Abstract
Background : Leprosy-related disability is a challenge to public health, and social and rehabilitation services in endemic countries. Disability is more than a mere physical dysfunction, and includes activity limitations, stigma, discrimination, and social participation restrictions. We assessed the extent of disability and its determinants among persons with leprosy-related disabilities after release from multi drug treatment.
Methods : We conducted a survey on disability among persons affected by leprosy in Indonesia, using a Rapid Disability Appraisal toolkit based on the International Classification of Functioning, Disability and Health. The toolkit included the Screening of Activity Limitation and Safety Awareness (SALSA) scale, Participation Scale, Jacoby Stigma Scale (anticipated stigma), Explanatory Model Interview Catalogue (EMIC) stigma scale and Discrimination assessment. Community members were interviewed using a community version of the stigma scale. Multivariate linear regression was done to identify factors associated with social participation.
Results : Overall 1,358 persons with leprosy-related disability (PLD) and 931 community members were included. Seventy-seven percent of PLD had physical impairments. Impairment status deteriorated significantly after release from treatment (from 59% to 77%). Around 60% of people reported activity limitations and participation restrictions and 36% anticipated stigma. As for participation restrictions and stigma, shame, problems related to marriage and difficulties in employment were the most frequently reported problems. Major determinants of participation were severity of impairment and level of education, activity and stigma. Reported severity of community stigma correlated with severity of participation restrictions in the same districts.
Discussion : The majority of respondents reported problems in all components of disability. The reported physical impairment after release from treatment justifies ongoing monitoring to facilitate early prevention. Stigma was a major determinant of social participation, and therefore disability. Stigma reduction activities and socio-economic rehabilitation are urgently needed in addition to strategies to reduce the development of further physical impairment after release from treatment.
About 15% of the world's population has some form of disability Citation1. Disability is a difficulty in functioning at the body, person, or societal levels, in one or more life domains, as experienced by an individual with a health condition in interaction with contextual factors Citation2. Several dimensions of disability are recognized in the International Classification of Functioning, Disability and Health (ICF): body structure and function (and impairment thereof), activity (and activity restrictions) and participation (and participation restrictions) Citation3. The classification also recognizes the role of physical and social environmental factors in affecting disability outcomes. The ICF shifts the focus from the cause of disability to its effect, thereby emphasizing the role of the environment (physical, cultural, social, political) rather than focusing on disability as a ‘medical’ or ‘biological’ dysfunction Citation3 (Appendix 1).
Leprosy is an important cause of preventable disability Citation4. Physical impairment associated with leprosy is usually secondary to nerve damage resulting from the chronic granulomatous inflammation due to Mycobacterium leprae Citation5. Impairments may give rise to disabilities, such as limitations of activities involving the use of hands, feet and eyes, and restrictions in social participation. The World Health Organization (WHO) classifies leprosy-related impairment into three grades: Grade 0 – no impairment, Grade 1 – loss of sensation in the hand or foot, and Grade 2 – visible impairment Citation6. Multi-drug treatment (MDT) can cure leprosy, and, if instituted early, can prevent disability. However, leprosy is still often diagnosed too late, when permanent impairment has already occurred. Even after completion of treatment, a significant proportion of patients sustain disability from nerve damage, requiring continued (self-) care to limit further secondary damage Citation5.
Future projections of the global leprosy burden show that 5 million new cases would arise between 2000 and 2020, and that in 2020 there would be an estimated 1 million people with WHO grade 2 disability Citation7. There is very little data on the types of problems faced by people with leprosy-related disabilities (PLD) and the resulting needs they have for services Citation5. The current ‘Enhanced global strategy to further reduce the disease burden due to leprosy’ of WHO describes the necessary elements of prevention of disabilities and rehabilitation of persons affected by leprosy. Though much progress has been made in reducing the number of leprosy patients registered for MDT globally, relatively little is known about disability after release from treatment. Therefore there is an urgent need for data on leprosy-related disability to assess the need for prevention of disabilities (POD) and rehabilitation services. Such data are also needed for programme monitoring, evaluation and for advocacy Citation8.
