Background
Research on reproductive health in developing countries focuses mostly on the role of economic development on various components of reproductive health. Cross-sectional and empirical research studies in particular on the effects of non-economic factors such as reproductive rights remain few and far between.
Objective
This study investigates the influence of two components of an empowerment strategy, gender equality, and reproductive rights on women's reproductive health in developing countries. The empowerment strategy for improving reproductive health is theoretically situated on a number of background factors such as economic and social development.
Design
Cross-national socioeconomic and demographic data from a number of international organizations on 142 developing countries are used to test a model of reproductive rights and reproductive health.
Results
The findings suggest that both economic and democratic development have significant positive effects on levels of gender equality. The level of social development plays a prominent role in promoting reproductive rights. It is found that reproductive rights channel the influences of social structural factors and gender equality on reproductive health.
Economic development brought about by industrialization and modernization is believed to be a prime factor in the overall improvement of quality of life and health in developing countries Citation1 Citation2. Decline in fertility, as well as morbidity and mortality, is also expected to accompany economic development Citation3. In countries such as India, an excessive focus on ways and means to ensure economic development produced some of the most well-recorded violations of human rights in modern history Citation4. Consequently, economic development policies for improving reproductive health are now subjected to the scrutiny of human rights groups and agencies at the national as well as international levels Citation5 Citation6 Citation7 . However, rights-based theories of reproductive health have not been adequately tested. World Health Organization Citation8 defines reproductive rights as a basic right of all couples and individuals to decide freely and responsibly the number, spacing, and timing of their children and to have the information and means to do so, and the right to attain the highest standard of sexual and reproductive health.
The objective of this article is to test a model of reproductive health in developing countries. First, we provide a theoretical framework for investigating the relationships among economic development, reproductive rights, and reproductive health. Next, we put forth a number of testable propositions contributing to a growing body of research on the structural basis of the reproductive rights–reproductive health relationship.
Theoretical approach
Reproductive health implies that people are able to have a responsible, satisfying, and safe sex life and that they have the capability to reproduce and the freedom to decide if, when, and how often to do so. Literature on reproductive health in developing countries shows a strong positive relationship between economic development and reproductive health Citation9 Citation10. Economic development is associated with improvement in public health as well as women's health Citation11. Currently, a small share of the support for economic development programs and projects in developing countries through the World Bank is targeted toward improving general nutritional and health standards Citation12.
The term ‘reproductive rights’ is of relatively recent origin. For roughly a decade after its introduction at the International Meeting on Women and Health in Amsterdam 1984, its impact remained limited to state actions in support of women's reproductive well-being. However, almost a decade later, the 1993 World Conference on Human Rights, held in Vienna, and the 1995 Fourth World Conference on Women in Beijing clearly publicized the positive relationship between the level of reproductive rights and reproductive health Citation13 Citation14 Citation15 Citation16 Citation17 Citation18 Citation19 Citation20 . The choices women make, with respect to reproductive health, can be broadened and realized only in the presence of a wide variety of reproductive rights Citation21 Citation22 Citation23 Citation24 Citation25 .
Current theoretical perspectives on reproductive rights place strong emphasis on social structural correlates. Several feminist scholars Citation26 Citation27 Citation28 Citation29 have pointed out that at low levels of social development, women's low socioeconomic status leaves them with few choices for decision making with respect to several aspects of the reproductive process: intercourse, contraception, and gestation.
The unequal distribution of power across gender resulting in gender inequality and undesirable constraints over social and economic opportunities influence the level of reproductive rights Citation6 Citation30 Citation31. Both gender equality and social development are seen as important structural correlates of reproductive rights. Social development tends to facilitate a broad level of participation spanning all levels of social institutions. Citizen participation at all societal levels can take place only when social transactions are bound by values of social justice and equality. To this extent, social development programs are guided by a social justice framework. A broadening set of opportunities for social participation is a function of social development Citation32.
