Abstract
The study deals with infant mortality (IMR) that is one of the most important aspects of indigenous vulnerability.
Background: The Sami are one of very few indigenous peoples with an experience of a positive mortality transition.
Objective: Using unique mortality data from the period 1750–1900 Sami and the colonizers in northern Sweden are compared in order to reveal an eventual infant mortality transition.
Findings: The results show ethnic differences with the Sami having higher IMR, although the differences decrease over time. There were also geographical and cultural differences within the Sami, with significantly lower IMR among the South Sami. Generally, parity has high explanatory value, where an increased risk is noted for children born as number five or higher among siblings.
Conclusion: There is a striking trend of decreasing IMR among the Sami after 1860, which, however, was not the result of professional health care. Other indigenous peoples of the Arctic still have higher mortality rates, and IMR below 100 was achieved only after 1950 in most countries. The decrease in Sami infant mortality was certainly an important factor in their unique health transition, but the most significant change occurred after 1900.
That the health of indigenous peoples worldwide compares unfavorably with that of their non-indigenous counterparts is well established. Recent studies have found that indigenous peoples suffer higher infant and child mortality, higher maternal morbidity and mortality, heavy infectious disease burdens, and higher levels of suicide. Colonization brings many changes to the area of traditional land use, and the complexity is a challenge to research Citation1. The epidemiological transition that took place in the western world with the introduction of modern public health measures was crucial in reducing epidemic diseases and raising life expectancy, but these measures have benefited non-indigenous populations more than indigenous peoples Citation2.
The improvement in health and life expectancy among Swedish Sami represents one of the few encouraging examples of a positive indigenous health transition. Even with documented threats such as high suicide rates among young reindeer herders, the Swedish Sami of today experience standards of living, life expectancy, and health equal to those of non-indigenous Swedes Citation3. The scenario was different 150 years ago when life expectancy was considerably lower among the Sami as compared to the settler population Citation4 Citation5. However, it is still unclear how the Sami health transition came about.
Systematic longitudinal information about health, morbidity, and mortality among the world's indigenous populations is generally hard to find. Infant mortality rates (IMR) are one of the most used indicators to understand a population's health status, especially if it is possible to examine them over an extended period of time. The contemporary evidence that does exist of indigenous peoples’ IMR suggests that poor living conditions and nutrition along with high rates of infectious diseases result in an IMR much higher than among non-indigenous populations Citation1 Citation6 Citation7 Citation8 .
In an effort to increase our understanding of the demographic transition in northern Sweden, the present study aims to examine the IMR during the period of intensified colonization in a Sami and non-Sami population.
Historical background
Research indicates that many Sami became reindeer herders in the early 17th century, as a response to a population crisis Citation9. Their economy was previously based on hunting and gathering. This transition coincided with the Swedish state's increased interest in Sápmi, the distant regions of the north which were the Sami's traditional lands. Churches were built with the ambition to convert the Sami to Christianity. Courts were held annually, market places were built, and the first printed books in the Sami language appeared Citation10. Further interest in the area was stirred in the late 17th century by the discovery of silver, but the mining epoch lasted for only 50 years. The Sami remained very isolated, not only because of their economy and culture but also because of the great distances between households and the intense cold of the region for most of the year. At the end of the 17 century, the state also tried to encourage settlers to move to the area, offering free land, and 15 years free from taxes. This had, however, a limited impact on in-migration, a trend that did not change until the mid-18th century. During the following 100 years, the ethnic balance in Sápmi changed, turning the Sami into a position as minority in their own lands. Their culture and society underwent major changes as well Citation11.
Data and research methods
Omran's essay on the epidemiological transition, modeling societies change from high mortality due to infectious diseases to low mortality caused by chronic diseases, has had a great impact on the public health community and stirred research in a variety of disciplines Citation12 Citation13. Indigenous peoples were not mentioned in his work, but few researchers would dispute that the indigenous populations of the world experienced demographic transitions much later than non-indigenous populations. However, although an indigenous demographic or health transition is generally acknowledged, due to lack of longitudinal data, it is rarely examined Citation14 Citation15.