In addition to physical impairments and activity restrictions, PLD are likely to suffer from social stigma and discrimination leading to economic loss Citation9. According to the ICF, social stigma and discrimination is considered an important ‘environmental factor’ that contributes to disability Citation3 Citation10 Citation11. Stigma is not a single phenomenon, but consists of several possible components, e.g. it may be conceptualized in terms of self-stigma (e.g. shame and lowered self-esteem) or public stigma (e.g. the general public's prejudice) that is also associated with social participation restrictions and discrimination Citation12 Citation13. The different aspects of health-related stigma can be measured using questionnaires, qualitative methods, indicators and scales Citation10. Similarly, suitable ICF-based instruments now exist to assess different aspects of disability and the factors contributing to these Citation5.
Indonesia ranks third in the number of new leprosy cases after India and Brazil Citation14. We conducted a cross-sectional baseline survey in five leprosy-endemic districts in Indonesia. Our aim was to assess the extent of disability and its determinants among persons with leprosy-related disabilities after release from MDT. In particular, we examined the incidence of worsening of physical impairment after release from treatment, the impairment in carrying out daily activities (activity restrictions), social participation, stigma (anticipated) and discrimination, all within the conceptual framework of the ICF.
Methods
Design and sampling
We conducted a cross-sectional house-to-house survey amongst persons affected by leprosy in five districts in Indonesia: Subang (West Java), Gresik, Malang (East Java), Bone and Gowa (South Sulawesi). Eligible were persons with any leprosy-related impairments, activity limitations or participation restrictions who had been released from MDT up to 5 years earlier. We obtained lists from the district cohort registers of all people affected by leprosy who had completed and been released from treatment in the past 5 years. Local health workers tried to contact as many of these as they could trace. The persons contacted were asked for consent to be screened for disability by leprosy-specialised health workers using a short eight-question questionnaire (see Appendix 2). Anyone answering ‘yes’ on any of the question was eligible for inclusion and was invited to participate in the study; all others were excluded. Furthermore, participants were excluded if they had mental impairment, severe hearing or speaking problems or were aged less than 10 years. Community members were selected through convenience sampling in the communities where persons affected by leprosy were contacted.
One hundred and twenty-six local leprosy workers conducted a house-to-house survey between December 2008 and January 2009. All interviewers received extensive and repeated training in conducting the interviews and the use of the survey instruments. Closed questionnaires were administered as face-to-face interviews for all subjects who consented to participate in the survey. We obtained basic demographic data including age, gender, marital status, employment status, WHO disability grading, and extent of physical impairment. Disability grading was done according to the WHO Operational Guidelines for the Enhanced Global Strategy 2011–2015 Citation15 and consistently applied throughout the study. Where available we obtained the disability grades at diagnosis and RFT for all subjects enrolled in the survey from the cohort register. In this way longitudinal data on physical impairment were obtained for most subjects.
The rapid disability assessment (RDA) toolkit used comprised generic methods and instruments for assessing disability and stigma, compatible with the ICF conceptual framework: Screening of Activity Limitation and Safety Awareness (SALSA) scale, Participation Scale, Jacoby Stigma Scale, Explanatory Model Interview Catalogue (EMIC) stigma scale and Discrimination assessment form Citation8 Citation10 Citation16–Citation23. Except for the discrimination questionnaire, all other instruments in the RDA toolkit were either developed in or have been culturally validated in several Asian countries in a similar target population. SALSA is a 20-item questionnaire that can be administered within 10 min and provides a standardized measure of limitations in daily activities related to mobility, dexterity, self-care and work Citation24. The Participation Scale is an 18-item instrument to measure how respondents rate their participation in comparison with a ‘peer’, defined as ‘someone similar to the respondent in all aspects except for the disease or disability’ Citation16. To measure anticipated stigma (felt stigma) we used the three-item Jacoby Stigma Scale, which measures the extent to which affected persons perceive negative attitudes or behaviour of others as a result of their condition Citation25. The Explanatory Model Interview Catalogue (EMIC) has been developed to elicit illness-related perceptions, beliefs, and practices Citation26. Part of the EMIC is a stigma scale assessing community-perceived stigma and discrimination related to a particular condition Citation19. We used a 15-item version adapted from the original EMIC scale to assess perceived stigma related to leprosy among the 931 community members included in the survey. For recording discrimination experiences, we used an adapted version of the leprosy disability study form drafted by WHO-SEARO, which assesses social discrimination experienced by people affected by leprosy (see Appendix 3). All of the questionnaires were administered in the Indonesian language.
