Abstract
Background: The quality of health care depends on the competence and motivation of the health workers that provide it. In the West, several tools exist to measure worker motivation, and some have been applied to the health sector. However, none have been validated for use in sub-Saharan Africa. The complexity of such tools has also led to concerns about their application at primary care level.
Objective: To develop a common instrument to monitor any changes in maternal and neonatal health (MNH) care provider motivation resulting from the introduction of pilot interventions in rural, primary level facilities in Ghana, Burkina Faso, and Tanzania.
Design: Initially, a conceptual framework was developed. Based upon this, a literature review and preliminary qualitative research, an English-language instrument was developed and validated in an iterative process with experts from the three countries involved. The instrument was then piloted in Ghana. Reliability testing and exploratory factor analysis were used to produce a final, parsimonious version.
Results and discussion: This paper describes the actual process of developing the instrument. Consequently, the concepts and items that did not perform well psychometrically at pre-test are first presented and discussed. The final version of the instrument, which comprises 42 items for self-assessment and eight for peer-assessment, is then shown. This is followed by a presentation and discussion of the findings from first use of the instrument with MNH providers from 12 rural, primary level facilities in each of the three countries.
Conclusions: It is possible to undertake work of this nature at primary health care level, particularly if the instruments are kept as straightforward as possible and well introduced. However, their development requires very lengthy preparatory periods. The effort needed to adapt such instruments for use in different countries within the region of sub-Saharan Africa should not be underestimated.
Currently, there is a keen interest from policy makers in strategies to enhance health worker motivation, especially in low-resource contexts. The reason for this interest is closely linked with the drive to improve the quality of health care services and, ultimately, health outcomes. Many of the major theories of motivation highlighted the concept's importance for the performance and productivity of workers, mainly in industry. In the health sector, the interest in motivation is particularly strong as health care delivery is labor-intensive Citation1. Indeed, ‘the quality of health services, their efficacy, efficiency, accessibility and viability depend mainly on the performance of those who deliver them’ Citation2.
It is logical to expect that a worker's performance depends on his or her level of training or competence. Kak et al. define competence as a worker's ‘ability to perform tasks in a manner that yield desirable outcomes’ (Citation3, p. 3). Yet, the relationship between health worker competence (can do) and performance (does do) is complex and the first does not directly cause the second Citation4. Even welltrained staff do not always perform to the best of their ability Citation5 and differences are found between how health providers know a task should be performed and how they actually perform it in practice. This is the so-called ‘know–do gap’ Citation6. Motivation is believed to hold the key to overcoming this problematic gap Citation7.
Motivation is the psychological process that gives behavior purpose and direction Citation8. It cannot be directly observed Citation9, but is considered, in a work context, to be reflected in the completeness, intensity, and persistence of a worker's effort Citation10. Beyond the difficulties of studying motivation caused by its complex, transitive nature, other factors also impede the endeavor in low-resource contexts. The major theories of worker motivation originated in industrialized countries Citation11 and inherent limitations surround the transferability of these theories to developing countries Citation12. For example, the poor applicability of process theories of motivation in cultures where the linkages among actions, outcomes, and reinforcements are less likely to follow in sequence has been demonstrated Citation13.
Most theories of motivation were not specifically developed for use in the health sector Citation12. In any context, the health sector is a difficult and emotive area in which to study work motivation due to the human suffering that any lapses in performance may cause. In recent years as staffing levels have become critical in many countries, attention has also been drawn to new issues not included in traditional theories of motivation such as work stress, exhaustion, and burnout. Health care settings around the world are plagued by stressors, including ‘confrontation with severe illness and patient deaths, work overload, role ambiguity’ and low levels of support (Citation14, p. 1361). In sub-Saharan Africa, where the available workforce and resources are most limited and the burden of disease greatest Citation15, these stressors are likely to be most prevalent.
In the West, a large number of tools are available for measuring motivation. Furthermore, there are tools for assessing the professional quality of life or job satisfaction of health professionals Citation16Citation17. However, there is no tool to measure motivation that has been validated for use in developing countries Citation18Citation19. Public health studies that address motivation in such contexts have often made use of qualitative methods Citation20–Citation23. Recent anthropological literature addressing health issues in developing countries has not placed a strong focus on this area either. There are studies exploring work motivation in Africa. However the focus is largely confined to labor markets Citation24, and worker productivity in industry Citation25Citation26 or agriculture Citation27.