The main source material used for the present study is a set of data files from the demographic dataBase (DDB) at Umeå University, one of the world's most information-dense historical population databases. A recent addition to the DDB are 18th and 19th century parish records from Sápmi. The longitudinal database includes every individual in the parishes during the period when the area was colonized, largely by Swedish settlers, and the Sami population changed from a majority to a minority. The source material separates the Sami and the settler populations and contains information on, for instance, sex, age, cause of death, migration, and fertility. Each individual can be followed from the cradle to the grave allowing the reconstruction of life biographies and family composition based on ethnic categorization ().
Table 1. Working sample and missing cases
Because data quality is poor in the earlier years, the time period has been restricted to 1750–1895. Only infants born within the study area and with a known birth day have been included. The total working sample comprises 18,801 births in three different parishes.
Infant mortality is calculated by the number of deaths within the first year of life during a time period divided by the number of live births during the same period. When calculating infant mortality and making comparisons with Swedish national data, 10 year intervals were used Citation16.
The risk of infant mortality is modeled as a Cox proportional hazard model with ethnicity, sex, parity, birth season, and birth period as the explanatory covariates. Separate models are estimated for the three different parishes. The statistical package used was SPSS, version 19 ().
Fig. 1. Map of Sweden, including the parishes of Jukkasjärvi, Jokkmokk, and Föllinge. Source: Demographic database, Umeå University.

Sápmi, the traditional Sami area, is culturally very complex. Sami live in four countries, speak nine different languages, and are diversified by reindeer-herding techniques, social organization, and economic resources. Until the early 19th century, Sami land rights were legally protected, but then a more repressive state policy replaced the Sami traditional division and use of land with a national administrative system Citation17.
The present study includes three parishes where Sami were in a great majority around 1750. The church registers of Jukkasjärvi and Jokkmokk in the North Sami area contained both Sami and Swedish settlers, whereas Föllinge Sami parish in the South Sami area was an administrative construction exclusively for the indigenous population in the area. There was also a corresponding parish register for the settlers of Föllinge. The magnitude and timing of colonization differed between the parishes. In the northernmost parish of Jukkasjärvi, Sami were in majority throughout the period 1750–1900. Until 1850, there are around 400 non-Sami and 1000 Sami, and both groups experienced a population increase from 1880, settlers more than the indigenous. We believe that the parish of Jokkmokk is more representative of the Sami parishes in general, where an ethnic majority shift occurred around 1830, moving in a frontier wave from the south to the north. In the parish of Föllinge, the ethnic majority shift came earlier: from the late 18th century, there were more non-Sami than Sami in the area, and the change accelerated so that at the end of the period there were almost 10 times as many Swedes as Sami. Conflicts between reindeer herders and settlers were intensive in the area.
Previous research has to a large extent exclusively counted the reindeer herding nomads in the Sami group. There was, however, an ethnic complexity in the north already during the early stages of colonization, and not all Sami were nomadic reindeer herders; large groups were hunters or farmers, and during the period, many Sami took up residence in settlements, becoming settlers but still Sami, sometimes recorded as ‘Sami-settlers’ [lappnybyggare] in the parish registers. All these groups are included as Sami in our study, resulting in a Sami population larger than normally stated. This has been done to create a more ‘in situ’-oriented demography Citation18. We have combined the ethnic markers in the sources using a system designed by the historian Gabriella Nordin in her dissertation on marriage patterns in Sápmi 1750–1900 and also presented in Sköld and Axelsson Citation5 Citation11.
A complementary source of information about infant mortality is the annual reports of the district physicians in the area. However, the doctors were not well acquainted with the conditions among the Sami, and the reports often give laconic and judgemental descriptions of Sami health.
