Abstract
Background : In Sweden, the smoking prevalence has declined. In 2007, it was among the lowest in the industrialized world. A steady increase in the use of Swedish oral moist snuff, snus, has occurred in parallel. This development is neither solicited by authorities nor the medical establishment, but rather has occurred along with increased awareness of the dangers of smoking, and has been promoted by product development and marketing of snus.
Objective : To evaluate time trends in patterns of tobacco use in northern Sweden during 1990–2007.
Design : Cross-sectional (99,381 subjects) and longitudinal (26,867 subjects) data from the Västerbotten Intervention Programme (VIP) 1990–2007 were analyzed. All adults in Västerbotten County are invited to a VIP health examination at ages 40, 50, and 60 years, and until 1995 also 30 years. Smoking and use of snus were evaluated by gender, age and educational groups. Intermittent smoking was categorized as smoking.
Results : From the period 1990–1995 to the period 2002–2007, smoking prevalence decreased from 26 to 16% among men and from 27 to 18% among women. The differences in prevalence increased between educational groups. The decline in smoking was less and the increase of snus use was greater among those with basic education. The use of snus among basic-educated 40-year-olds reached 35% among men and 14% among women during 2002–2007. Dual smoking and snus use increased among men and women with basic education. Smoking without snus use was more prevalent among women. Gender differences in total smoking prevalence (smoking only plus dual use) were small in all age groups, but increased among those with basic education reaching 7.3% during 2002–2007, with women being more frequent smokers. Smoking prevalences were similar among never, former and current snus users. Among the 30,000 former smokers, 38% of men and 64% of women had never used snus. Longitudinal data showed a decline in total tobacco use from baseline until follow-up and this was mainly due to a smoking cessation rate of < 1% a year. Snus use was started by 6.2% of the 30-year-old women (age at baseline), and this contributed to a stable prevalence of total tobacco use in this group. Seventy percent of baseline snus users still used snus at follow-up. Among smokers, 55% continued smoking, 12% of men and 7% of women switched to snus. Among those with dual tobacco use at baseline, a third of men and a fourth of women remained dual users 10 years later.
Conclusion : There are increasing differences in tobacco use between educational groups. Higher smoking and snus use prevalence are found among those with basic education, and this is most pronounced in the younger group of this middle-aged population. In spite of a higher prevalence of smoking without snus use among women, total smoking prevalence is similar in men and women due to a higher prevalence of dual tobacco use, i.e. snus and cigarettes, among men. The increase in snus use is being paralleled by a slight increase in dual use and the smoking prevalence does not seem to be influenced by snus. This should be the subject of further studies and also have implications for tobacco control policies.
Tobacco is the number one preventable cause of death worldwide. Smoking is a risk factor for six of the eight leading causes of death and currently causes over five million deaths annually Citation1 Citation2. From that perspective the Swedish situation is positive. In Sweden, the prevalence of daily smoking was 35% in men and 28% in women in 1980, and declined to 13 and 15% in 2007, which is among the lowest national rates in the world Citation3 Citation4. Regional differences exist with smoking prevalence varying from 16% in men and 22% in women in Södermanland County in southern Sweden, to 9% of men and 11% of women, in the northern county of Västerbotten. Parallel to the smoking decline, there has been a steady increase in the use of Swedish oral moist snuff, called snus. During the same period, the use of any form of tobacco has been stable Citation5. The decline in smoking prevalence is thought to be mainly due to increased snus use. Smokers switch to snus as an aid when stopping smoking Citation6 Citation7, and snus use may reduce smoking initiation Citation5 Citation8. However, the majority of Swedish smokers who quit smoking do so without switching to snus Citation9 Citation10, and the largest increase in snus use is seen among male teenagers and young adults aged 16–24 years Citation11.
Snus is a product that traditionally has been used in Sweden since early nineteenth century. It differs from many other smokeless tobacco products due to its lower content of tobacco-specific nitrosamines. The maximum blood nicotine level after single doses of snus is similar to smoking one cigarette, although snus peaks slower, and the elevated nicotine level has longer duration after snus than after smoking a cigarette Citation12. The addictive capacity of snus to nicotine is comparable to smoked tobacco Citation13. These days Snus is largely consumed as pouches, i.e. small tea-bag-like packages, that allow it to remain under the upper lip for prolonged periods. The increase in snus in Sweden has occurred more or less in response to increased awareness of the dangers of smoking. The authorities and the medical establishment have not responded to this increase in a consistent way. In contrast, the driving forces from manufactures, including product development and marketing, have been strong and obvious. It has been widely debated whether snus should be given the credit for the low prevalence of smoking in Sweden Citation8 Citation9. Sweden is the only country in the European Union that has an exception from the ban on manufacturing and selling snus. The tobacco industry and their allies are pushing for lifting the ban in the EU.
A cohort study that included the middle-aged population of Västerbotten County showed that the tobacco-free proportion increased from 75.2 to 79.2% for women and from 61.1 to 64.3% for men from the early 1990s to the early 2000s Citation10. The present study aims to broaden the results from this study by accounting for age and socioeconomic status, measured as attained educational level, when evaluating time trends in tobacco use patterns during the time period 1990–2007. We also evaluated longitudinal changes in tobacco habits from baseline (1990–1997) to 10-year follow-up (2000–2007).