It has further been highlighted how seeking to apply instruments developed in one culture can lead to missing important motivational components of ‘the other culture’ (Citation25, p. 32). This risk may be considered especially pronounced given the rich cultural, ethnic, and linguistic diversity that distinguish sub-Saharan Africa Citation28.
Nonetheless, a small body of literature measuring the motivation of health workers in developing countries has emerged. Building on the research of Kanfer, a conceptual framework has been proposed for exploring the effects of health sector reform upon health worker motivation in developing countries Citation29, which has been broadly adopted Citation15Citation18Citation19. Tools were elaborated to measure motivation in the context of this framework. However, implementation largely took place at hospital level in transition countries (Jordan and Georgia). The authors observed that lower cadres had difficulty with some of the more abstract questions. With this they caution that the complexity of such tools may present an inherent barrier for their use in settings where health staff have lower levels of education Citation30.
With reference to the above, a tool was developed to establish reasons for, and explore the consequences of, the turnover of professional nurses working at public hospitals and health centers in the context of HIV/AIDS in South Africa Citation31. Further important work was undertaken in Kenya to develop a short, practical tool to measure hospital-level providers motivation, with a view to establishing what effect motivation itself may have on the introduction of interventions Citation19. Others explored, and sought to measure, the motivation of mid-level providers (sub-cadres of physicians) in Tanzania Citation18. Meanwhile, the Healthcare Provider Work Index, which incorporates many aspects of relevance to motivation, was applied to mid-level providers working at public and faith-based hospitals and health centers in Malawi Citation32. The later studies saw a shift in the emphasis from the main professional groups (physicians, nurses) to mid-level providers Citation18. However, to date there has been little exclusive focus on exploring the motivation of staff (including lower-level cadres) at primary health care level.
Present investigation
The aim of the present investigation was to develop an instrument to monitor any changes in maternal and neonatal health (MNH) care provider motivation resulting from the introduction of pilot interventions in rural, primary level facilities in Ghana, Burkina Faso, and Tanzania. The work was undertaken in the frame of the ‘Quality of Maternal and Prenatal Care: Bridging the Know–do Gap (QUALMAT) Project’. The interventions that QUALMAT will pilot are a clinical decision support system (CDSS) to reinforce provider competence, and a package of incentives to reward good performance. As the interventions are the same for all three countries it was agreed that a common instrument would be used to assess their effect on provider motivation so as to facilitate comparability. In contrast to other work in this area, this paper focuses upon the actual development of the instrument and the challenges that presented themselves. Whilst this instrument is rather specific for QUALMAT, the detailed methodology outlined here provides guidance for others seeking to put such tools into practice.
Conceptual framework
The QUALMAT conceptual framework () Citation3Citation18Citation20Citation29–Citation31Citation33 shows how individual and contextual influences interact with a provider's competence and work motivation to give rise to their work effort, ultimately resulting in their overall job performance. Its elaboration was based upon a literature review and exchange between the project collaborators. In particular, reference was made to the multi-level approach proposed by Franco et al. Citation29. It was further complemented by preliminary qualitative work carried out in all three countries.
Fig. 1. QUALMAT conceptual framework of MNH provider motivation and performance. Developed with reference to Citation3Citation18Citation20Citation29–Citation31Citation33.
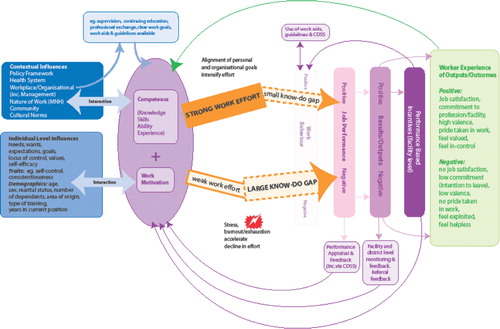
Bennett et al. attach a great deal of importance to individual level influences Citation30. In line with this, the framework outlines demographics such as age, sex, marital status, number of dependents, and level of training. It also outlines a health worker's needs, wants, expectations, goals, values, and how far they believe in their ability to succeed in certain situations (self-efficacy) Citation34. Efficacious individuals have been found to be more persistent in trying to accomplish goals Citation35. Furthermore, mention is made of traits such as self-control and conscientiousness that predispose a person to behave or respond in a certain way and which can also influence job performance (Citation3, p. 3).