Previous studies of Sami mortality have revealed considerably higher rates from 1750 to1900 compared with non-Sami, both in Sápmi and in Sweden generally Citation4 Citation5 Citation19. By contrast, the second half of the 20th century shows no ethnic mortality differences Citation3. This is consistent with the occurrence of a delayed indigenous demographic and epidemiologic transition Citation20, and because infant mortality is one of the early indicators of intensified change, our study aims to find evidence for declining IMR among the Sami before 1900 that could be interpreted as a forerunner of a general transition. Long-term infant mortality trends are analyzed to compare Sami and non-Sami groups in the three parishes.Using both northern and southern Sami areas, the cultural complexity of the Sami society is recognized. Infant mortality generally has shown great geographic variations Citation21. Sex differences and seasonality are included parameters that are interpreted in terms of the varying work intensity of the reindeer nomads. Parity, causes of death, and change over time are additional variables that complete the study together with an estimation of the impact of health care programs. The results are discussed from the perspective of data quality, methodological issues, and the general demographic transition in Sweden.
Northern cultures
The Sami have lived in Sápmi for thousands of years and have learned to adapt to the extreme conditions there. Nevertheless, the nomadic Sami lifestyle, the hazardous character of reindeer herding, and a shifting food resource resulted in a high mortality, including infant mortality. The Sami were devoted parents with strong emotions and traditions attached to their children, and had developed customs for reducing risk during pregnancy, delivery, and child care. Traditionally, pregnant women were recommended to stay mobile but not to work hard. Birth was given in a standing or knee heeling position. Men were considered excellent midwives because of their experience with reindeer. The child was believed to be endangered by evil spirits and other threats, and a newborn child was put in a skin from a newborn reindeer calf, with a piece of steel close to the infant to protect it Citation22.
Breast-feeding was the only option for Sami mothers. It is universally reported by the clergy, physicians, travelers, politicians – and later also expressed by the Sami themselves – that Sami children were breast-fed for at least 2 years, and sometimes for as long as four years. During the first days after birth, before the mother produced milk, the infant was given a piece of sugar or reindeer fat in a small napkin. This might have caused a risk of infections, especially during summer. Some Sami women consumed alcohol during pregnancy but not during the last days before birth giving. However, when the infant was born, the woman was encouraged to drink quite a lot of alcohol Citation22.
The non-Sami settlers were mostly from other parts of Sweden, but sometimes from Finland or Norway. Colonization was promoted by the state from the late 17th century, but the great explosion of in-migration occurred in the second half of the 19th century, when mining, railroads, and improved agricultural techniques offered new opportunities.
The medical health care organization
From the mid-18th century, the Swedish health care system tried to reduce the very high infant mortality in the country. In Stockholm and other urban areas, sometimes more than half of the newborn children died within their first year of life. Medical instructions were published concerning the care of infants, and district doctors were employed, even though in the 1870s it was still a rare event for someone in northern Sweden to have a visit by the doctor Citation23.
In earlier times, the clergy were given responsibility for health care, but during the 19th century they became less and less involved. They were officially released from health duties in 1830, and after this, their participation in medical issues in the parish was greatly reduced, although many clergy continued to assist with medical advice. From this time, midwifery services increased, although economic difficulties caused many parishes to resist official requests to employ a midwife Citation24.
Infant mortality in Sápmi
In the early 19th century, the northern parishes had among the highest infant mortality in Sweden. The region around Stockholm also suffered from extremely high death rates for the youngest. The IMR declined over the 19th century, as a result of improved hygiene, and increased breast-feeding. In many places in Sweden, it had not been common to breast-feed babies. Instead, there was a widespread culture of artificial feeding, where undiluted and unboiled cow milk, often sour and of bad quality, replaced breast-feeding. Different sorts of diarrhea were common in those areas, especially during the warm summer months. The combination of hard agricultural work that often prevented mothers from breast-feeding their infants, and the difficulties in preserving fresh milk, resulted in repeated mortality peaks from June to August. Previous research has shown that high levels of artificial feeding of infants lead to higher mortality during the summer months. Nevertheless, many areas in northern Sweden experienced a great reduction in infant mortality during the 19th century. In some parishes, it dropped from over 50% to below 18% 50 years later Citation23.