Methods
Population
The Västerbotten Intervention Programme (VIP) has been ongoing in the county of Västerbotten since 1985. In 1985, the county's cardiovascular (CVD) mortality rate was remarkably high and therefore VIP was launched by local authorities to reduce the burden of CVD and diabetes. VIP was designed in collaboration between health care providers and Umea University. The methodology was first tested in a single community and gradually spread to the rest of the county. Since 1990 the whole county has been involved. Thus, VIP is population-based and a longstanding activity. All inhabitants are invited to a health examination the year they turn 40, 50, or 60 years of age. One underpinning principle is that individuals are invited to attend the survey by their local primary health care centre, and the examination takes place at each center. Until 1995, those aged 30 years were also included. The health examination is integrated in routine activities and includes assessment of the classical CVD risk factors and a comprehensive questionnaire with questions on socioeconomic factors and housing, as well as self-reported health and life style habits including tobacco use. Individually, each participant is given the results of the examination and health promoting issues are discussed using motivational interviewing. Details of the VIP design and methodology have been described previously Citation14.
This paper is based on consecutive surveys from 1990 to 2007 and include a total of 112,920 subjects (49.2% men). Participation rates were 48–57% during 1990–1995, then increased and has been 66–67% since 2005 Citation14. Since subjects aged 30 years (n=8,980) were only included in the VIP until 1995, this age group was excluded from the cross-sectional analyses.
Three panels including yearly cohorts of VIP-participants in 1990–1997 aged 30, 40 or 50 years and who returned to a follow-up visit 10 years later, are also investigated. A drop-out analysis based on the Swedish population register, that covers the whole Swedish population, showed that among participants 1990–1997 (N=38,041) a total number of 2,649 were not eligible for follow up due to migration from the region (N=1,508) or from the country (N=173), death (N=909), change in person number (N=13), or other causes (N=47). Of eligible participants 75.9% (N=26,867) returned a second time after 10 years. Thus, both cross-sectional and longitudinal data are evaluated.
Variables
Assessment of tobacco habits are based on two different questions in the questionnaire. Smoking was separated into three categories: never-smokers, former smokers and current smokers. Former intermittent smokers (used to smoke occasionally but not daily) and former daily smokers were categorized as former smokers. Subjects who currently were smoking intermittently or daily were grouped together as current smokers in this article. For comparison, mean values of the prevalence of smoking with this categorization (I) and an alternative categorization (II), where the 3.6% male and 3.5% female intermittent smokers are included in the not smoking category, are shown for the period 1990–2007 in . The use of snus was categorized into never, former and current use. Cross-tabulation of the three smoking and snus categories resulted in nine categories: never used tobacco, never smoker and former snus user, never smoker and current snus user, former smoker and never snus user, former smoker and former snus user, former smoker and current snus user, current smoker and never snus user, current smoker and former snus user, and current smoker and current snus user (also called dual use).
Table 1. Prevalence (%) of smoking by two different classifications among participants in the VIP, Sweden
To reduce the complexity of tobacco habit categories, never and former smokers, as well as never and former snus users, were further grouped into non-smokers and non-snus users. Participants were then divided into smokers/non-smokers and snus-users/non-snus users. These two variables were cross-tabulated, and thus defined four mutually exclusive categories of tobacco-free, exclusive snus users, exclusive smokers and smokers also using snus (dual use).
Socioeconomic status was assessed by the highest educational level according to the Swedish educational system. Nine years in school is compulsory and was defined as basic education. Completion of 12 years in school was defined as mid-level education, and university or academic graduation was categorized as high education.
Statistics
Prevalence for the nine categories of tobacco habits and three educational levels are presented by sex and age for the three periods of 1990–1995, 1996–2001, and 2002–2007. The age-adjusted distributions of the four categories (tobacco-free, exclusive snus users, exclusive smokers, and dual users) are given for each educational group during the study period. The age-distribution of the whole study-group is used as a reference-population; men and women are analyzed separately. Comparisons between distributions are done with chi-squared-test, and multinomial logistic regression was used to compare the tobacco habits in the different educational groups over time and by age and gender. Longitudinal data are used to estimate age-adjusted changes in tobacco habits from baseline to 10-year follow-up by gender and education and statistical significance is analyzed using the Marginal Homogeneity test. Statistical significance was assumed at p<0.001. All analyses were done with SPSS version 18.
Ethical considerations
This study was approved by the regional Research Ethics Board in Umea (08-131M). Each individual gave informed consent prior to the health screening.
Results
Cross-sectional data: population trends in tobacco use
During 1990–2007, a total of 103,940 subjects aged 40, 50, or 60 years participated in VIP. This was 52–69% of the eligible population. The lowest participation rates were in the mid 1990s and the highest during the more recent years Citation14. Data regarding tobacco use were completed by 47,850 men and 51,531 women, with missing data among 4.3% of men and 4.4% of women. Data are presented in three periods, 1990–1995, 1996–2001, and 2002–2007. The proportion of 60-year-olds increased from 27% in 1990–1995 to 34% in 2002–2007. A corresponding reduction from 38 to 32% was seen in the 40-year-old group and the 50-year-old group was a stable proportion of approximately 35%.