At the individual level, social development is purported to promote quality of life Citation33. An expansion of choices that people enjoy to improve their own welfare requires vast social institutional development over and above mere economic development. Improvement in social participation increases individual's substantive freedoms or capabilities Citation34. Lack of democratic freedom, the press, and the absence of agencies that represent people's voices are all characteristic of unfreedom, which citizenship theorists suggest are associated with low levels of social development. At higher levels of social development, social participation is sustained by improving availability and universal access to societal resources necessary to realize a number of social choices that individuals make. With social development, human rights are valued and recognized Citation35 Citation36 Citation37 Citation38 . In general, there is a positive relationship between the level of social development and the reproductive rights level.
The gender differences in social power and gender equality influence the extent of rights women have, including reproductive rights Citation30. The removal of gender inequality through empowerment, in developing countries, is one among the eight Millennium Development Goals. As gender equality improves, the amount of power women exert collectively – to bargain and acquire desired resources – is likely to increase Citation16 Citation39 Citation40 and result in a vast expansion of opportunities for women to make realistic social and personal choices. The active pursuit of these choices involves both the demand for new rights necessary for enjoying reproductive health Citation41 and the dismantling of existing and emerging discriminatory legal practices limiting the expansion of reproductive choices. Thus, improving gender equality is likely to result in increases in women's rights in general and reproductive rights in particular.
Within the democratic setting, women's agencies are much more likely to develop the capacity to make effective demands on the state to effect gender equality Citation42 Citation43 Citation44 Citation45 . It is well known that the development of democratic institutions is associated with economic development and value changes with respect to women's roles in the public sphere. As support for democratic ideals increases, women are more likely to gain political power Citation46 and in the long term gender equality at the institutional level. Squires Citation47 suggested that programs and policies to enhance gender equality should ‘draw upon the resources developed within democratic theory.’ As societies develop strong democratic institutions, the level of gender equality is also likely to improve.
There is a positive relationship between economic development and gender equality Citation48 Citation49. Economic development is accompanied by shifts in several values such as transfer of status through inheritance widespread among agricultural communities to achievement orientation among the industrial Citation50. With modernization, attitudes toward women's roles also tend to become less conservative, enabling women to pursue education and seek outside employment in the wage economy Citation50. As the economy grows, women are expected to make considerable gains in their collective social status, and the socioeconomic gap between men and women is likely to either disappear or become insignificant. Accordingly, these theories suggest that there is a positive relationship between economic development and gender equality.
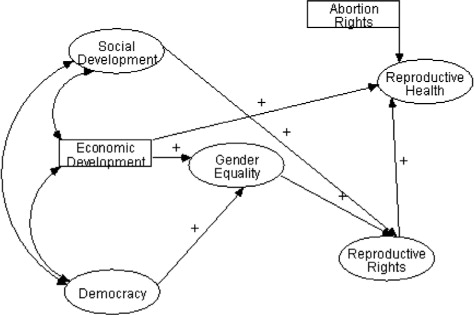
presents the theoretical relationships among the various factors in the proposed model of reproductive health and reproductive rights.
Fig. 1. A rights-based model of reproductive health in developing countries.
Materials and methods
The proposed model of reproductive health contains four latent constructs, social development, gender equality, democracy, reproductive rights, reproductive health, and two variables, economic development and abortion rights. The reproductive rights dimension consists of two subdimensions, social rights related to reproduction and abortion rights. Factors influencing social rights appear to be significantly different from the determinants of level of abortion rights Citation51. No attempt has been made in this study to identify the influences on abortion rights; instead, the focus is on social rights associated with reproductive health. presents the definitions of variables used in this study.
Table 1. Variables and their definitions
The term developing countries in this study includes all nations with a per capita income below 3,600 US Dollars in 2004. One hundred and forty-two countries fall into the category of developing countries in the lower middle income category or lower.
Analysis
Analysis is conducted in two stages. In the first stage, we address a number of measurement issues related to the proposed model followed by its estimation.
