Abstract
Significant funding of health programs in low-income countries comes from external sources, mainly private donors and national development agencies of high-income countries. How these external funds are allocated remains a subject of ongoing debate, as studies have revealed that external funding may misalign with the underlying disease burden. One determinant of the priorities set by both private donors and development agencies is the perceptions of populations living in high-income countries about which diseases are legitimate for global health intervention. While research has been conducted on the priorities expressed by recipient communities, relatively less has been done to assess those of the donating country. To investigate people's beliefs about the disease burden in high-income countries, we compared publicly available data from U.S. surveys of people's perceptions of the leading causes of death in developing countries against measures of the actual disease burden from the World Health Organization. We found little correlation between the U.S. public's perception and the actual disease burden, measured as either mortality or disability-adjusted life years. While there is potential for reverse causality, so that donor programs drive public perceptions, these findings suggest that increasing the general population's awareness of the true global disease burden could help better align global health funding with population health needs.
Significant funding of global health programs comes from ‘external sources,’ mainly private donors and national development agencies. How these external funds are allocated remains a subject of ongoing debate. Several recent studies have revealed that external funding can create misalignments in allocations with the underlying disease burden, even in organizations with a health mandate such as the World Health Organization (WHO) Citation1 Citation2 Citation3 Citation4 . This potential misalignment of global health funding can arise in several ways. In the case of private donors, it may stem from the priorities of the donating individuals and their families; in the case of national development agencies, these priorities are often explicitly set in the interest of the donating country Citation5 Citation6.
One potential check on the priorities set by both private donors and development agencies comes from the perceptions of ordinary people living in high-income countries about what is the legitimate scope of global health intervention. The general public may directly influence private donors by committing to charitable giving, out of a sense of concern, guilt, or genuine compassion. The public's influence is also indirect. A favorable perception of charitable efforts confers goodwill and positive reputation on private donors and, in democratic polities, the public's support is crucial for raising the tax revenues required to finance global health programs.
It is therefore relevant to ask, what do ordinary people in high-income countries believe are the leading causes of poor health in the developing world? If their perceptions about the burden of disease are inaccurate, it would be unsurprising if so too were their priorities – and those of the private donors and national development agencies influenced by them – misaligned with the health needs of people living in developing countries.
To shed light on the general population's underlying beliefs in high-income countries, we compared publicly available data from a demographically representative survey of American adults, one of the largest pools of global health donors, about their perceptions of the leading causes of death in the developing world against measures of the actual disease burden. Data were taken from a Research!America survey of Americans perceptions about the leading causes of death in developing countries, drawn from a representative sample of 1,000 US adults (aged 18 and older) through online polls in the year 2006 Citation7. Although online sampling can lead to a biased sample as it typically includes more highly educated members of the population, such bias would likely skew the responses to be closer to the actual situation. Data for the actual causes of death comes from the most recent estimates from the WHO's Global Burden of Disease study for the year 2004 Citation8.
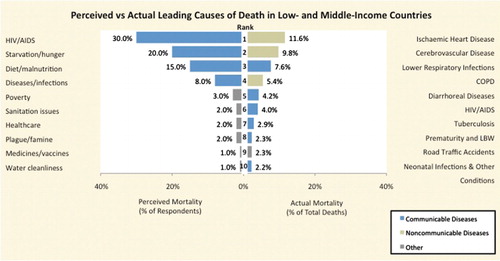
As shown in , there appeared to be little correlation between the American public's perception of the leading killers and the actual disease burden. HIV/AIDS was perceived to be the leading cause of death (30% of respondents rank it as the leading cause of death in low- and middle-income countries), although HIV/AIDS only accounted for about 4% of all deaths in low- and middle-income countries in the year 2004. On the other hand, the leading killer was heart disease (including ischemic heart disease and cerebrovascular disease) worldwide, yet none of the respondents ranked heart disease as the leading cause of death. Similar misalignment was observed when using alternative metrics of the disease burden, including premature mortality and years of life lived with disability (the two main components of disability-adjusted life years, not shown).
Fig. 1. Perceived vs actual leading causes of death in low- and middle-income countries.