During the study period, the level of education increased in all groups but it was highest and increased more markedly among women (). The highest prevalence of university graduation was found among 40-year-old women and was 40.7%, during 2002–2007, compared to 11.1% among 60-year-old men during 1990–1995. Mid-level education increased in all age groups, but particularly among men.
Table 2. Distribution (%) of tobacco use and attained educational level among men and women who participated in the VIP, Sweden, 1990–2007. There were statistically significant differences (p < 0.001) for tobacco habits in all comparisons between periods in both men and women, and between men and women in all three periods, and also for education in all comparisons between periods in both men and women. Furthermore, in education comparisons between men and women in the three periods were statistically significant (p < 0.001), except among 60-year-olds, among whom there was no difference between men and women during 1990–1995 p=0.82 and in the period 1996–2001 the difference was significant with p=0.004
In the early 1990s, 40.1% of men and 28.1% of women used some form of tobacco (all ages); a reduction of 1.5% for men and 3% for women was seen until 2002–2007. Time trends for the nine categories of smoking and snus use by age group are shown in .
The overall smoking prevalence (smoking only plus dual use and all age groups together) decreased by 10% (from 26 to 16%) among men from 1990–1995 to 2002–2007, and by 9% (from 27 to 18%) among women. Dual use was more common among men in all ages, and therefore, in spite of smoking only being more prevalent among women, the difference between men and women was small with regard to total smoking prevalence in the three age groups; 1.6% among 40-year-olds, 4.2% among 50-year-olds, and 2.2% among 60-year-olds.
Among 40-year-olds, smoking (smoking only plus dual use) decreased from 28 to 13% among men and from 32 to 14% among women. Never-smoking increased from 41 to 67% in men and from 40 to 59% in women. Former smoking decreased from 31 to 21% in men and was stable at 27% among women. Fifty-year-old men and women also reported a reduction in smoking prevalence of 10 and 7%, respectively. Among those aged 60 years, there were only small shifts between smoking categories among men. Among women, the smoking group was stable, the proportion of former smokers increased from 22 to 36%, and a corresponding decrease in never-smokers from 60 to 45% was seen.
Snus was most frequently used among 40-year-old men and increased from 28% during 1990–1995 to 34% during 2002–2007. This increase of snus user was dominated by never smokers while the group of former smokers was stable. Among 40-year-old women, the group of snus users increased more than four-fold, from 3 to 14%, dominated by former smokers. The trend of increasing prevalence of snus use was even more obvious among 50-year-old men, and increased from 18% in the first period to 30% in the third period. This increase was similarly distributed between never smokers and former smokers. At the same time, the prevalence of 50-year-old male never snus users declined with 14% from 66 to 52%, and the prevalence of 50-year-old male former snus-users increased with 3% and was 18.7% in the third period. Fifty-year-old women increased their snus use from 0.8 to 8.2%, and this mainly occurred among former smokers. Among 60-year-olds, the use of snus increased from 14 to 21% among men and from 0.3 to 3% among women and among both genders the snus users were predominately former smokers.
Among men during the period from 1990 to 2007, 58.5% did not have any history of snus use, 16.4% were former users and 25.1 were daily users. Among women these proportions were 91.8, 3.2 and 5.0%, respectively. The prevalence of current smoking (daily or intermittent) in the three snus using groups among men was 18.2, 21.6 and 21.4%, and among women 22.1, 28.3 and 21.4%. Thus, the prevalence of smoking was similar in five of these snus using groups with differences < 3% between groups. The only exception being the 3.2% of women who were former snus users, among whom 28.3% were smokers. Smoking has declined over time in all snus using groups in both men and women.
During the study period more than 30,000 former smokers (48% women) participated in VIP (). Among them 38% of the men and 84% of the women had never used snus. Thirty-six percent of the men and 8% of the women were former snus users. During 2002–2007, the prevalence of former snus use among women who were former smokers was two-fold higher among 40- versus 50-year-olds, and thirty-fold higher compared to 60-year-olds during 1990–1995. Moreover, during 2002–2007 40-year-old female former smokers had quit smoking without using snus to a similar extent (55.8%) as 60-year-old male former smokers had done during 1990–1995 (58.2%).
Table 3. Number of former smokers among participants in the VIP, Sweden, during 1990–2007, and the proportion without a history of ever using snus, or with a history of former snus use. The rest of the participating former smokers were current snus users at the time of the health survey. All comparisons between periods in both men and women, as well as all comparisons between men and women in all three periods are statistically significant p < 0.001
Age-adjusted time trends for tobacco consumption patterns from 1990 to 2007 by educational group are shown in . The tobacco-free proportion of the population was approximately 55, 60 and 70% among men with basic, mid-level and high education, and 65, 70 and 80%, in comparable groups of women. These proportions were stable (within±2%) during the study period, however, there was a declining trend among men (–3.3%) and women (−6.4%) with basic education.