The contextual influences include workplace factors (organizational level), factors resulting from the broader health system and policy environment, including conditions of employment, as well as community and cultural level influences. It has also been suggested that the nature of a job itself has implications for its motivating potential Citation36, which explains the further inclusion of work factors, that is, the variety of skills required, or the discretion a worker has to decide how to accomplish tasks. The preliminary qualitative research indicated that the actual nature of MNH work is of relevance in that it is an area that either involves routine monitoring, or rapid action and decision-making, if problems arise. Moreover, it is perceived to be an area of high occupational risk and to readily expose a provider's actual level of competence Citation37.
The workplace or organizational level factors are expanded upon in the framework, as our qualitative findings indicated difficulties in this area. Particular attention is paid to management aspects, especially human resources management, given their importance for staff performance Citation38. These aspects include whether a health worker has clear work goals, access to professional exchange, work aids and guidelines, continuing education, and supportive supervision. The other factors are not fully elaborated on in the framework. In short, health system factors are considered to include facility staffing levels and skills mix, availability of work equipment and drugs, state of infrastructure, functionality of the referral system, and so on. Policy aspects refer to employment conditions, including salaries, overtime, leave, and pension provision. Many of these were shown to be sources of serious concern in the qualitative research with many providers only moving on to talk about other aspects of their work and motivation once they had aired their grievances on these issues. At primary level care in all three countries, mid-level cadres and auxiliaries make up a significant proportion of the workforce. Several studies have highlighted that the position of these cadres is difficult in terms of the respect they command Citation18, their conditions of employment, and their opportunities for professional development Citation39Citation40. Broader conditions such as the effectiveness of legal systems may also have relevance in so far as they may deter the more extreme forms of adverse worker behavior (theft and corruption), as well as national ownership of reform processes Citation41.
Community issues include the number of patients, their level of education Citation42 and neediness Citation43, as well as their preferences and whether they are considered to resist or accept treatment Citation44. Finally, cultural factors include a tendency for workers in less secure settings to focus on immediate rather than long-term goals Citation13, loyalty to ones kin, responsibility to one's extended family, and the socioeconomic expectations made of those in certain positions Citation45. The qualitative findings show that the challenges of facility management go hand in hand with some of these issues, such as difficulties associated with maintaining discipline and criticizing older workers Citation37.
The framework ascribes a central place to work motivation, which in public health literature is defined as ‘an individual's degree of willingness to exert and maintain an effort towards organisational goals’ (Citation29, p. 1255). It shows that the extent of alignment between a health worker's personal goals and those of their workplace has an effect on an individual's willingness to exert an effort at work Citation1. Several items were incorporated in the instruments that build upon this definition. This was influenced by the qualitative work, which revealed primary health care workers were very clear about the goal of their facilities, by the ‘Work Group Climate Assessment Tool’ Citation46, and drew upon work undertaken with employees in the private sector in South Africa Citation47.
Another important factor that affects the ongoing motivation of health workers is their experience of work results or outcomes Citation29 and the feedback they receive. The framework shows the different modalities through which providers should receive feedback, even though the qualitative research indicated that some of the mechanisms do not work well.
Study context
The study was carried out in Lindi Rural and Mtwara Rural Districts in the South of mainland Tanzania, Nouna and Solenzo Districts in North–West Burkina Faso, and Builsa and Kassena-Nankana Districts in North-Eastern Ghana. These are all deprived, rural areas where community livelihoods are vulnerable, infrastructure is poorly developed, and the working conditions of health staff are difficult.
Whilst there are very important differences among Ghana, Tanzania, and Burkina Faso, at primary health care level in these disadvantaged districts there are also strong commonalities. In all three countries, maternal and child health services feature prominently in the essential health package at primary level. Moreover, all the countries face critical shortages of skilled health staff and challenges to recruit and retain staff in rural facilities Citation48–Citation50. It should be noted that from the outset, it was assumed, based upon knowledge of the setting, that the providers in the study context were literate in either English (Ghana), French (Burkina Faso), or Kiswahili (Tanzania).