The descriptive statistics for all the variables are provided in . The average maternal mortality rate is approximately 277 deaths per 100,000 births, a rate at least 16 times higher than that of the United States in 2000. Very few variables have large number of missing cases. One of the techniques for handling missing data is single imputation using Expectation Maximization (EM) algorithm. This method is used to impute missing values. An advantage of this method is that it produces reliable Citation52 Footnote1 estimates.
Table 2. Descriptive statistics for all variables in the reproductive rights–reproductive health modela
Because multivariate methods are essential for the testing models such as the one presented here, we initiate data analysis with a number of procedures for testing some of the basic statistical assumptions of the proposed model. Multivariate techniques assume that variables in the model are normally distributed. To test the assumption of multinormality of the variables in the model, measures of skewness and kurtosis were obtained and compared against the norms for skewness and kurtosis of an ideal normal distribution. None of the indicators in the model were affected by extreme skewness.
The model proposed in this study presented five latent constructs: democracy, social development, gender equality, reproductive rights, and reproductive health. The measurement of each of these constructs involves theoretically justified indicators. The appropriateness of the selected indicators may be examined by assessing the validity and reliability of each of the latent constructs. A preliminary approach toward assessing the construct validities involves the use of factor analysis. Principal component analysis was conducted with varimax rotation.
The principal component analysis of variables in the reproductive rights–reproductive health model did not indicate the presence of factorial validity for social development scale. The variables assigned to the ‘social development factor’ cross correlated with a number of other indicators of factors such as reproductive health and gender equality. Specifically, social development variables had high loading on the reproductive health factor. That is, three of the hypothesized indicators of social development had strong loading on the reproductive health factor.
The results from factor analysis suggest that reproductive health indicators are correlated with the indicators of social development. It is necessary to establish factorial validity of reproductive health construct, as it is an endogenous factor of crucial importance to the theoretical model in this article. This issue is addressed in the course of analysis that follows.
Confirmatory factor analysis methods Citation53 provide an array of tests and procedures for assessing the factorial validity of the latent constructs in the model. The confirmatory factor analysis results are reported in . The table presents the factor loading, scale reliability, and goodness of fit indices. The factor loadings are regressions coefficients (standardized) of the indicators to which they are theoretically related. All the factor loadings are greater than 0.3, except for GINI1 and SEAT. The measurement characteristics of the constructs are further analyzed by deriving the construct (scale) reliabilities. It is assumed that any one indicator alone is insufficient to measure the construct. Nunnaly Citation54 had argued that scale reliabilities should be approximately 0.6 or above. All scale reliabilities are approximately 0.6 or above except for the reliability value of ‘democracy.’
Table 3. Factor loadings, reliability, and goodness of fit of variables from measurement models for the latent constructs in the reproductive rights–reproductive health model
The goodness of fit indicators are useful to assess how well the hypothesized measurement model fits data. There are several fit indices available. The current practice is to refrain from using any one single goodness of fit index. Values indicating good fit are expected from all three measures to conclude that the measurement model has the desired level of goodness of fit. The three selected indicators are Comparative Fit Index (CFI), root mean square error of approximation (RMSEA), and Hoelter's Index. The comparative fit index is chi-square based. The desirable values range from 0.90 to 1.00. RMSEA is also chi-square based, with values greater than 0.1 suggesting poor fit. Hoelter's Index asserts the sample size at which chi-square would not be significant. The index is, therefore, used only when the model chi-square is significant. Index values less than 75 indicate very poor fit between the model and data Citation55.For all measurement models, values from the three goodness of fit indexes provided uniform support, with the exception of ‘democracy.’ Two indexes suggested good fit, whereas the third, RMSEA, indicated poor fit. In general, it can be stated that most of the constructs in the model are adequately measured.
The construct ‘social development’ has a good fit indicating the presence of construct validity. However, during the course of principal component analysis, it was noted that ‘social development’ variables loaded on the ‘reproductive health’ component. This raises issues with respect to the factorial validity of reproductive health, which is a crucial variable in this study. To ascertain the extent of influence of reproductive health factors on social development, it is appropriate to further investigate the factor structure of social development and reproductive health.