Figure 1. Patterns of tobacco use among participants in the VIP, Sweden, from 1990 to 2007 by gender and educational status. Data are mean values for three 6-year periods, adjusted to the age-distribution for men and women in the whole dataset.
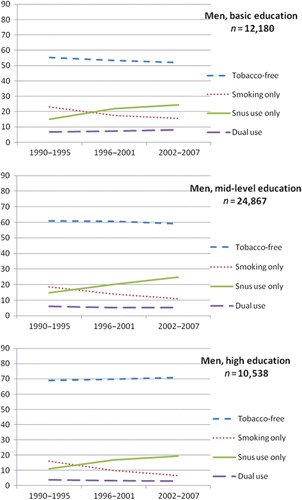
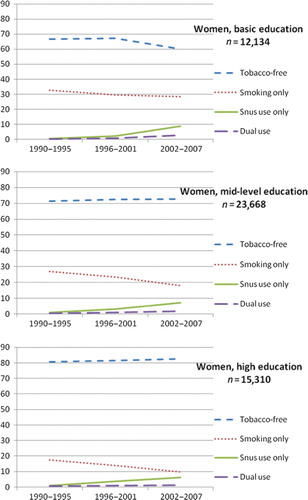
Smoking decreased in all ages and educational groups, but this was less marked throughout the study period among men and women with basic education. Smoking declined 5.9 and 1.8% among men and women with basic education, compared to 10.1 and 7.1% among high educated. Therefore, the difference in smoking prevalence between those with basic and high education increased in both genders. Similarly, the lower the educational level, the greater the increase was in prevalence of snus use. This resulted in increasing differences between educational groups among snus users. Among women, those with high education took up snus use earlier than those with basic education, but the increase was more marked from the mid-1990s among the basic educational group and surpassed the prevalence of snus use among the highly educated. This resulted in a higher prevalence of snus use among women with basic education and larger differences between educational groups at the end of the study period. Among men with either basic or high education, the increasing trend of snus use slowed down during 2002–2007. Dual use was more common among men, in particular among those with basic education, and was 6.6% during 1990–1995 and 8.3% during 2002–2007 in this group. Dual use also increased slowly among women with basic education, from 0.1 to 2.6%. The age-adjusted prevalence of dual use among men (all educational groups) was 3.8% in the period 1990–1995 and 5.1% in 2002–2007, and among women 0.5 and 1.1%.
The difference between men and women with regard to overall smoking prevalence (smoking only plus dual use) was stable throughout the study period among those with high (1.5%) and mid-level (3.5%) education. In contrast, among those with basic education the difference between men and women increased from 3.3% during 1990–1995 to 7.3% during 2002–2007, with women smoking the most frequently.
Smoking and snus use trends crossed in the mid-1990s among men, resulting in snus use becoming more prevalent than smoking. Among women, rates of smoking and snus use approached equilibrium and the difference among highly educated women was only 1% in 2007, compared to 8% among mid-level, and 11% among women with basic education. This was despite snus use being more prevalent among women with mid-level (10%) and basic (14%) education. Thus, in 2007 smoking was three-fold more prevalent among men and women with basic education as compared to those with high education. Prevalence rates of snus use showed less marked differences between educational groups of both genders and were 31, 29, and 23% among men with basic, mid-level and high education, and 14, 10, and 8% among women in those educational groups.
Using the trend of non-tobacco use as a reference, multinomial logistic regression showed that smoking was stable among low educated while those with middle and high education reduced their smoking. The increase in dual use was statistically significant among those with low education (OR 1.4, 95% CI 1.25–1.50), nearly significant among middle educated (OR 1.1, 95% CI 0.998–1.13) but not among highly educated (OR 0.96, 95% CI 0.86–1.07). Snus increased significantly in all educational groups.
Panel data: changes in tobacco use over 10 years in panels aged 30, 40 and 50 years at baseline
The 26,867 subjects who participated twice in VIP were 30, 40 or 50 years of age at baseline during 1990–1997, and 92.4% completed all questions regarding education and tobacco use. A drop-out analysis comparing baseline characteristics for participants and non-participants (participated at baseline but did not return for the 10-year follow-up) was performed among eligible VIP participants. This showed that among the participants there were fewer men (difference of 3.6%), 30-year-olds (difference of 6.6%), daily smokers (difference of 5.9%), and snus users (difference of 2.1%) compared to those who did not participate at follow-up. The difference among educational groups was 1.5%, with more non-participants who had high education.
The transition of tobacco habits are shown in . The tobacco-free group was the most stable group over the 10-year period. In both genders approximately 90% of those who were tobacco-free at baseline remained so at follow-up and 2.6% of men and 3.2% of women became smokers and 4.2 and 1.4% became snus users. In contrast, among baseline snus users 6.1% of men and 8.1% of women were smokers at 10-year follow-up and the majority of them were dual users. A larger proportion of smokers compared to snus users quit using tobacco during the period. Among baseline smokers 7.4% of men and 2.4% of women, changed to dual tobacco use. Among those who were dual users at baseline 34.4% of men and 25.7% of women remained dual users at follow-up.