Oral consent was obtained from all adults and from guardians of children. As this was operational research carried out within the context of the routine leprosy programme, the Leprosy Control Sub-Directorate of the Ministry of Health did not consider it necessary to obtain separate ethical approval.
Statistical analysis
Although 1,358 subjects were enrolled, not all were able to complete all assessments at the time of the survey. In addition, previous WHO disability grades were missing for a number of subjects, particularly at RFT. For this reason, we conducted one analysis on a cohort for whom data was available on all 3 assessment occasions. Parametric statistical tests were used for ordinal variables. Differences between percentages were tested using a z-test for percentages. Non-parametric analysis of variance was done using a Kruskal-Wallis test. Because the participation score was not normally distributed, multivariate quantile regression was used to examine to joint effect of a range of factors on the 75th quantile of the participation score. The coefficients indicate by how much the value of 75th quantile would be raised (or lowered) for each unit change in the explanatory variable. A higher value of the participation score indicated more severe restrictions. All analyses were done with STATA version 12.
Results
Of the 3,596 persons listed in the district cohort registers, local health workers were able to contact 2,450 persons (987 persons were unavailable due to migration, death or untraceable address). Of these, 1,092 were excluded because they did not have disability according to the screening form, were aged less than 10, or had more severe mental impairment or hearing or speaking problems; 1,358 persons were included in the survey (). The demographic characteristics of our study sample are presented in ; 843 were male (63%); the mean age was 42.5 years (range 2–90). The mean age for men was 40.6 (range 2–89) and for women it was 45.5 (range 2–90). The proportion of persons who were separated, divorced or widowed was higher among women (22.5%) than among men (8.3%; p<0.001). The illiteracy rate was 31.9%. Men had better education than women, in terms of completion of primary school, high school or advanced high school (75.9% versus 54.8%, p<0.001). The proportion of men who had salaried work was higher than of women (69.6% versus 37.2%, p<0.001). Unpaid work, including household work, was much more common among women than among men (43.9% versus 14.6%; p<0.001).
Fig. 1. Selection procedure of survey participants.
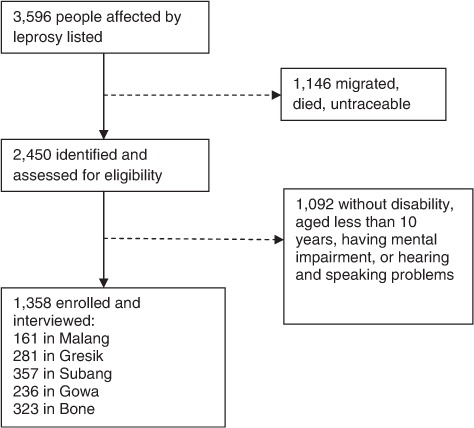
Table 1. Demographic characteristics of people affected by leprosy with disability in five districts in Indonesia (n=1,339)
shows that 76.7% of people had physical impairment (48.7% grade 2 and 28.0% grade 1). shows that most impairment was associated with the feet (47%), followed by 31% associated with the hands and 11% associated with eyes (grade 2). shows that, before treatment with standard MDT, 31% of the people already had grade 1 impairment and 31% had grade 2 impairment. The impairment status did not change significantly during treatment. At RFT, 27% had grade 1 and 32% had grade 2 impairment. However, 2–5 years after RFT, 26% of the people had grade 1 impairment and 49% had grade 2 impairment. This difference was statistically highly significant. shows the progression of impairment grades between diagnosis and the time of the survey. Among those with grade 0 at diagnosis, 48% developed additional or worse impairments; among those with grade 1, this percentage was 32%. In total 26% of those with grade 1 or 2 at diagnosis improved.
Fig. 2. Distribution of grade 0, 1 and 2 impairments after release from treatment (RFT).