If social development variables are also valid indicators of reproductive health, a single construct model, with all the social development variables coupled with reproductive health indicators, is likely to yield high goodness of fit. An alternate explanation is that reproductive health and social development are separate constructs with moderate covariation. Confirmatory factor analysis is used to test these two competing hypotheses. The results of the test of the two hypotheses are presented in . When social development variables are added to reproductive health variables in a one-construct hypothesis, the model fit is poor. The RMSEA is 0.116. The test of the alternate hypothesis also yields poor goodness of fit values. These results suggest that including social development variables with reproductive health indicators diminishes the construct validity of reproductive health. Consequently, it appears more appropriate to treat the two constructs, reproductive health and social development, as independent.
Table 4. Validating hypothesis that reproductive health–social developmentis a two factor model versus it is one factor model
A common issue that plagues cross-national data is the presence of outliers. They are problematic when they influence regression parameters. To test if there are outliers, Cook's test was conducted. The test utilizes the Cook's distance measure, which is an index of change in the parameter estimates when one observation at a time is dropped from the analysis. The Cook's distance values D i>F(1−α,p,n−p) where p is the number of independent variable in the model and n is the number of cases that are marked as outliers. The Cook's Statistics (Di) is compared with percentiles from an F distribution. The level of confidence is often fixed as high as 0.8 or 0.9. In this study, it was fixed at 0.8. Cook's test was conducted using two independent variables, reproductive rights and economic development, which directly influence the level of reproductive health. We found one country, Equatorial Guinea, with a high Cook's value. To examine which of the two independent variables had an outlying case that significantly influenced the slope parameter; we looked at the DFBETA for the two variables that influence reproductive health. It was discovered that one case, Equatorial Guinea, had significantly influenced the slope of the GDP per capita (GDPIND) variable.
To investigate the relationships among proposed concepts taking into account measurement errors in the model, a structural equation analysis is conducted. Because there is an indication that ‘Equatorial Guinea’ may be an outlier case, in the analysis that follows two types of models will be examined; one including Equatorial Guinea and another excluding it. The direction and strength of the parameter estimates derived from the two models will be examined to assess if there are significant differences.
presents the results of Structural equation analysis of the proposed model, and presents the hypothesized model to be tested using Structural Equation Modeling (SEM).
Fig. 2. Structural equation model of reproductive rights and reproductive health.Footnote3 See Table 3 for variable names of latent constructs.
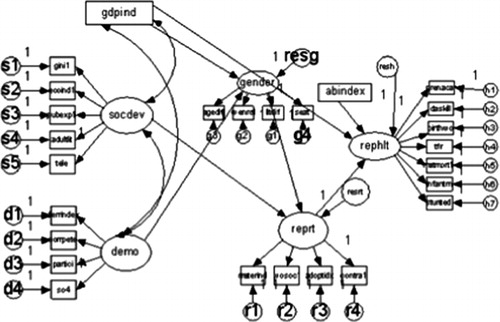
Table 5. Structural equation analysis of reproductive rights–reproductive health model: structural parameter estimates (standardized)
The effect of economic development on reproductive health is insignificant, and the coefficient is negative. A positive effect was expected. As expected, the relationship between economic development and gender equality is positive and significant at 0.5 level. The democracy factor has a substantial positive effect on gender equality. Social development has a positive and significant effect on reproductive rights. The hypothesized positive relationship between reproductive health and reproductive rights is also supported. Availability of abortion measured by the variable ‘Abortion index’ has a positive and significant effect on reproductive health. The goodness of fit indicators suggest a moderate fit. In particular, the RMSEA value is nearly 0.06. Values above 0.10 suggest poor fit. The results provide partial support to the proposed theory of reproductive rights and reproductive health.