Table 4. Transition of tobacco use (%) from baseline during 1990–1997 until 10-year follow-up during 2000–2007 among participants in the VIP
Tobacco consumption at baseline (1990–1997) and follow-up (2000–2007) by gender, education and age at baseline, as well as the 10-year changes are shown in . Similar to the cross-sectional data, this shows that smoking and snus use were more prevalent among those with lower education. The use of tobacco from baseline until follow-up decreased in all age and educational groups. This was most marked among 40- and 50-year-old men and women, reflecting a high smoking cessation rate among all ages of women and the 40- and 50-year-old men. A high frequency of uptake of snus among women with basic education who were 30-years-old at baseline contributed to the stable overall tobacco use in this group, in spite of the high smoking cessation rate. Smoking prevalence decreased by < 1% per year and during the 10-year period by 7–10% in most groups. An exception was 30-year old men, who reduced their smoking by 2.4–5.4% between surveys, and high educated 30-year old women, who reduced their prevalence by 4.7%. The latter group was also the one with the lowest smoking prevalence of all both at baseline and follow-up. The use of snus increased most markedly among 30- and 40-year old women, and in particular among those with basic education (+6.0% and +6.6%, respectively) whose overall use of snus reached 15.5% and 8.0% at follow-up. The younger age groups of women with basic education also had the highest prevalence of smokers at follow-up, 31.5% of 30-year olds and 29.4% of 40-year olds. Despite a small 10-year reduction from baseline of snus use only, dual use and smoking among 30-year old men with basic education, among men this group had both the highest prevalence of snus users (37.4%) and smokers (25.4%), including dual use, at follow-up. The decline of dual use from baseline until follow-up among men was smaller than the decline in smoking alone, i.e. a few percentage points in all categories. Dual use was uncommon among women but showed an increasing tendency in most groups.
Table 5. Tobacco use (%) by sex and attained educational level at baseline (Bl) during 1990–1997 and at follow-up (F) after 10 years during 2000–2007, and the change between surveys among participants in the Västerbotten Intervention Programme, Sweden, who were 30, 40 or 50 years old at baseline. The change from baseline to follow-up was not statistically significant among men who were 30 years old at baseline and with basic education (p = 0.213). Among 30 years old men with high education and 30 years old women with basic or high education the p-value was <0.05. All other p-values were <0.001.
Discussion
The main finding of both the repeated cross-sectional and longitudinal data analyses was the substantial and increasing differences between educational groups among both men and women with regard to tobacco consumption patterns. This was most marked in the younger part of the population. Among 40-year-old men and women with basic education, non-use of tobacco actually decreased. This is in line with findings from several previous studies Citation15–Citation18. During the observation period, smoking decreased and the use of snus increased. This was seen most clearly in the younger part of this middle-aged population. Never-smokers were seen to increase among male snus users while the female snus users were dominated by former smokers. This demonstrates the ongoing transition in Sweden from smoking to use of snus. Men started this practice 10–15 years before women. In spite of a low smoking prevalence in an international perspective, there remains considerable nicotine dependence in this middle-aged population. More than one out of three men and one out of four women smoked or/and used snus in 2002–2007. Our next finding is that the smoking prevalence was nearly the same among former, current and never snus users. If this was a randomized trial it would definitely refute the argument that snus use reduces smoking prevalence. However, as the subjects have self-selected themselves into the three groups of snus use, the conclusion must be limited to say that our data is not in support of the claim of smoking reduction of snus. This, and the fact that most people who quit smoking in Sweden do so without using snus Citation9 Citation10, points to the fact that on a population level, snus has played a small role in the decision process to quit smoking. In addition, our longitudinal data show that among those who are tobacco-free in middle age few begin smoking, whereas 6% of men and 8% of women who used snus at base-line became smokers. This raises the question whether snus to some extent contributes to maintenance of the smoking prevalence, at least in a society with a high proportion of snus users.
Longitudinal data show that tobacco habits are most stable among men with basic education who were 30-years-old at baseline. At 10-year follow-up they were both the most frequent smokers and the most frequent snus users among men. Their female counterparts (30-years-old at baseline) frequently quit smoking, and yet had the highest smoking prevalence at 10-year follow-up. In addition, due to frequent uptake of snus, they were also the most frequent snus users among women. The overall aim of the Swedish national public health policy is to promote good health for the entire population Citation19. Our results underscore the need of new strategies and policies in tobacco control that target less privileged groups, and in particular, the young.