Swedish observers in the 18th century believed that Lapland, as Sápmi was then known, was one of the healthiest places someone could live. It was thought that the fresh air guaranteed a long and strong life. Although some clergy were afraid that the nomadic life that began soon after the birth was harmful, as were the drinking habits of the women, the Sami were generally described as healthy: children were given frequent baths and infants were breast-fed for several years Citation25. It was not until Hellstenius in 1884 published an article on infant mortality in the counties of Jämtland and Härjedalen, including the South Sami area, that the extremely high infant mortality among the Sami was revealed. However, Hellstenius offered no explanation other than vague ideas about racial differences. Later, Wahlund showed a similar infant mortality among Sami parishes in the northern area, twice as high as the settlers. Children and adults showed no corresponding increased mortality Citation26 Citation27 ().
Fig. 2. Sami infant mortality in Jukkasjärvi, Jokkmokk, Föllinge, and Sweden in 1751–1895.
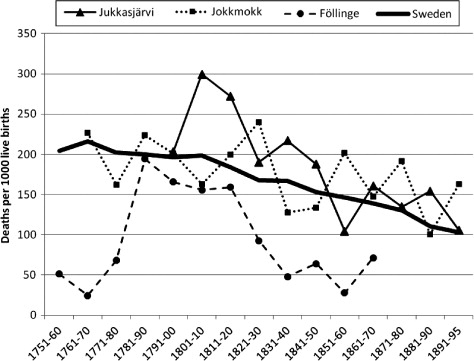
Registration before 1780 is often incomplete and the IMR is unreliable. At the end of the 18th century, Sami infant mortality was at the same high level as the rest of Sweden, and occasionally even higher, but when the IMR declined generally in Sweden from 1810, the Sami in Jukkasjärvi and Jokkmokk stayed at high rates. The Sami parish of Föllinge shows considerably lower rates than the Sami in the other two parishes, and until 1850 Sami infants in Föllinge had much lower mortality than in the rest of Sweden. The trend appears to continue with only six infant deaths of 93 births during the period 1850–1895. Due to the low overall number of births and deaths, we have excluded 10 year averages for Föllinge parish ().
Table 2. Infant mortality (per 1000) in Jukkasjärvi, Jokkmokk, and Föllinge in 1750–1899
There is a general trend of decreasing Sami infant mortality in 1750–1899. In the northern parish of Jukkasjärvi, Sami have consistently higher IMR than the rest of Sweden, but the difference decreases over time. Until 1850, they also have higher rates than the non-Sami in the parish, but during the second half of the century, the situation is the opposite. The non-Sami in Jukkasjärvi experience increased infant mortality over time. Before 1850, their IMR is lower than in Sweden, thereafter higher. The non-Sami in Jokkmokk also have lower IMR than Sweden until the mid-19th century. They have an increasing IMR trend over time, nevertheless their rates are lower than the Sami throughout the period. In Föllinge, there are insignificant IMR differences between Sami and non-Sami, and both groups are well below the Swedish average. There is an excess infant mortality for males in all three parishes, and for both Sami and non-Sami (except for non-Sami in Föllinge). The sex difference was greater among the Sami ().
Table 3. Male and female infant mortality (per 1000) in Jukkasjärvi, Jokkmokk, and Föllinge 1750–1899
The higher male IMR is significant for both Sami and non-Sami in Jukkasjärvi and in Jokkmokk, but in Föllinge only for Sami. There is, however, no reason to believe that these differences have any explanatory value for the demographic transition in Sápmi.
Parity: the impact of birth order
It was often claimed that Sami families were smaller than non-Sami families in the area Citation28. This was often based on an assumption that a large family was an obstacle to the nomadic life of the reindeer herders ().
Table 4. Infant mortality (per 1000) after parity in Jukkasjärvi, Jokkmokk, and Föllinge 1750–1899
In all three parishes, Sami infants born as child number five or more suffered from the highest risk of dying. Although we cannot control for the number of older siblings that were actually alive, it seems clear that large families were less able to avoid infant mortality. The mothers who gave birth for the fifth time or more were also older than those giving birth for the first time. The health status of the mother is an important determinant of infant survival, especially during the first week. Among the Sami, first-born infants had the second largest risk of dying, whereas among the non-Sami they experienced the greatest risk. The settlers may have lacked the well-developed traditional knowledge needed for dealing with the cold climate and other risks specific to the northern inland area. Both ethnic groups in all parishes had the lowest risks for mortality for infants born as number two, three, or four in the birth order of the mother.