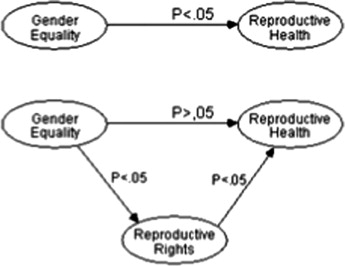
The effects of background factors, such as democracy, social development, and gender equality, influence reproductive health through reproductive rights. Thus, reproductive rights play a monumental role in translating several aspects of broad-based sociopolitical changes into gains in women's reproductive health in developing countries. The role of reproductive rights as a mediating variable in the SEM model was further explored as follows. The direct effect between gender equality and reproductive health is nearly 0.156, significant at the 0.05 level. When reproductive rights are introduced in the model along with gender equality, the relationship between gender equality and reproductive health disappears, suggesting that reproductive rights explain the relationship between gender equality and reproductive health (see ).Footnote2
Fig. 3. Reproductive rights as a mediating variable.
Discussion and conclusion
The findings in this study support an emerging set of results from investigations on the relationship between reproductive rights and reproductive health. Several studies have revealed that reproductive rights are significantly related to reproductive health at the cross-national level Citation56 Citation30 Citation57 Citation58 Citation59 Citation31 Citation60.
It is shown that social development plays a prominent role in promoting reproductive rights. At a theoretical level, discussion on the structural determinants of reproductive rights has focused on the influence of political and economic development Citation58 Citation31. This popular thesis that economic development cultivates reproductive health did not receive adequate statistical support. Instead, we found that social development programs, such as those targeted toward lessening social inequality and improving telecommunication, are likely to promote levels of reproductive rights in developing countries. Thus, social developmental projects and programs are vital for supporting a rights-based approach toward improving reproductive health.
The empirical support for the relationship between gender equality and growth of democratic institutions is indeed useful for the development of a theory of gender equality. Sen Citation61 suggested that emergence of democracy as a valued system of good governance has increased opportunities for the socially and economically marginalized to access valuable scarce resources and also benefit from them. He further argued Citation61 that cooperative strategies often supported through the development of democratic institutions tend to reduce gender inequality and promote women's reproductive choices Citation62. Improving women's representation in government through democratic processes and ensuring attention to women's risks, issues, and concerns pave the way for gender equality.
The role of gender equality in improving women's reproductive health has been widely recognized both at the theoretical and the policy level. Among the eight Millennium Development Goals, the third Millennium Development Goal is to ‘Promote gender equality and empower women.’ Improving reproductive rights is an aspect of empowerment. The Millennium Development Goal aims to achieve gender equality and reproductive rights, even though the term ‘reproductive rights’ is not explicitly used. Gains in reproductive rights are sought through empowerment. Improving gender equality and lessening power imbalances with men is an integral part of achieving reproductive rights Citation16, a relationship recognized by the Millennium Development Goals. To draw on reproductive rights, a number of social conditions that enable women to exercise their reproductive choices must be present. They must be presented with realistic opportunities to gain access to social and economic resources. We found that gender equality has a positive and significant effect on reproductive rights. Even though the Millennium Development Goals do not discriminate between the concepts of gender equality and reproductive rights, our finding suggests that gender equality is not only associated with empowerment but also has an effect on reproductive rights.
Two broad social structural factors influence the level of gender equality. Economic development and democracy have significant positive effects on levels of gender equality.
Equality is not possible until women are empowered to recognize their needs as democratic citizens. One of the most important preconditions for the growth of gender equality is the emergence of democracy Citation63. Democratic societies are more likely to seek reproductive health goals through cooperative strategies Citation61. Research on Africa and Latin America indicates that the democratization process generally facilitates a broad-based gender equality agenda Citation64 Citation65 Citation66 Citation43 and opens avenues for women to negotiate for independence and pursue initiatives for social change Citation67 Citation68.
A surprising finding was that economic development had no effect on reproductive health. Economic development, however, had an indirect effect on reproductive health through gender equality. Gender equality is an important outcome as it is mediates the relation between economic development and economic rights. Improvement in economic opportunities through economic development improves women's access to jobs. As women acquire a large share of the jobs, parents are more likely to invest in girls education Citation69. Economic development is also likely to improve basic infrastructure such as availability of water, transportation, and electricity, which increases the time available for girls’ schooling Citation70. It improves people's attitudes toward gender equality as well. As economic development increases, the proportion of the population that considers gender inequality as undesirable also increases Citation46.