We have shown both a trend of increasing prevalence of dual smoking, that was statistically significant among those with basic education, and also of snus use in this middle-aged population, that in comparison to many other populations have a high prevalence in use of oral tobacco. Previous reports from this region that were based on data from the Northern Sweden MONICA study included 25–64-year-olds and reported dual use among only 2–5% Citation5 Citation8. It was also suggested that dual use is an unstable and transient category, and described it as a transition between smoking and snus use Citation5. If this is true, one would expect combined smoking and snus use to decline in parallel with the decline in smoking alone. Our cross-sectional data indicate that this is not the case (). In all educational groups and in spite of a declining prevalence in smoking, the proportion of those who both smoke and use snus was stable or tended to increase, and reached an age-adjusted 8.3% among men with low education. Moreover, in our longitudinal analysis, although the majority (45%) had switched to snus only, 33% of male and 25% of female dual users were still dual users after 10 years. This shows that dual use is not entirely a transient phenomenon. We hypothesize that dual smoking and snus use, which seems to be more frequent in this population with its high prevalence of snus use, might contribute to continuation of smoking among some smokers. Contrary to previous studies from this population Citation5, and in spite of a higher prevalence of smoking without using snus among women, we also document that the difference in overall prevalence of smoking was small between men and women of all age groups. A higher prevalence of dual use among men contributes to this finding. This should be considered a red flag, and further development of dual use and its role in tobacco use should be followed. The possible consequences from continued combined smoking and snus use are in itself a matter for future research. Dual use might create a vicious circle with more frequent tobacco use and difficulty in quitting tobacco use, and has also been shown to be related to a strong tobacco addiction Citation20 Citation21. Taken together, our findings indicate that the suggestion that snus has the potential to reduce smoking on a population level should be questioned. These data also have implications for tobacco control policies and is relevant for the ongoing discussions with respect to lifting the ban on snus in the European Union.
We grouped intermittent smokers and daily smokers in the smokers’ category, and this should contribute to discrepant results of smoking prevalence compared to previous studies that consider intermittent smokers as non-smokers or exclude them from the analyses. The health hazards associated with smoking increase as exposure increases, and they are well known and documented even at low exposure Citation22. Therefore we question whether intermittent smoking can be regarded as non-smoking. Snus use among intermittent smokers might reflect one stage in a smoking cessation process, if snus during a shorter period is used in parallel with intermittent smoking when a smoker gradually goes from daily smoking to non-smoking. However, this is not supported by a study that demonstrated that intermittent smoking tends to be a long term habit Citation23. Our data cannot separate ‘party smoking’ from smoking 6 days a week, which would also be categorized as intermittent smoking. Further studies targeting the nature of intermittent smoking and its relation to relapses and snus use and dual tobacco use are warranted.
Our cross-sectional and longitudinal results, as well as findings of previous studies Citation6 Citation8 Citation24, show that using snus is a more stable habit than is smoking. Even though research on possible health effects from snus are inconclusive and limited and the studies often underpowered Citation25, there are results that raise concerns. For example, associations are found between snus use and pancreatic cancerCitation26, fatal myocardial infarction Citation27, fatal stroke Citation28, obesity Citation29 Citation30, and hypertension Citation31. Scientific evidence on the harms of smoking started to be compiled in the 1950s but it took decades before consensus was reached by the scientific community. Similarly, it might also take long time until the evidence on risks from snus use are established. It is clear that the health hazards from snus are much smaller than those from smoking. However, even small risks associated to the use of snus may be serious enough to cause public health problems in populations with high snus use prevalence Citation32.
Age-adjusted smoking prevalence only differed slightly between men and women within each educational group, with the exception of those with basic education. This might contribute to increasing health inequalities between men and women with basic education as they grow older, and is in agreement with other Swedish Citation15 and European studies Citation16. Also noteworthy is that in the younger age group with high education, the men were both the most frequent smokers and snus users, and this might contribute to future worsening health among highly educated men as compared to women.
The low prevalence of daily smoking in Sweden has by some been attributed to the use of snus Citation6 Citation33 Citation34. However, the decline in smoking has been equally dramatic in other developed countries where snus is not available, e.g. Canada has a prevalence of smoking that is lower among both men and women compared to Sweden Citation3. Data from the US, where smokeless tobacco is widely available, also show that male and female US smokers have higher cessation rates than Swedish smokers despite a higher prevalence of snus use in Sweden Citation35. Since the early 2000s, a higher proportion of 40-year-old men who use snus are never-smokers rather than former smokers. The use of snus among women has increased most in the younger groups and these women are primarily former-smokers.
Taken together these data demonstrate the ongoing transition from smoking to using snus among Swedish tobacco consumers, and tobacco consumers remain a relatively stable proportion of the population. Our finding that a considerably larger proportion (84%) of female former smokers succeeded in smoking cessation without any use of snus, compared to 38% of men is in line with previous Swedish findings which showed that most smokers who quit smoking do not take up snus Citation9 Citation36. The fact that during 2002–2007, 40-year-old female former smokers had a history of snus use that was similar to that found in 60-year-old male former smokers during 1990–1995, illustrates that snus as a smoking cessation aid is a time-bound and gender-linked phenomenon and rather the result of trends in norms and attitudes. The driving forces in the development of increasing use of snus in Sweden may be a combined effect of successful marketing and weak tobacco control policies with regard to snus use, as well as current limited evidence regarding the effects of snus on public health.