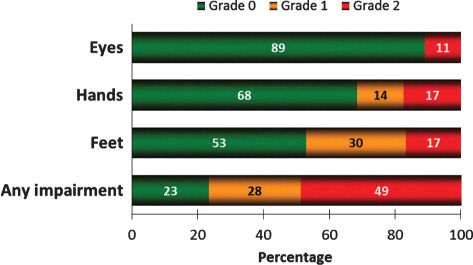
Table 2. Disability components in people with leprosy-related disability in the five-district study in Indonesia
Table 3. Development of grade 1 and grade 2 impairments at diagnosis, at release from treatment and at the time of the survey in a sub-cohort of people with leprosy-related disability who had assessment on all three occasions in the five-district study in Indonesia (n=966)
Table 4. Changes in impairment grades between diagnosis and the time of the survey in people with leprosy-related disability who had assessment on both occasions in the five-district study in Indonesia
About 60% of the people had a limitation in executing daily activities (). A similar percentage had problems participating in social life and 35.5% expressed that they experienced stigma ().
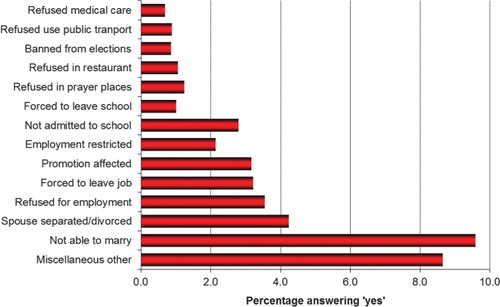
A profile of the EMIC stigma scale items () showed that the main stigma-related problems perceived by the community were shame and embarrassment, problems in finding a marriage partner and difficulties in finding salaried work. These results were consistent with the experiences of the affected persons shown in . Prominent discrimination issues were problems related to marriage, getting married and employment.
Fig. 3. Results of the Explanatory Model Interview Catalogue (EMIC) stigma scale.
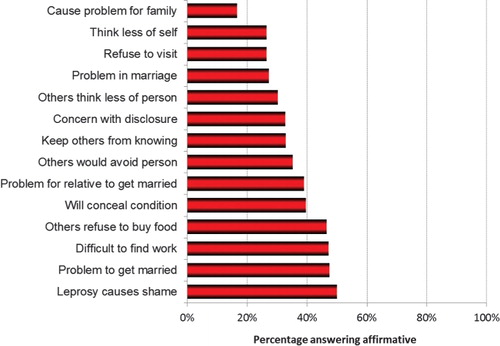
Fig. 4. Examples for discrimination from the discrimination scale.
As shown in , participation was significantly associated with age, education level, owning a motorbike, number of wounds, activity level and anticipated stigma (p<0.001), but not with gender. The 75th quantile of the participation score was six points lower for those with primary and eight points for those with higher education, compared to people without formal schooling. Severe activity limitations and/or the highest level of anticipated stigma was associated with a much higher level participation restriction (13.8 and 20.8 points, respectively).
Table 5. Factors associated with participation restriction in people with leprosy-related disability in the five-district study in Indonesia (n=1,164)
Comparison of community stigma, anticipated stigma, participation score and Salsa score by district () showed a relationship between the level of community stigma and the level of participation reported by PLD. Both were higher in Gresik, Bone and Gowa than in Malang and Subang. These differences were statistically significant (p<0.001, Kruskal Wallis test). This pattern was not seen for PLD-anticipated stigma or activity level.
Table 6. The median scores of community stigma, anticipated stigma, activity limitation and participation restriction among community members and persons with leprosy-related disabilities in the five-district study in Indonesia
Discussion
Our findings show that people affected by leprosy experience major problems in all four components of disability, body functions and structures, activities and participation, personal factors and environmental factors.
The majority of the subjects had leprosy-related physical impairments (75%). A substantial proportion (39%) of those with visible impairments at the time of the survey had developed these after release from treatment (RFT; see ). Other investigators also reported that worsening of impairments was accelerated after RFT compared to during treatment Citation27. They found a significant association between impairment at diagnosis and the risk of developing additional impairment after RFT. The most important determinant for future impairment was impairment status at diagnosis Citation27. This finding indicates a need for specific activities to prevent worsening of impairments also after RFT, especially surveillance of persons at high risk, training in foot and hand care, and provision of assistive devices.