The results of this study suggest that both social development and democratic institution building are crucial to improving gender equality. Feminists Citation72 for long have argued that macrosocial structures that limit social well-being among women will empower patriarchal institutions to maintain power over women. Women's social well-being is often compromised through restraints on accessibility and availability of basic social goods and services along with women's limited participation in democratic institutions. The impact of the power differential between the two genders results in inequalities in several aspects of resources such as education and income available to women. Policies to correct gender inequalities as a necessary condition is essential for improving rights. These policies have to enable women preserve their privacy, increase their perceived choices, and also improve personal freedom with regard to reproductive processes.
The results of this study indicate a few considerations for reproductive health policy development. First, reproductive health policies should include safeguards against the violation of reproductive rights. Second, gender equality programs should be seen as essential for building sustainable reproductive rights and reproductive health policies. Gender equality approach has been recognized in the European Union as essential for facilitating a conducive environment for women's reproductive health through eradicating poverty and promoting women's employment. Finally, broad-based policies strengthening democratic institutions as well as agencies and organizations at the governmental and non-governmental levels for promoting social development are essential for achieving reproductive health through improvements in gender equality.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Notes
1To assess the reliability of this approach, we conducted a sensitivity analysis. We dropped about 10% of the cases for each variable with known values and re-estimated the values using EM algorithm. We then compared the known values with estimated values using EM algorithm. We counted all re-estimated values to be acceptable if the estimated value was less than 20% of the actual value. Using this method, in all instances of single imputation, more than 70% of the cases were accurately predicted.
2We repeated the test of the SEM model with Equatorial Guinea dropped from the study. The magnitudes of the relationships among variables in the model changed only very slightly. The level of significance of all the paths remained the same across the two models with and without Equatorial Guinea.
Related Research Data
References
- Ehrich I, Lui FT. The problem of population growth: a review of literature from Malthus to models of endogenously population and endogenous growth. J Econ Dyn Contro. 1997; 21: 205–42.
- Richey LA. From the policies to the clinics: the reproductive health paradox in post-adjustment health care. World Dev. 2004; 32: 923–40.
- Moore TW. Fertility in China 1982–1990: gender equality as a complement to wealth flows theory. Popul Res Policy Rev. 1998; 17: 197–222.
- Colon-Warren AE, Alegria-Ortega I. Shattering the illusion of development: the changing status of women and challenges for the feminist movement in Puerto Rico. Feminist Rev. 1998; 59: 101–117.
- Conway T, Norton A. Nets, ropes, ladders, and trampolines: the place of social protection within current debates on poverty reduction. Dev Policy Rev. 2002; 20: 533–40.
- Uvin P. Human rights and development. Kumarian. Bloomfield CT, 2004
- Kabeer N. Mainstreaming gender equality in poverty eradication and the millennium development goals. Commonwealth Secretariat. LondonUK, 2003
- WHO. (1999). The World health report: making a difference. Genva: World Health Organization.
- Kaufmann L. Self-in-a-vat: on John Searle's ontology of reasons for acting. Philos Soc Sci. 2005; 35: 447–79.
- Qadeer I. Unpacking the myths: inequities and maternal mortality in South Asia. Development. 2005; 48: 120–6.
- Dyches H, Rushing B. The health status of women in the world system. IntJ Health Serv. 1993; 23: 359–71.
- Dennis S, Zuckerman E. Mapping multilateral development. Banks'reproductive health and HIV/AIDS spending. WashingtonD.C.: Population Action International. 2007
- Fathalla MF. Reproductive health: a global overview. Early Hum Dev. 1992; 29: 35–42.
- Cook RJ. International human rights and women's reproductive health. Stud Family Plann. 1993; 24: 73–86.
- Cook RJ. Gender, health, and human rights. Health Hum Rights. 1995; 1: 14–25.
