelin et al Citation36, which show that poor SRH dramatically increases the risk for acute myocardial infarction and stroke among persons with other CVD risk factors. However, such focus on CVD risk factors and poor SRH may cause an unforeseen and undesired side effect. Those with good SRH at baseline might feel left out and exhibit deterioration in their SRH at follow-up.
These results should not undermine the success of VIP in addressing the target population as illustrated in earlier studies Citation13 Citation31–Citation34. Moreover, earlier VIP studies have shown that SRH deterioration among VIP participants is slower than in the reference area Citation37. Nevertheless, our findings raise the question of how to best design a health intervention to reach the whole population of a defined geographical area.
According to our analysis, 21% of those with good SRH at baseline deteriorate over 10 years. Since poor SRH is a proxy of general health and may reflect preclinical manifestations of disease Citation38 Citation39, we need to consider whether it is possible to prevent this negative development among seemingly healthy participants as part of the VIP.
Our analysis also illustrated that other factors (e.g. marital status) influence SRH. This shows that deterioration of SRH is not only associated with lifestyle risk factors or chronic conditions such as CVD or diabetes, even if lifestyle is a strong predictor of a future SRH Citation28. Therefore, it is important to emphasise that from a public health perspective, VIP should use its influence to target not only those who are clearly at risk for developing CVD or diabetes and have poor SRH but also those with good SRH at baseline. The methods of addressing such participants (e.g. confirmation, encouragement) are not discussed here, but should be considered elsewhere. This argument is supported by a qualitative sub-study of VIP participants done in 1995–1996. That study found a desire among the participants to be seen and confirmed by the VIP personnel even if they did not have any of the risk factors that VIP was designed to target. Otherwise, they felt disappointed and left out – feelings that increase their risk of moving from a low to high CVD risk factor load Citation13.
Conclusion
The analysis of the SRH development among the VIP participants during 1990–2007 in Västerbotten County, Sweden, suggested a positive effect of the VIP. The majority of the VIP participants remained in good SRH, and the majority of those with fair or poor SRH at baseline revealed improvement in their SRH at 10-year follow-up. Nevertheless, a fifth of the VIP participants, mostly those with good SRH at baseline, had deterioration in SRH at a 10-year follow-up. These findings raise a question of how to best design a health intervention to reach the whole population of a defined geographical area. From a public health perspective, it is important to support health maintenance and prevention of future disease in those with a healthy profile as well as the high-risk individuals.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study. This study was funded by FAS, the Swedish Council for Working Life and Social Research (Grant no. 2006-1512) and the Swedish Research Council (Grant no. 2008-6592).
Acknowledgements
This work was undertaken at the Umeå Centre for Global Health Research, funded by FAS, the Swedish Council for Working Life and Social Research (Grant no. 2006-1512), and within the Ageing and Living Conditions Programme, funded by a Linnaeus grant from the Swedish Research Council (Grant no. 2008-6592). All authors contributed to discussion and presentation of results as well as revision of the manuscript. YB conducted the data analyses. The funding sources were not involved in any parts of the study conduct or data analyses.
Related Research Data
References
- Manderbacka K, Lundberg O, Martikainen P. Do risk factors and health behaviours contribute to self-ratings of health?. Soc Sci Med. 1999; 48: 1713–20. 10.3402/gha.v4i0.5435.
- Lundberg O, Manderbacka K. 1996; 24: 218–24.
- Idler EL, Benyamini Y. 1997; 38: 21–37.
- Fayers PM, Sprangers MAG. 2002; 359: 187–8.
- DeSalvo KB, et al.. Predicting mortality and healthcare utilisation with a single question. Health Serv Res. 2005; 40: 1234–46. 10.3402/gha.v4i0.5435.
- Orth-Gomer K, Unden AL, Edwards ME. 1988; 224: 205–15.
- Pijls LT, Feskens EJ, Kromhout D. Self-rated health, mortality, and chronic diseases in elderly men. The Zutphen Study, 1985–1990. Am J Epidemiol. 1993; 138: 840–8.
- Appels A, Bosma V, Grabauskas A. 1996; 42: 681–9.
- Moller L, Kristensen TS, Hollnagel H. Self rated health as a predictor of coronary heart disease in Copenhagen. Denmark. J Epidemiol Community Health. 1996; 50: 423–8. 10.3402/gha.v4i0.5435.
- Heistaro S, et al.. Self rated health and mortality: a long term prospective study in eastern Finland. J Epidemiol Community Health. 2001; 55: 227–32. 10.3402/gha.v4i0.5435.
- Norberg M, Boman K, Weinehall L. The Västerbotten Intervention Programme: Background, design and implications. Global Health Action. 2010; 3. 10.3402/gha.v4i0.5435.
- Kottke TE, et al.. Changes in perceived heart disease risk and health during a community-based heart disease prevention programme: the North Karelia project. Am J Public Health. 1984; 74: 1404–5. 10.3402/gha.v4i0.5435.
- Emmelin M, Weinehall L, Stenlund H, Wall S, Dahlgren L. To be seen, confirmed and involved--a ten year follow-up of perceived health and cardiovascular risk factors in a Swedish community intervention programme. BMC Public Health. 2007; 7: 190.10.3402/gha.v4i0.5435.