Both felt (anticipated) stigma and community stigma were high in our study population. Perception of stigma and experiences of discrimination cause people to feel ashamed, and may cause them to isolate themselves from society, thus perpetuating the stereotype that leprosy is something shameful to be hidden away Citation28. It may cause anxiety, depression, isolation, problems in family relationships and friendships and reduce treatment adherence and chances of recovery Citation29–Citation31. As a consequence, stigma, activity and participation are usually more important to the affected person and their family than physical impairment Citation32.
The proportion of people with participation restrictions (about 60%) was much higher in this study than in studies in China (46%) Citation33 and in India (34%), but was measured in a sample who had screened positive for ‘any disability’. When using social participation as the main outcome measure, increasing levels of impairment and activity limitation increased the risk of participation restrictions significantly. Higher education and owning a motorcycle – personal factors in the ICF model – had a protective effect. The ‘motorcycle effect’ may either be explained as a proxy for wealth or social status, or work more directly through increasing mobility. Higher levels of anticipated stigma, as a proxy for stigma as environmental factor, were strongly associated with increased participation restrictions. Similar findings have been reported studies in Bangladesh, India and Brazil Citation34 Citation35. This shows that, to improve social participation, interventions may be needed at different levels. At the personal and physical level this would include measures such as improving education, income and activity, addressing physical impairments and rehabilitation; and at the societal level, reduction of stigma in the community and addressing other environmental barriers.
Multivariate analysis confirmed the strong associations between the different components of disability. The ICF emphasizes the important role of the environment and personal factors influencing body function, activities and participation and thus as determinants of disability. Especially stigma and discrimination are powerful forces in society that profoundly affect the lives of millions of people affected by stigmatized health conditions Citation36. Our study showed that stigmatising attitudes related to shame were most predominant, followed by problems to find a marriage partner, problems in marriage and problems to find work. Despite this, the majority of people interviewed did not feel stigmatised by others. Reasons for this discrepancy could be underreporting of perceived stigma or insufficient sensitivity of the Jacoby stigma scale. The high level of stigmatising attitudes in the community was confirmed by the results of qualitative data (reported elsewhere). It is possible, however, that these were not enacted and, as a result, people affected did not actually experience stigma very frequently. However, from the demographic data we observed some possible implications of disability or stigma due to leprosy. Thirty-eight percent of the people affected were unmarried, divorced, separated or widowed. This is significantly more than in a community sample with a similar age-distribution (n=101) in a recent study in Indonesia (22%; to be published elsewhere). It may be the effect of community stigma and discrimination, since problems in marriage were reported by the respondents as one of the major difficulties they faced. This has been reported elsewhere also. A study in South Africa showed that one-third of leprosy patients were abandoned by their spouses Citation37. Our study showed that women were disproportionately affected by separation and divorce then men, which can possibly be explained by the observation that women tend to be more disempowered than men when actively choosing partners and pursuing marriage. Social discrimination in marital relationships should be addressed through counselling and through advocacy in the community, with a particular focus on the needs of women.
A substantial proportion of the people with leprosy-related disability were unemployed or did unpaid work (42%). Women were disproportionally affected by unemployment, which may also be explained by the overall status of employment in a society such as Indonesia, as well as the reported lower educational status as seen in this study. The observation of high unemployment rates fits our findings regarding community stigma and the results of the Participation Scale, both of which showed that employment was one of the major problem areas. People may lose their employment because of functional disabilities associated with leprosy and or because of negative attitudes of employers or the community. This has a major impact on people's economic ability to support themselves and their families Citation38 Citation39. Being able to make a financial contribution influences a person's status in his family and in the community. In the light of these needs, socio-economic rehabilitation (SER), such as income generating projects and vocational training, should be given first priority. This will enable people affected by leprosy to find productive employment, contribute to the economy of their family and live with dignity. In a study in Nigeria, SER not only resulted in improved self-esteem, skills acquisition and financial independence, but also seemed to have initiated positive change processes in the norms and values of social interaction with people affected by leprosy Citation30.
Our study underlines that people with disability are often burdened with social stigma that promotes a cycle of poverty via unemployment, social discrimination and threats to mental health (Citation12). The findings of our survey show that stigma reduction activities and socio-economic rehabilitation are urgently needed in addition to strategies to reduce the development of further physical impairment after release from treatment.