Methods
From the start, the scope of the instrument was clarified. It was decided that two further tools would complement it. The first would explore changes in MNH provider knowledge as a result of the interventions. The second would monitor the overall performance of facilities through the use of a quality composite index. These two tools are not discussed further here.
It was also agreed that the instrument would be implemented at baseline, before the interventions were introduced at facility level, and then at two subsequent intervals to capture possible changes in the shorter and longer term. It should be clarified that the instrument actually only affords the opportunity to monitor changes over time, through a comparison of the findings from subsequent rounds of data collection to the baseline. Furthermore, a plan was made for further qualitative research, in the form of in-depth interviews, to be conducted after the analysis of the data from each subsequent use of the instrument to facilitate a deeper understanding of any changes shown.
The process of developing the instrument was informed by a literature review, reference to the QUALMAT conceptual framework and the aforementioned, preliminary qualitative research. Scientific literature was retrieved from PubMed, Science Direct, PsycINFO, and the Anthropological Index Online. Further literature was sought by means of a request to experts in this field.
Following on from this, the project collaborators brainstormed to identify constructs where changes were expected due to the pilot interventions. These included contextual influences such as competence strengthening, work organization, quality of MNH services, and the role of performance and community relations. Changes at the level of the individual MNH providers were also expected. These were differentiated into attitudes (how MNH providers think and feel) and behavior (what they do) Citation30. Constructs covered by the former included self-efficacy, motivation, pride, and task meaningfulness. The latter included timeliness and attendance, behavior to patients, conscientiousness, and cooperation, which are all constructs that lend themselves to a degree of verification by others.
For validation, the proposed constructs were presented to a panel of experts from the three countries involved. They were requested to rank them in terms of their influence on provider motivation and the extent to which they would be likely to be affected by the interventions. This was to ensure a sub-Saharan lens was applied to the instrument from the outset Citation51 and to maximize the possibility of the instrument focusing upon constructs that were applicable in all settings.
In a subsequent step, items were elaborated for each construct. As Fontaine observed that issues of functional equivalence are not restricted to theoretical constructs but can also emerge in regards to measurement aspects Citation52, reference was made, wherever possible, to tools that had already been used in the context of developing countries. Each construct had at least three items Citation18. Care was taken to formulate the items in as straightforward a manner as possible given the intended target audience. A total of 35% of the items were negatively phrased to reduce response–set bias Citation19.
The items pertaining to provider behavior (timeliness, attendance, etc.) were also included in a further, short instrument for completion by a peer. Such verification has been sought from the managers of health workers Citation30. However, in these study settings, facility managers were still involved in the delivery of clinical care. In addition, the strong influence of the hierarchy revealed by the preliminary qualitative research led to concerns that this mechanism could influence the findings. It was therefore decided to use a peer approach. A peer was defined as another colleague based at the same facility who was also involved in the study.
At this stage, senior health staff from the three countries informed of the project were sent the instrument. They were asked to reflect upon whether they thought it would actually measure what was intended and to fill it out. As a result several items were further simplified, but overall no constructs or items were questioned so confirmation of face validity was assumed.
For both parts of the instrument, a four-point Likert scale was used with the options: ‘strongly agree’, ‘agree’, ‘disagree’, and ‘disagree strongly’. A four-point scale was thought to be relatively straightforward and therefore preferable for the target group. This decision was only taken after considering whether a ‘don't know’ option might be necessary. However, this was not found to be the case. Moreover, others observed that little use was made of this option even when it was available Citation19. The output was a final version for pre-test which contained 64 items for self-administration and 12 to be completed by one of the respondent's co-workers (peer) so that perceptions could be compared and limited verification undertaken. The instrument was introduced with a text adapted from that used in the Hackman and Oldham Job Diagnostic Survey Citation36. Given the varying understandings of motivation that were observed in the qualitative research, and to avoid ‘socially desired behaviour’ responses Citation38, the actual term ‘motivation’ was not included in either the title or the introduction to the instrument.