Sources: Research!America's November 2006 ‘Attitudes: Global Health Research’ survey (No. 1279c), conducted by Charlton Research (available at http://www.researchamerica.org). Respondents were asked ‘What do you think are the two leading causes of death in [poor or developing countries/countries other than the US]?’ Mortality data is from the Global Burden of Disease (GBD) Study 2004 Update (2008), available at http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/index.html. The GBD defines low-income countries as those with a gross national income per capita of $825 or less and middle-income countries as those with a gross national income of less than $10,066. The Communicable Diseases category includes maternal and perinatal conditions and nutritional deficiencies. The diseases/infections category refers to general infections/illnesses. The sanitation issues category includes sanitation issues and living conditions. The health care category includes health care coverage and insurance. The medicines/vaccines category includes medical supplies, medicines, and vaccinations. The stroke category includes stroke and other cerebrovascular diseases. The violence/suicide category includes crime, murder, violence, and suicide. COPD, Chronic Obstructive Pulmonary Disease; LBW, Low Birth Weight.
Several important caveats apply to our observations. One is that the causes of death according to survey respondents are imperfectly comparable with the epidemiologic categories of WHO Global Burden of Disease Study. Nonetheless, the overall picture shows a clear pattern where the perceptions of Americans perceive infectious diseases and inadequate food to be leading causes of death. In general, these perceptions appear to lag behind the so-called ‘epidemiologic transition’ occurring in developing countries whereby chronic non-communicable diseases increasingly account for a greater share of the disease burden. This potential lag in the public's consciousness may reflect enduring dispositions created by social marketing of famine in the 1980s and the tremendous health burden posed by the spread of HIV in the 1990s, which coincided with a massive increase in resources for global health from western donors. A second limitation is that our study can only show misalignment but not identify its causes. It is possible that Americans’ perceptions simply reflect the prevailing funding patterns and marketing of global health programs and have little or no influence over global health priorities (‘reverse causality’). However, in democratic systems, popular perceptions may in turn influence which issues donors as well as national development agencies choose to adopt as priorities. If this is the case, perversely, the current state of imbalance could create a self-perpetuating situation, whereby existing global health priorities lock in popular perceptions.
To our knowledge, this analysis is among the first to compare actual health situation in developing countries with the perceptions of a large pool of health donors. It suggests that, if policymakers wish to better align global health funding with the avoidable burden of disease, they should begin to account for the general public's views. Analogously, the climate change movement is beginning to adopt social marketing approaches to address mismatches between public perceptions of climate change and the actual situation Citation9. Until global health awareness is consistent with global health reality, misalignments between aid and the disease burden may continue. Future research is needed to better understand the drivers of these perceptions about global health and how to align them more closely to the health care realities confronting at-risk populations in developing settings.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Acknowledgements
KRS, ABF, and DS analyzed the data and drafted the manuscript; SPK, ABF, and DS helped to revise the manuscript. All authors agreed to the final version.
References
- Stuckler D, King L, Robinson H, McKee M. WHO's budgetary allocations and burden of disease: a comparative analysis. Lancet. 2008; 372: 1563–69.
- Sridhar D, Batniji R. Misfinancing global health: a case for transparency in disbursements and decision making. Lancet. 2008; 372: 1185–91.
- Ravishankar N, Gubbins P, Cooley RJ, Leach-Kemon K, Michaud CM, Jamison DT, et al.. Financing of global health: tracking development assistance for health from 1990 to 2007. Lancet. 2009; 373: 2113–24.
- Nugent R, Feigl A. Where have all the donors gone? Scarce donor funding for non-communicable diseases working paper 228. Center for Global Development. Washington DC, 2010
- Benatar SR. Imperialism, research ethics and global health. J Med Ethics. 1998; 24: 221–22.
- Watch GH. Global health watch 2. Zed Books. London, 2009
- Research!America. Complete poll history. AlexandriaVA: Research!America. 2006. Available from: http://www.researchamerica.org/poll_history [cited 13 January 2011]..
- WHO. Global burden of disease study (2004). Geneva: World Health Organisation. 2009.
- Campbell-Lendrum D, Bertollini R. Science, media and public perception: implications for climate and health policies. Bull World Health Org. 2010; 88: 242.