1800–1899: a dynamic century
The period of study includes great social, political, economic, demographic, and environmental changes. Due to the unreliability of the data during the 18th century, the cox regression analysis is based on results from the period 1800–1899 ().
Table 5. Cox regression of infant mortality in Jokkmokk, Jukkasjärvi, and Föllinge, 1800–1899
The results show geographical differences between the three Sami groups. In Jokkmokk with an ethnic majority shift around the 1830s, a pronounced Sami excess infant mortality remains throughout the 19th century. This is also the only parish with the highest mortality risk among the first born infants in 1850–1899. The northern parish Jukkasjärvi experiences a dramatic shift from twice as high Sami infant mortality in1800–1849 to slightly lower IMR compared to the non-Sami during the second half of the century. The more balanced the ethnic proportions became, the less differences occurred in infant mortality. In the southern parish of Föllinge, Sami were a minority from the 18th century, but nevertheless they showed higher IMR over the entire period.
Generally, a modest male excess mortality is found and less risk for parity 2–4. There are no noteworthy seasonal differences, except in Föllinge where higher IMR appeared among infants born during the winter months January to March. The sample from this parish is too small to include separate analyses for different periods of the 19th century.
Conclusion
The Sami in the northern parishes of Jokkmokk and Jukkasjärvi had a high IMR between 1750 and 1900, whereas the southern Sami in Föllinge experienced considerably lower levels. If infant mortality is used as an indicator of a positive shift in the demographic, epidemiologic, and health transitions, it can be concluded that by 1900 these transitions had not begun in the northern parts of the area. The non-Sami in the area show increased IMR over time, and did not follow the decreasing IMR in Sweden from the 1820s. The indigenous people of northern Sweden experienced a delayed process, and at the end of the 19th century, their IMR were still above the national average. On the other hand, the trend shows decreasing IMR, and we know that the gap between the Sami and the rest of Sweden was closed around 1950.
Other indigenous peoples of the Arctic still have much higher mortality rates, and an IMR below 100 was achieved only after 1950 in most countries Citation29 Citation30. Between 1910 and 1939, the native people in Canada had an IMR between 120 and 205 Citation31. Serning reported remaining ethnic IMR differences in Jukkasjärvi and Jokkmokk for the period 1930–1948, but they were rapidly decreasing Citation22. And, from the 1960s, there are no significant mortality differences between Sami and non-Sami in the area Citation3. Therefore, the first half of the 20th century is crucial for our understanding of the IMR transition in Sápmi, and hence for our understanding of the Sami demographic, epidemiologic, and health transitions.
Brändström Citation23 asked if there were reasons to believe that the Sami practiced birth control. Contemporary observers claimed that Sami women gave birth to few children, rarely more than five or six Citation31, even if they married at early ages Citation11. By limiting family size, they may have avoided the increased risk associated with higher order births, and by concentrating births in the seasons with lower risk, they may have improved survival. Cultural responses to infectious diseases and the use of a so-called komse, a small wooden boat box where infants were kept almost constantly for 1 or even 2 years Citation32 Citation33 helped in the care of the newborn children.
The traditional nomadic life style is important for our understanding of Sami infant mortality Citation25, but there is no reason to believe that hard working conditions caused the Sami women to stop breast-feeding their infants, as was often the case in other contexts Citation34. Reindeer herding was an extreme form of living, and the social organization did not offer any assistance. Sami women either rejoined the continuous travel with the reindeer only a couple of days after giving birth Citation31 or were left alone with the child in a hut Citation22. This would certainly have increased the risk of the infants dying.
Until the mid-19th century, the Sami IMR was considerably higher than the non-Sami in the area, even though extensive breast-feeding prevented infectious diseases and nutritional deficiencies. We can note cultural differences within Sápmi, where the South Sami joined the low IMR of the district of Jämtland, whereas the northern parishes remained at higher levels. However, there is no evidence that medical interventions played any significant role in the reduction in infant mortality. The Sami rarely had any contact with the district physicians, and midwives were not appointed in the northern parishes until the late 19th century.