Up until now the development was informed as far as possible by input from all the three countries. For simplicity, Ghana was selected as the country for the pretest. This was because the instrument could be applied in English which was the language in which the development had taken place. The pretest was conducted with 70 primary level health workers in the Bongo District of the Upper East Region of Ghana. This number of health workers was chosen as being just sufficient for the purpose of factor analysis Citation53, whilst also in keeping with the number of participants in the study overall.
The pre-test revealed that the use of the Likert scale required detailed introduction in the field, as expected. It was clarified to these health workers that there would be no feedback on the findings as they were sought for finalization of the instrument only. Refreshments and stationary were provided as tokens of appreciation. The respondents were assured about confidentiality. However, at this stage, to facilitate the work of the country researchers, the name of the staff member for peer assessment was written on the peer instrument. Although the peer that filled out this instrument did so anonymously, the issue of confidentiality was questioned by some of the respondents as they filled out this part of the instrument. To address this, a numbering system was used to pair up the self and peer responses when the final version was implemented.
The data was entered using Microsoft Excel. This process was then double-checked and identified errors were corrected. Item difficulty, that is, a measure of the ability of items to differentiate between subjects, was then calculated and 14 items with extreme difficulty (p<0.3 or p>0.7) were excluded Citation54. Internal consistency was judged by Cronbach's α coefficients using a criterion of 0.70 Citation55. For the overall instrument Cronbach's α was 0.871 and the split half reliability (Spearman Brown Coefficient) was 0.737, both of which were considered to be satisfactory Citation54. However, the internal consistency of the single constructs was less convincing as shown in .
Table 1. Overview of Cronbach's α coefficients for constructs from pre-test data
Bennett et al. argued in their pioneering work in Jordan and Georgia that Cronbach's α scores of 0.60 might also be considered acceptable in such pilot situations Citation30. Constructs included in the tool in Kenya gave Cronbach's α coefficients of between 0.36 and 0.64 Citation19, although it should be qualified that their intention was to develop a short, practical tool meaning the number of items per construct was sometimes small, which has an effect upon such scores.
An exploratory factor analysis was carried out. The scree plot that was generated to explore the overall distribution of the data indicated a three-factorial structure. Despite some overlapping, the two main factors were broadly equivalent to the theoretically assumed dimensions management and performance. The items loading on management covered issues of work tools and staffing as well as promotions and further training. The items loading on performance had more to do with feedback from managers, co-workers, and the community as well as the reputation of the facility in general. Items loading on the third factor pertained to individual health workers and covered their self-efficacy, motivation, commitment, and behavior at work. All three factors relate back to the conceptual framework. A total of 14 items loaded to the management factor, giving a Cronbach's α of 0.786 and explaining 15.8% of the variance. A total of 13 items loaded to the performance factor, giving a Cronbach's α of 0.829 and explaining 14.6% of the variance. Finally, a total of 15 items loaded to the third factor, with generally lower loadings. The Cronbach's α was 0.815 and they explained 9.7% of the variance. Given that the pre-test version was considered too long, eight items that did not load highly (loading 0.3) to any of the three factors were also removed to achieve a lean and focused instrument.
An overview of the items and constructs that did not perform well and thus removed to finalize the instrument is provided with a discussion in the next section.
The final version of the instrument was then translated into French and Kiswahili using the back translation method and further pre-testing for quality control. A short set of instructions was developed to ensure that a streamlined approach was taken to the implementation in all three countries. During development, it was flagged that collecting information on issues such as provider behavior from peers could be potentially sensitive. In particular, cognitive dissonance might play a role and cause viewpoints to differ. Cognitive dissonance refers to the way people alter their perceptions to reduce the discomfort experienced by holding conflicting views, such as knowing what one should do in a given situation, yet privately acknowledging what one really does Citation56. It was therefore agreed that feedback sessions would be arranged to present and discuss any differences that emerged between the self and peer assessments in an organized and constructive manner.
As there had been errors with the use of Excel to enter the pre-test data, an epi-data entry-mask was developed for use at baseline. The mask showed the coding of the responses very clearly next to each item (1 = agree strongly; 2 = agree; 3 = disagree; 4 = disagree strongly), and only allowed for one response per item or a zero if no response had been given.