It should be observed that this is a very large study including almost 100,000 subjects. As a consequence, it is relatively easy for even a small difference to attain statistical significance. However, this does not mean that they should be considered relevant. What is relevant from a public health perspective is rather a question of judgement. Overall we have described differences as ‘small’ if they are only a few percentages regardless of statistical significance. This study has the strengths of being large-scale, long-term, performed in a setting where health surveys target the whole middle-aged population without any selection, and are integrated into primary care routines. This allows for population-based measurements with high participation rates in both cross-sectional and longitudinal standardized surveys. One limitation is that only middle-aged adults are included, and thus our conclusions are restricted to the ages of 30–60 years. The drop-out analysis was in line with a previous analysis Citation37and showed that those who participated initially but not in follow-up were more likely to be young, men, smokers, and snus users but with minimal difference in education. Although we consider these differences to be small, they suggest that our results should be conservative and not overestimate tobacco, especially among men and the younger age groups. Determinants and patterns of intermittent smoking and dual tobacco use should be studied further. Qualitative methodology might be appropriate for such research.
In conclusion, both cross-sectional and longitudinal analyses show that there are increasing differences in tobacco use between educational groups in this middle-aged population. Higher prevalence rates exist for both smoking and snus use among those with basic education compared to those with mid-level and higher education. These differences are most marked in the younger men and women. Therefore better tobacco control strategies are needed that target the young. In spite of a higher prevalence of only smoking among women, a higher prevalence of dual use among men contributes to similar smoking prevalence rates in men and women. Dual smoking and snus use is slowly increasing in parallel to a high prevalence of snus use, and among dual users one out of three of men and one out of four women are still dual users after 10 years of follow-up. The role of snus in dual use and intermittent smoking should be investigated in further studies.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this research.
Acknowledgements
This study was supported by the Västerbotten County Council. Statistical expertise was provided by senior lecturer Hans Stenlund.
Related Research Data
References
- WHO. (2008). Fresh and alive: WHO report on the global tobacco epidemic. Geneva: World Health Organisation. Available from: http://www.who.int/tobacco/mpower/mpower_report_full_2008.pdf [cited 9 December 2009].
- WHO. (2009). Implementing smoke-free environments: WHO report on the global tobacco epidemic. Geneva: World Health Organisation. Available from: http://whqlibdoc.who.int/publications/2009/9789241563918_eng_full.pdf [cited 10 March 2010].
- Shafey O, Eriksen M, Ross H. Mackay J. The tobacco atlas. 3rd ed. Available from: http://www.cancer.org/docroot/AA/content/AA_2_5_9x_Tobacco_Atlas_3rd_Ed.asp [cited 23 March 2010].
- SCB. (2007). Survey on living conditions (ULF). Daily smoking. Stockholm. Available from: http://www.scb.se/Pages/TableAndChart____48675.aspx [publisher] [cited 23 March 2010].
- Stegmayr B, Eliasson M, Rodu B. The decline of smoking in northern Sweden. Scand J Public Health. 2005; 33: 321–4. 10.3402/gha.v4i0.5613.
- Rodu B, Stegmayr B, Nasic S, Cole P, Asplund K. Evolving patterns of tobacco use in northern Sweden. J Intern Med. 2003; 253: 660–5. 10.3402/gha.v4i0.5613.
- Foulds J, Ramstrom L, Burke M, Fagerstrom K. Effect of smokeless tobacco (snus) on smoking and public health in Sweden. Tob Control. 2003; 12: 349–59. 10.3402/gha.v4i0.5613.
- Rodu B, Stegmayr B, Nasic S, Asplund K. Impact of smokeless tobacco use on smoking in northern Sweden. J Intern Med. 2002; 252: 398–404. 10.3402/gha.v4i0.5613.
- Gilljam H, Galanti MR. Role of snus (oral moist snuff) in smoking cessation and smoking reduction in Sweden. Addiction. 2003; 98: 1183–9. 10.3402/gha.v4i0.5613.
- Lundqvist G, Sandstrom H, Ohman A, Weinehall L. Patterns of tobacco use: a 10-year follow-up study of smoking and snus habits in a middle-aged Swedish population. Scand J Public Health. 2009; 37: 161–7. 10.3402/gha.v4i0.5613.
- Tomar SL, Connolly GN, Wilkenfeld J, Henningfield JE. Declining smoking in Sweden: is Swedish Match getting the credit for Swedish tobacco control's efforts?. Tob Control. 2003; 12: 368–71. 10.3402/gha.v4i0.5613.
- Benowitz NL. Systemic absorption and effects of nicotine from smokeless tobacco. Adv Dent Res. 1997; 11: 336–41. 10.3402/gha.v4i0.5613.
- Henningfield JE, Fant RV. Tobacco use as drug addiction: the scientific foundation. Nicotine Tob Res. 1999; 1(Suppl 2):31–5. 10.3402/gha.v4i0.5613.
- Norberg M, Wall S, Boman K, Weinehall L. The Västerbotten intervention programme: background, design and implications. Global Health Actio. 2010; 3: 4643. 10.3402/gha.v4i0.5613.
- Ali SM, Chaix B, Merlo J, Rosvall M, Wamala S, Lindstrom M. Gender differences in daily smoking prevalence in different age strata: a population-based study in southern Sweden. Scand J Public Health. 2009; 37: 146–52. 10.3402/gha.v4i0.5613.
- Giskes K, Kunst AE, Benach J, Borrell C, Costa G, Dahl E, et al.. Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. J Epidemiol Community Health. 2005; 59: 395–401. 10.3402/gha.v4i0.5613.