- Dixon-Mueller R. Population policy and women's rights: transforming reproductive choices. Praeger Publishers. Westport CT and London, 1993
- Correa S, Petchesky R. Reproductive and sexual rights: a feminist perspective. Population policies reconsidered: health, empowerment, and rights. Sen G, Germain A, Chen LCHarvard University Press. Boston MA, 1994; 107–123.
- Garcia-Moreno C, Claro A. Challenges from the women's health movement: Women's rights versus population control. Population policies reconsidered: health, empowerment, and rights. Sen G, Germain A, Chen LCHarvard University Press. Boston MA, 1994; 47–57.
- Germain A, Nowrojee S, Pyne H. Setting a new agenda: sexual and reproductive health and rights. Population policies reconsidered: health, empowerment, and rights. Sen g, Germain A, Chen LCHarvard University Press. Boston MA, 1994; 27–46.
- Yamin AE. Defining questions: situating issues of power in the formulation of a right to health under international law. Hum Rights Quart. 1996; 18: 398–438.
- Mann J. Human rights and AIDS: the future of the pandemic. The John Marshall Law Rev. 1996; 30: 195–206.
- Mann J. Medicine and public health, ethics and human rights. Hastings Cent Rep. 1997; 27: 6–13.
- Mertus J. War's offensive on women: the humanitarian challenge in Bosnia, Kosovo and Afghanistan. Kumarian Press. Bloomfield CT, 2000
- Easley Marks C, Morgan R. The challenge and place of international human rights in public health. Am J Public Health. 2001; 91: 1922–5.
- Marks SP. The new partnership of health and human rights. Hum Rights Dialog. 2001; 2: 21–22.
- Hartmann B. Reproductive rights and wrongs: the global politics of population control and contraceptive choice. Harper & Row. New York NY, 1987
- Folbre N. Who pays for the kids? Gender and the structures of constraint. Routledge. London and New York, 1994
- Kathewera-Banda M, Gomile-Chidyaonga F, Hendriks S, Kachika T, Mitole Z, White S. Sexual violence and women's vulnerability to HIV transmission in Malawi: a rights issue. Int soc sci j. 2005; 57: 64–660.
- Nair S, Sexton S, Kirbat P. A decade after Cairo: women's health in a free market economy. Ind J Gen Stud. 2006; 13: 171–93.
- Eager PW. From population control to reproductive rights: understanding normative change in global population policy (1965–1994). Global Soc. 2004; 18: 145–73.
- Clark R. Three faces of women's power and their reproductive health: a cross –national study. Int Rev Moder Sociol. 2006; 32: 35–45.
- Mohan B. Social exclusions: challenges for new social development. J Comp Soc Wel. 2007; 23: 69–79.
- Haq M. ul. Reflections of human development. Oxford: Oxford University press. 1995.
- Sen A. Democracy as a universal value. J Democr. 1999; 10: 3–17.
- Midgley J. Social development: the developmental perspective in social welfare. Sage. London and Thousand Oaks CA, 1995
- Ruger JP. Health and social justice. Lancet. 2004a; 364: 1075–1080.
- Ruger JP. Combating HIV/AIDS in developing countries. Brit J Med. 2004b; 329: 121–2.
- Ruger JP. Millennium development goals for health: building human capabilities. B World Health Organ. 2004c; 82: 951–2.
- Buvinic M. Promoting gender equality. Int Soc Sci J. 1999; 51: 567–574.
- World Bank. Gender equality and the millennium development goals. gender and development group. New York: World Bank. 2003.
- McDaniel SA. Toward a synthesis of feminist and demographic perspectives on fertility. The Sociol Quart. 1996; 37: 83–104.
- Vilas C. Between earthquakes and volcanoes: market, state, and the revolution in Central America. Monthly Review Press. New York, 1995
- Walby S. Gender, globalization and democracy. Gender dev. 2000; 8: 20–28.
- Ball W, Charles N. Feminist social movements and policy change: devolution, childcare and domestic violence policies in Wales. Women's Stud Int Forum. 2006; 29: 172–183.