Conclusion
This survey adds further evidence about the extent of disability that many persons affected by leprosy still have to cope with after completion of treatment. We showed that persons affected by leprosy face a substantial risk of deteriorating impairments after they are released from treatment with MDT. They often ‘disappear off the public health radar’. Women, in particular, suffer from the consequences of discrimination and stigma, as shown by higher unemployment and divorce rates. Depending on their situation, many will need appropriate support, training in self-care, monitoring of impairment status and rehabilitation. In addition to physical impairment, the stigma of leprosy has a large impact on many people's lives, affecting their physical, psychological, social and economic well-being. Stigma has multiple causes; these should be addressed in partnership with communities and persons affected. Stigma reduction activities and socio-economic rehabilitation are urgently needed in addition to strategies to reduce the development of further disabilities after release from treatment.
Conflict of interest and funding
We declare that we have no conflict of interest. The survey was supported by the Netherlands Leprosy Relief as part of their regular support to the National Leprosy Control Programme in Indonesia and by the Sasakawa Memorial Health Foundation (SMHF) through the WHO. The sponsors of this study had a role in the study conception and study design, but had no role in data collection, data analysis, data interpretation, and writing of the report.
Acknowledgements
We are grateful to the health workers who gave their best efforts in conducting the interviews for this survey and to the respondents of this survey who allowed us to take some of their valuable time. The provincial and district health services extended their generous cooperation.
Related Research Data
References
- WHO. (2011). World report on disability. Geneva: World Health Organization.
- Leonardi M, Bickenbach J, Ustun TB, Kostanjsek N, Chatterji S. The definition of disability: what is in a name?. Lancet. 2006; 368: 1219–21. 10.3402/gha.v5i0.18394.
- WHO. (2001). International classification of functioning, disability and health. Available from: http://www.who.int/classifications/icf/en/ [cited 20 April 2009].
- Britton WJ, Lockwood DN. Leprosy. Lancet. 2004; 363: 1209–19. 10.3402/gha.v5i0.18394.
- Wilder-Smith EP, Van Brakel WH. Nerve damage in leprosy and its management. Nat Clin Pract Neurol. 2008; 4: 656–63. 10.3402/gha.v5i0.18394.
- World Health Organisation (2006). Global Strategy for Further Reducing the Leprosy Burden and Sustaining Leprosy Control Activities. Operational Guidelines. http://www.who.int/lep/resources/SEAGLP20062.pdf [cited 22 July 2009].
- Richardus JH, Habbema JD. The impact of leprosy control on the transmission of M. leprae: is elimination being attained?. Lepr Rev. 2007; 78: 330–7.
- Van Brakel WH, Officer A. Approaches and tools for measuring disability in low and middle-income countries. Lepr Rev. 2008; 79: 50–64.
- Jopling WH. Leprosy stigma. Lepr Rev. 1991; 62: 1–12.
- Van Brakel WH. Measuring health-related stigma – a literature review. Psychol Health Med. 2006; 11: 307–34. 10.3402/gha.v5i0.18394.
- Stevelink SA, van Brakel WH, Augustine V. Stigma and social participation in Southern India: differences and commonalities among persons affected by leprosy and persons living with HIV/AIDS. Psychol Health Med. 2011; 16: 695–707. 10.3402/gha.v5i0.18394.
- Reeder GD, Pryor JB. Dual psychological processes underlying public stigma and the implications for reducing stigma. Mens Sana Monogr. 2008; 6: 175–86. 10.3402/gha.v5i0.18394.
- Weiss MG. Stigma and the social burden of neglected tropical diseases. PLoS Negl Trop Dis. 2008; 2: e237.10.3402/gha.v5i0.18394.
- World Health Organisation. Global leprosy situation, beginning of 2008. Wkly Epidemiol Rec. 2008; 83: 293–300.
- World Health Organisation. Enhanced global strategy for further reducing the disease. Burden due to leprosy. Operational guidelines (updated) (2011–2015). 2009. Contract No.: SEA-GLP-2009.4.
- van Brakel WH, Anderson AM, Mutatkar RK, Bakirtzief Z, Nicholls PG, Raju MS, et al.. The participation scale: measuring a key concept in public health. Disabil Rehabil. 2006; 28: 193–203. 10.3402/gha.v5i0.18394.