- Norberg M, et al.. Changing patterns of tobacco use in a middle-aged population – the role of snus, gender, age, and education. Glob Health Action. 2011; 4.
- StataCorp. Stata Statistical Software: Release 10.1. College StationTX: Stata Corporation. 2009.
- Population Statistics, part 3. Örebro: Statistics Sweden. 2007.
- Undén A-L, Elofsson S. Do different factors explain self-rated health in men and women?. Gender Medicine. 2006; 3: 295–308. 10.3402/gha.v4i0.5435.
- af Sillen U, et al.. Self-rated health in relation to age and gender: influence on mortality risk in the Malmo Preventive Project. Scand J Public Health. 2005; 33: 183–9. 10.3402/gha.v4i0.5435.
- Public Health Report. Stockholm: National Board of Health and Welfare. 2007.
- Burström K, Johannesson M, Rehnberg C. Deteriorating health status in Stockholm 1998–2002: results from repeated population surveys using EQ-5D. Qual Life Res. 2007; 16: 1547–53. 10.3402/gha.v4i0.5435.
- Public Health Report. (). Stockholm: National Board of Health and Welfare. 2005.
- Statistical information. Days covered by sickness allowance, December 1998 – June 2002. Stockholm: The Social Insurance Office. 2002.
- Statistical information. Diseases that caused retiring. Stockholm: The State Insuarance Office. 2004.
- Lidwall U, Marklund S, Thoursie PS. Sickness absence in Sweden. Worklife and health in Sweden. Gustafsson RÅ Lundberg INational Institute for Working Life. Stockholm, 2004; 183–204.
- Blomstedt Y, Blomstedt P, Janlert U, Weinehall L. The millennium shift: might a symbolic date affect the level of self-reported health in a modern secularised society?. (submitted).
- Andersen FK, Christensen K, Frederiksen H. Self-rated health and age: a cross-sectional and longitudinal study of 11,000 Danes aged 45–102. Scand J Public Health. 2007; 35: 164–71. 10.3402/gha.v4i0.5435.
- Chen H, Cohen P, Kasen S. Cohort differences in self-rated health: Evidence from a three-decade, comunity-based, longitudinal study of women. Am J Epidemiol. 2007; 166: 439–46. 10.3402/gha.v4i0.5435.
- Borg V, Kristensen TS. Social class and self-rated health: can the gradient be explained by differences in life style or work environment?. Soc Sci Med. 2000; 51: 1019–30. 10.3402/gha.v4i0.5435.
- Disney R, Emmerson C, Wakefield M. Ill health and retirement in Britain: a panel data-based analysis. J Health Econ. 2006; 25: 621–49. 10.3402/gha.v4i0.5435.
- Miller TR, Wolinsky FD. Self-rated health trajectories and mortality among older adults. J Gerontol B Psychol Sci Soc Sci. 2007; 62: S22–7.
- Weinehall L, et al.. Shifting the distribution of risk: results of a community intervention in a Swedish programme for the prevention of cardiovascular disease. J Epidemiol Community Health. 1999; 53: 243–50. 10.3402/gha.v4i0.5435.
- Weinehall L, et al.. Can a sustainable community intervention reduce the health gap? 10-year evaluation of a Swedish community intervention programme for the prevention of cardiovascular disease. Scand J Public Health Suppl. 2001; 56: 59–68.
- Jansson JH, Boman K, Messner T. Trends in blood pressure, lipids, lipoproteins and glucose metabolism in the Northern Sweden MONICA project 1986–99. Scand J Public Health Suppl. 2003; 61: 43–50. 10.3402/gha.v4i0.5435.
- Lindahl B, et al.. Trends in lifestyle1986 –1999 in a 25- to 64-year-old population of the Northern Sweden MONICA project. Scand J Public Health Suppl. 2003; 61: 31–7. 10.3402/gha.v4i0.5435.
- Weinehall L, et al.. Perceived health modifies the effect of biomedical risk factors in the prediction of acute myocardial infarction. An incident case-control study from northern Sweden. J of Internal Med. 1998; 243: 99–107. 10.3402/gha.v4i0.5435.
- Emmelin M, et al.. Self-rated ill-health strengthens the effect of biomedical risk factors in predicting stroke, especially for men – an incident case referent study. J of Hyperten. 2003; 21: 887–96. 10.3402/gha.v4i0.5435.
- Emmelin M. Self-rated health in public health evaluation (PhD thesis). Umea University. Umea, 2004
- Froom P, Melamed S, Triber I, Ratson NZ, Hermoni D. Predicting self-reported health: the CORDIS study. Prev Med. 2004; 39: 419–23. 10.3402/gha.v4i0.5435.
- Szwarcwald CL, Souza-Junior PR, Esteves MA, Damacena GN, Viacava F. Socio-demographic determinants of self-rated health in Brazil. Cadernos de saude publica / Ministerio da Saude, Fundacao Oswaldo Cruz, Escola Nacional de Saude Publica. 2005; 21 Suppl: 54–64.