- Rothschild J, Tomchin A. Can collectivist-democracy bring gender equality? The efforts at Twin Oaks. Res Sociol Work. 2006; 16: 178–198.
- Inglehart R, Norris P. Rising tide gender equality and cultural change. Cambridge University Press. Cambridge Massachusetts, 2003
- Squires J. Is mainstreaming transformative? Theorizing mainstreaming in the context of diversity and deliberation. Soc Pol: Int Stud Gen, State & Soc. 2005; 12: 366–88.
- Clark R. Contrasting perspectives on women's access to prestigious occupations: across national investigation. Soc Sci Quart. 1991; 72: 22–32.
- Clark R, Ramsbey TW, Adler E. Culture, gender, and labor force participation: a cross national study. Gender and Soc. 1991; 5: 47–66.
- Norris P, Inglehart R. Sacred and secular: religion and politics worldwide. Cambridge University Press. CambridgeUK, 2004
- Wang GZ, Pillai VK. Women's reproductive health: a gender sensitive human rights approach. Acta Sociologica. 2001; 44: 231–42.
- Dempster AP, Laird NM, Rubin DB. Maximum likelihood from incomplete data via the EM algorithm. J Roy Stat Soc, Ser B. 1977; 39: 1–39.
- Brown T. Confirmatory factor analysis for applied research. The Guilford Press. New York NY, 2006
- Nunnaly JC. Psychometric theory. McGraw Hill. New York, 1978
- Hair JF Jr, Anderson RE, Tatham RL, Black WC. Multivariate data analysis5th ed. Prentice Hall. Upper Saddle River NJ, 1998
- Hossain MK, Khan MH, Islam MN. Men's attitudes and their participation in family planning program: A micro level study in Bangladesh. Proceedings of the Pakistan Academy of Sciences. 2004; 41: 95–101.
- Bogecho D. Putting it to good use: the international covenant on civil and political rights and women's right to reproductive health. Law, Soc Justice and Glob Develop. 2004; 1: 68–98.
- New Freeland L. The status of reproductive rights and related research and the impact on dialogue. Paper presented at the Oxford Roundtable. Oxford, England2004.
- Kaddour LA, Hafez R, Zurayk H. Women's perceptions of reproductive in health three communities around Beirut. Reprod Health Matt. 2005; 13: 34–42.
- Pillai V, Gupta R. Cross-national analysis of a model of reproductive health in developing countries. Soc Sci Res. 2006; 35: 210–27.
- Sen A. Population policy: authoritarianism versus cooperation. J Popul Econ. 1997; 10: 3–22.
- Turner B. The erosion of citizenship. Brit J Soc. 2001; 52: 189–209.
- Mahajan G. Gender equality and community rights: paradoxes of liberal democracy in India. J gen stud. 1996; 169–77.
- Phillips A. Engendering democracy. Pennsylvania University Press. University Park PA, 1991
- Jensen J. Extending the boundaries of citizenship: women's movements in western Europe. The challenge of local feminisms: women's movements in global perspectives. Basu AWestview. Boulder CO, 1995; 45.
- Jaquette JS, Wolchik SL, Women and democracy: Latin America and Central and Eastern Europe. Baltimore: Johns Hopkins University Press. 1998.
- Luciak IA. Gender equality in the Salvadoran transition. Lat Am Perspect. 1999; 26: 43–67.
- Schild V. Gender equality without social justice: women's rights in the neoliberal age. NACLA Rep Americans. 2000; 34: 25–28.
- Achola PW, Pillai V. Challenges of primary education in developing countries: insights from Kenya. Ashgate publishers. Aldershot Burlington, VT, 2000
- Sunil TS. Age at marriage, contraceptive use and abortion in Yemen 1991–1997. Can Stud Popul. 2004; 31: 83–107.
- Vanhanen T. Democratization: a comparative analysis of 170 Countries. Routledge. New York, 2003
- Hoskyns C. Integrating Gender: women, law and politics in the European Union. Verso. Brooklyn, 1996