Demographic changes certainly occurred in Sápmi during the process of colonization. Kertzer and Fricke Citation35 take a cultural approach to demographic behavior, arguing that from an anthropological perspective, the concept of agency must be given more prominence. They emphasize a cultural sphere that is interwoven with, both shaping and being shaped by, political and economic institutions as well as by kinship and other social organizational structures.
The Sami population has slowly increased since the 18th century and onwards, and the previous general opinion that the Sami were a dying race has been proven to be mistaken. It is the Sami culture, and not the Sami race, that is under threat today Citation36. But the path to this point has been long and winding, including great improvements in life expectancy. Infant mortality was a difficult obstacle to overcome, and the final breakthrough did not occur until the 20th century.
Conflict of interest and funding
The authors have not received any funding or benefits from industry to conduct this study.
Acknowledgements
The present study has been funded by the Swedish Council for Working Life and Social Research (FAS) and the European Science Foundation: Eurocores Programme – BOREAS (Home, Hearth, and Household).
References
- Gracey M, King M. Indigenous health part 1: determinants and disease patterns. The Lancet. 2009; 374: 65–75.
- Coates KS. A global history of indigenous peoples. Struggle and survival. Houndmills, Basingstoke, Hampshire. Palgrave Macmillan. New York, 2004
- Hassler S. The health condition in the Sami population of Sweden 1961–2002. Umeå: Umeå University. 2005.
- Sköld P. Liv och död i Lappmarken. Aspekter på den demografiska utvecklingen i Arjeplog under 1700- och 1800- talen [Life and death in Sápmi. Aspects on the demographic development in Arjeplog during the 17th and 18th centuries]. Befolkning och bosättning i norr. Etnicitet, identitet och gränser i historiens sken [Population and settlement in the north. Ethnicity, identity and borders in the light of history]. Lantto P, Sköld PUmeå University. Umeå, 2004; 85–105.
- Sköld P, Axelsson P. The Northern population development. Colonization and mortality in Swedish Sápmi 1786–1895. Int J Circumpol Health. 2008; 67: 29–44.
- King M, Smith A, Gracey M. Indigenous health part 2: the underlying causes of the health gap. The Lancet. 2009; 374: 76–85.
- Heaton TB, England J, Lynne B, Myrna G, López GL. The child mortality disadvantage among indigenous people in Mexico. Population Review. 2007; 46: 1–11.
- Stephens C, Porter J, Nettleton C, Willis R. Disappearing, displaced, and undervalued: a call to action for indigenous health worldwide. The Lancet. 2006; 367: 2019–28.
- Sköld P. Samisk bosättning i Gällivare 1550–1750 [Sami settlement in Gällivare 1550–1750]. Umeå: Umeå University. 1992.
- Rydving H. The end of drum-time. Religious change among the Lule Saami, 1670s–1740s. Uppsala University. Uppsala, 1993
- Nordin G. Äktenskap i Sápmi. Giftermålsmönster och etnisk komplexitet I kolonisationens tidevarv, 1722–1895 [Sápmi marriages. Marriage patterns and ethnic complexity during the era of colonization, 1772–1895]. Umeå: Umeå University. 2009.
- Omran AR. The epidemiologic transition. A theory of the epidemiology of population change. Millbank Mem Fund Quart. 1971; 49: 509–38.
- Caldwell JC. Population health in transition. Bulletin of the World Health Organization. 2001; 79: 159–60.
- Kunitz S. Disease and social diversity. European impact on the health of non-Europeans. Oxford University Press. New York and Oxford, 1994
- Waldram JB, Herring A, Young TK. Aboriginal health in Canada: historical, cultural and epidemiological perspectives2nd ed. Toronto University Press. Toronto, 2006
- Befolkningsutvecklingen under 250 år. Historisk statistik för Sverige. Demografiska rapporter 1999:2 [The population development during 250 years. Historical statistics of Sweden. Demographic reports 1999:2]. Stockholm: Statistiska Centralbyrån. Stockholm: Statistics Sweden; 1999
- Brännlund I, Axelsson P. Reindeer management during the colonization of Sami lands: a long-term perspective of vulnerability and adaptation strategies. Glob Environ Change. 2011; 21: 1095–105.