- van Brakel WH. Measuring leprosy stigma – a preliminary review of the leprosy literature. Int J Lepr Other Mycobact Dis. 2003; 71: 190–7.
- Withington SG, Joha S, Baird D, Brink M, Brink J. Assessing socio-economic factors in relation to stigmatization, impairment status, and selection for socio-economic rehabilitation: a 1-year cohort of new leprosy cases in north Bangladesh. Lepr Rev. 2003; 74: 120–32.
- Guidelines to reduce stigma: how to assess health-related stigma. Amsterdam/London: The International Federation of Anti-Leprosy Associations (ILEP) and the Netherlands Leprosy Relief (NLR). 2011.
- Rensen C, Bandyopadhyay S, Gopal PK, Van Brakel WH. Measuring leprosy-related stigma – a pilot study to validate a toolkit of instruments. Disabil Rehabil. 2011; 33: 711–9. 10.3402/gha.v5i0.18394.
- Kelders R, van Brakel W, Beise K, Irwanto. Testing and validating a simplified scale to measure social participation of people with disabilities in Indonesia. Disabil Rehabil. 2012; 34: 638–46. 10.3402/gha.v5i0.18394.
- Melchior H, Velema J. A comparison of the screening activity limitation and safety awareness (SALSA) scale to objective hand function assessments. Disabil Rehabil. 2011; 33: 2044–52. 10.3402/gha.v5i0.18394.
- Weiss MG, Doongaji DR, Siddhartha S, Wypij D, Pathare S, Bhatawdekar M, et al.. The explanatory model interview catalogue (EMIC). Contribution to cross-cultural research methods from a study of leprosy and mental health. Br J Psychiatry. 1992; 160: 819–30. 10.3402/gha.v5i0.18394.
- Ebenso J, Fuzikawa P, Melchior H, Wexler R, Piefer A, Min CS, et al.. The development of a short questionnaire for screening of activity limitation and safety awareness (SALSA) in clients affected by leprosy or diabetes. Disabil Rehabil. 2007; 29: 689–700. 10.3402/gha.v5i0.18394.
- Jacoby A. Felt versus enacted stigma: a concept revisited. Evidence from a study of people with epilepsy in remission. Soc Sci Med. 1994; 38: 269–74. 10.3402/gha.v5i0.18394.
- Weiss MG, Doongaji DR, Siddhartha S, Wypij D, Pathare S, Bhatawdekar M, et al.. The explanatory model interview catalogue (EMIC). Contribution to cross-cultural research methods from a study of leprosy and mental health. Br J Psychiatry. 1992; 160: 819–30. 10.3402/gha.v5i0.18394.
- Meima A, van Veen NH, Richardus JH. Future prevalence of WHO grade 2 impairment in relation to incidence trends in leprosy: an exploration. Trop Med Int Health. 2008; 13: 241–6. 10.3402/gha.v5i0.18394.
- Arole S, Premkumar R, Arole R, Maury M, Saunderson P. Social stigma: a comparative qualitative study of integrated and vertical care approaches to leprosy. Lepr Rev. 2002; 73: 186–96.
- Fung KM, Tsang HW, Corrigan PW, Lam CS, Cheung WM. Measuring self-stigma of mental illness in China and its implications for recovery. Int J Soc Psychiatry. 2007; 53: 408–18. 10.3402/gha.v5i0.18394.
- Fung KM, Tsang HW, Corrigan PW. Self-stigma of people with schizophrenia as predictor of their adherence to psychosocial treatment. Psychiatr Rehabil J. 2008; 32: 95–104. 10.3402/gha.v5i0.18394.
- Corrigan PW, Larson JE, Rusch N. Self-stigma and the ‘why try’ effect: impact on life goals and evidence-based practices. World Psychiatry. 2009; 8: 75–81.
- Van Bennekom CA, Jelles F, Lankhorst GJ. Rehabilitation activities profile: the ICIDH as a framework for a problem-oriented assessment method in rehabilitation medicine. Disabil Rehabil. 1995; 17: 169–75. 10.3402/gha.v5i0.18394.