- Schaap MM, Van Agt HM, Kunst AE. Identification of socioeconomic groups at increased risk for smoking in European countries: looking beyond educational level. Nicotine Tob Res. 2008; 10: 359–69. 10.3402/gha.v4i0.5613.
- Schulze A, Mons U. The evolution of educational inequalities in smoking: a changing relationship and a cross-over effect among German birth cohorts of 1921–70. Addiction. 2006; 101: 1051–6. 10.3402/gha.v4i0.5613.
- Government Offices of Sweden [En förnyad folhälsopolitik]. In: Affairs ministry of health and social affairs 2008. Available from: http://www.regeringen.se/content/1/c6/10/09/78/2ee01484.pdf [cited 10 March 2010].
- Tomar SL, Alpert HR, Connolly GN. Patterns of dual use of cigarettes and smokeless tobacco among U.S. males: findings from national surveys. Tob Control. 2010; 19: 140–9. 10.3402/gha.v4i0.5613.
- Post A, Gilljam H, Rosendahl I, Bremberg S, Galanti MR. Symptoms of nicotine dependence in a cohort of Swedish youths: a comparison between smokers, smokeless tobacco users and dual tobacco users. Addiction. 2010; 19: 740–6. 10.3402/gha.v4i0.5613.
- Bjartveit K, Tverdal A. Health consequences of smoking 1–4 cigarettes per day. Tob Control. 2005; 14: 315–20. 10.3402/gha.v4i0.5613.
- Lindstrom M, Isacsson SO. Long term and transitional intermittent smokers: a longitudinal study. Tob Control. 2002; 11: 61–7. 10.3402/gha.v4i0.5613.
- Furberg H, Lichtenstein P, Pedersen NL, Bulik C, Sullivan PF. Cigarettes and oral snuff use in Sweden: prevalence and transitions. Addiction. 2006; 101: 1509–15. 10.3402/gha.v4i0.5613.
- Hatsukami DK, Lemmonds C, Tomar SL. Smokeless tobacco use: harm reduction or induction approach?. Prev Med. 2004; 38: 309–17. 10.3402/gha.v4i0.5613.
- Luo J, Ye W, Zendehdel K, Adami J, Adami HO, Boffetta P, et al.. Oral use of Swedish moist snuff (snus) and risk for cancer of the mouth, lung, and pancreas in male construction workers: a retrospective cohort study. Lancet. 2007; 16(369):2015–20. 10.3402/gha.v4i0.5613.
- Hergens MP, Alfredsson L, Bolinder G, Lambe M, Pershagen G, Ye W. Long-term use of Swedish moist snuff and the risk of myocardial infarction amongst men. J Intern Med. 2007; 262: 351–9. 10.3402/gha.v4i0.5613.
- Hergens MP, Lambe M, Pershagen G, Terent A, Ye W. Smokeless tobacco and the risk of stroke. Epidemiology. 2008; 19: 794–9. 10.3402/gha.v4i0.5613.
- Hergens MP, Ahlbom A, Andersson T, Pershagen G. Swedish moist snuff and myocardial infarction among men. Epidemiology. 2005; 16: 12–6. 10.3402/gha.v4i0.5613.
- Norberg M, Stenlund H, Lindahl B, Boman K, Weinehall L. Contribution of Swedish moist snuff to the metabolic syndrome: a wolf in sheep's clothing?. Scand J Public Health. 2006; 34: 576–83. 10.3402/gha.v4i0.5613.
- Hergens MP, Lambe M, Pershagen G, Ye W. Risk of hypertension amongst Swedish male snuff users: a prospective study. J Intern Med. 2008; 264: 187–94. 10.3402/gha.v4i0.5613.
- Rose G. Sick individuals and sick populations. Int J Epidemiol. 2001; 30: 427–32. 10.3402/gha.v4i0.5613.
- Ramstrom LM, Foulds J. Role of snus in initiation and cessation of tobacco smoking in Sweden. Tob Control. 2006; 15: 210–4. 10.3402/gha.v4i0.5613.
- Stenbeck M, Hagquist C, Rosen M. The association of snus and smoking behaviour: a cohort analysis of Swedish males in the 1990s. Addiction. 2009; 104: 1579–85. 10.3402/gha.v4i0.5613.
- Zhu SH, Wang JB, Hartman A, Zhuang Y, Gamst A, Gibson JT, et al.. Quitting cigarettes completely or switching to smokeless tobacco: do US data replicate the Swedish results?. Tob Control. 2009; 18: 82–7. 10.3402/gha.v4i0.5613.
- Lundqvist G, Sandstrom H, Ohman A, Weinehall L. Patterns of tobacco use: a 10-year follow-up study of smoking and snus habits in a middle-aged Swedish population. Scand J Public Health. 2009; 37: 161–7. 10.3402/gha.v4i0.5613.
- Nafziger AN, Lindvall K, Norberg M, Stenlund H, Wall S, Jenkins PL, et al.. Who is maintaining weight in a middle-aged population in Sweden? A longitudinal analysis over 10 years. BMC Public Health. 2007; 7: 108.10.3402/gha.v4i0.5613.