- Taylor J. Indigenous demography and public policy in Australia: population or peoples?. J Popul Res. 2009; 26: 115–30.
- Edvinsson S, Gardarsdottir O, Thorvaldsen G. Infant mortality in the Nordic countries, 1780–1930. Continu Change. 2008; 23: 457–85.
- Trovato F. Aboriginal mortality in Canada, the United States and New Zealand. J Biosoc Sci. 2001; 33: 67–86.
- Brändström A, Edvinsson S, Rogers J. Infant mortality in Sweden. Creating regions from nineteenth-century parish data. Hist Meth. 2000; 33: 105–13.
- Serning I. Lappbarnen, deras vård och uppfostran i spädbarnsåldern och lekåldern. Norrbotten. Norrbottens Läns Hembygdsförenings Årsbok 1949. Luleå Boktryckeri. Luleå, 1950; 55–109.
- Brändström A. Från förebild till motbild. Spädbarnsvård och spädbarnsdödlighet i Jokkmokk [From ideal to contrast. Infant care and infant mortality in Jokkmokk]. In: Åkerman S, Lundholm, K. Älvdal i norr. Människor och resurser i Luledalen 1300–1800 [River valley in the north. People and resources in the Lule valley 1300–1800]. Stockholm: Almqvist & Wiksell International.: 2001, pp. 307–51.
- Sköld P. Kunskap och kontroll – Den svenska befolkningsstatistikens historia. Almqvist & Wiksell International. Umeå, 2001
- Johan Ellmin. 1851. Annual report. District physician of Jämtland. Stockholm: National Archives.
- Hellstenius J. Barnadödligheten i Vesternorrlands och Jemtlands län. Statistisk Tidskrift1884: 153–68.
- Wahlund S. Demographic studies in the nomadic and the settled Population of Northern Lapland. Almqvist & Wiksell. Uppsala, 1932
- von Düben G. Om Lappland och lapparne, företrädesvis de svenske. Stockholm. Nordstedts, 1873
- Bogoyavlenskiy D, Siggner A. Arctic demography. Stefeansson Arctic Institute. Arctic Hum Dev Rep Akureiry, 2004; 27–41.
- Bjerregaard P, Young TK, Dewally E. Ebbesson SOE. Indigenous health in the Arctic: an overview of the circumpolar Inuit population. Scand J Publ Health. 2004; 32: 390–96.
- Grape E. Fortsättning af Utkast til Beskrifning öfver Enontekis Sokn i Torneå Lappmark. Kongl [Continuation of Draft of a description of Enontekis parish in Torneå Lapp District. Royal Academy of Science New Proceedings 1804]. Vetenskaps Academiens Nya Handlingar. 1804; 25: 1–44.
- Wargentin P. Anmärkningar Om nyttan af årliga Förtekningar på födda och döda i et land. Sjette stycket. Kongl. Vetenskaps Academiens Handlingar för år 1755 [Notes on the use of annual registers over births and deaths in a country. Sixth paragraph. Royal Academy of Sciens Proceedings for the year 1755]. Stockholm: Lars Salvius.: 1755; XVI: 241–53.
- Arnell C. Om förekommande af späda barns förquäfwande. Hushållnings Journal för1778: 3–8.
- Brändström A. The impact of female labour conditions on infant mortality: a case study of the parishes of Nedertorneå and Jokkmokk, 1800–96. Soc Hist Med. 1988; 1: 329–58.
- Kertzer DI, Fricke T. Towards an anthropological demography. Anthropological demography. Towards a new synthesis. Kertzer DI, Fricke TUniversity of Chicago Press. Chicago, 1997; 1–35.
- Manker E. De svenska fjällapparna. Stockholm: Svenska Turistföreningens Förlag. [The Swedish Mountain Lapps. Stockholm: Swedish Tourism Association Publishers]; 1947.