- Chen S, Chu T, Wang Q. Qualitative assessment of social, economic and medical needs for ex-leprosy patients living in leprosy villages in Shandong Province, The People's Republic of China. Lepr Rev. 2005; 76: 335–47.
- Plagerson S. Attacking social exclusion: combining rehabilitative and preventive approaches to leprosy in Bangladesh. Dev Pract. 2005; 15: 692–70. 10.3402/gha.v5i0.18394.
- Nicholls PG, Bakirtzief Z, Van Brakel WH, Das-Pattanaya RK, Raju MS, Norman G, et al.. Risk factors for participation restriction in leprosy and development of a screening tool to identify individuals at risk. Lepr Rev. 2005; 76: 305–15.
- Weiss MG. Stigma and the social burden of neglected tropical diseases. PLoS Negl Trop Dis. 2008; 2: e237.10.3402/gha.v5i0.18394.
- Scott J. The psychosocial needs of leprosy patients. Lepr Rev. 2000; 71: 486–91.
- Gershon W, Srinivasan GR. Community-based rehabilitation: an evaluation study. Lepr Rev. 1992; 63: 51–9.
- Kopparty SN, Kurup AM, Sivaram M. Problems and coping strategies of families having patients with and without deformities. Indian J Lepr. 1995; 67: 133–52.
Appendix 1
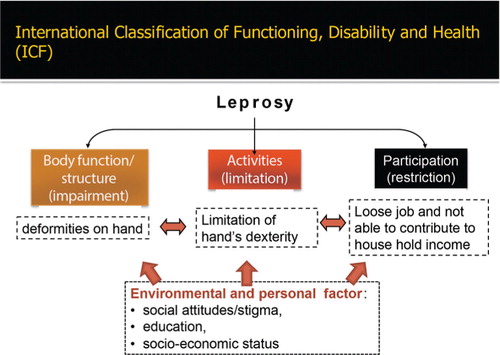
International classification of functioning, disability and health (ICF), modified from the World Health Organization (3).
Appendix 2
Screening questionnaire used in the five-district survey in Indonesia to screen for the presence of any difficulties in functioning.
Appendix 3
Discrimination questionnaire
Please answer the following questions:
1. Have you ever been at school? Yes No
a. If NO, ask: why not? Have you ever not been admitted to school or other education because being affected by leprosy? Yes No
b. If YES, ask: Have you ever been forced to leave or removed from school/other education because being affected by leprosy? Yes No
2. Have you ever been married? Yes No
a. If NO, ask: Why not? Have you ever been not able to marry because being affected by leprosy? Yes No
b. If YES, ask: Have you ever been left or separated/divorced by your spouse because being affected by leprosy? Yes No
3. Have you ever been working? Yes No
a. If No, ask:
- Why not? Have you ever been refused employment because being affected by leprosy? Yes No
- Have you ever been restricted or banned in your employment for certain areas e.g. as cook or domestic helper because being affected by leprosy? Yes No
b. If YES, ask:
- Have you ever been forced to leave or removed from a job because being affected by leprosy? Yes No
- Has your promotion ever been negatively affected because being affected by leprosy? Yes No
4. Did you ever use public transportation? Yes No
If NOT, continue with question No 5
If YES, ask: Have you ever been refused travel by public transport because being affected by leprosy? Yes No
5. Have you ever been at places of worship (temple, church, mosque or other)? Yes No
If NOT, continue with question No 6
If YES, ask: Have you ever been refused admission into a temple, church, mosque or other places of worship because being affected by leprosy? Yes No
6. Have you ever been to public places like shops or restaurants? Yes No
If NOT, continue with question No 7
If YES, ask: Have you ever been refused admission into a restaurant, hotel, shops etc because being affected by leprosy? Yes No
7. Have you ever been seeking medical care in a hospital or a health centre or at a doctor's praxis? Yes No
If NOT, continue with question No 8
If YES, ask: Have you ever been refused medical care or hospital/clinic admission because being affected by leprosy? Yes No
8. Are you old enough to vote or be voted? Yes No
If NOT, continue with question No 9
If YES, ask: Have you ever been banned from standing for elections or refused to vote because being affected by leprosy? Yes No
9. Have you ever experienced other discriminatory situations? Yes No
If YES, can you please explain?