Baseline data was collected with the instrument in all three countries in September–October 2011. In each country, 12 facilities had previously been purposely selected according to certain criteria, including being based in a rural area (>10 km from a town) whilst fulfilling certain basic requirements of infrastructure (e.g. electricity supply) needed for the pilot interventions. No sampling was undertaken and all the MNH providers (83 in Burkina Faso, 50 in Ghana, and 62 in Tanzania) at these facilities were approached. All those agreeing to take part signed consent forms. Willingness to take part in the study was high in all the settings and nobody refused. Whilst these numbers are quite small, they are nonetheless sufficient to identify an effect, should one exist Citation57. On average it took 1.5 hours to introduce, explain, and administer both parts of the instrument.
Analysis of the baseline data in all three countries was carried out using SPSS. Mean responses to the three main aspects (management, performance, and individual) were compared across the demographic variables for any differences of significance. Un-weighted means were used as all the aspects were afforded the same importance. The mean was chosen rather than the sum to facilitate interpretation of scores, in which 2.5 is the neutral midpoint on the 4-point response set. The professions of the respondents were re-coded into lower level and more higher trained cadres, and the number of dependents that a respondent was financially responsible for were grouped (0–4, 5–9, 10 + ) for analysis. Regression analysis was used with the respondents’ age, total years at school, length of time in their current level/position, and at their current rural workplace.
Ethical clearance was granted by the Institutional Review Board at the Navrongo Health Research Centre (ID NHRCIRB 085) for Ghana; the Muhimbili University of Health and Allied Sciences Ethical Review Committee (ref no. MU/AEC/VOLXIII/96) for Tanzania; and the Ethics Committee for Health Research for Burkina Faso (No.2010.05/CLE/CR).
Results and discussion
Before presenting the final instrument, it is considered worthwhile to show and discuss which aspects did not perform well during the pre-testing.
shows that the constructs that did not perform well when used at primary care level in Ghana included work meaningfulness, energy level/burnout, whether a provider feels valued/exploited, attitudes to patients, behavior to patients, conscientiousness, and timeliness/attendance. In addition, single items from the constructs self-efficacy, pride/shame, motivation, satisfaction, and cooperativeness also failed to perform well.
Table 2. Constructs and items that did not perform well psychometrically
At the outset, it should be noted that nine of the 22 items that were eliminated had been newly developed based upon our preliminary qualitative research. It is likely that these items were under-researched. For example, with regard to the construct work meaningfulness, the thrust of the items would appear to be important as all respondents agreed with wanting to serve their people and provide them with important services. It is possible that positive bias, the wish to respond in a socially desired way Citation58 or cognitive dissonance may all have had an influence here. These concerns also apply to the constructs conscientiousness and timeliness/attendance. Items about dependability at work and doing things without being told were all responded to positively across the board despite the qualitative research having indicated that serious problems existed in precisely these areas.
With regard to the construct energy level/burnout, the intention was to take this issue of concern up but not to make it a strong area of focus. As a result the number of items may have been too few. Future efforts would be well advised to follow Citation32 and refer to the subscales of Maslach's Burnout Inventory Citation59, as these have also been found to demonstrate reliability when used with health professionals in Africa Citation60.
All the providers strongly disagreed with the items about the sufficiency of their salary. This was despite the fact that the items had previously performed adequately in other settings. This result is perhaps not surprising, and suggests too narrow and undifferentiated a focus upon financial aspects. Conversely the aspect of motivation that did not perform well was the item that provoked the respondents by asking whether the salary was the main reason for them to do their work. This was strongly rejected. The preliminary qualitative research endorses this view with some of the respondents in all three countries underlining that this was absolutely not the reason that they took up a health profession, whilst others blamed the providers they considered to be driven by financial rewards for the poor quality of care.
It is interesting that the construct ‘attitudes to patients’ performed so poorly. The internal consistency of the items was unacceptable and the items also failed to load to any of the three factors. This construct sought to capture interpersonal aspects that were shown to be important for the quality of care in the preliminary qualitative phase. This was therefore a sensitive area, as were the points raised in the construct ‘behavior to patients’, such as politeness and whether a companion could stay with a woman in labor. The question must be raised of how far providers engage with individual patients. Most of the statements made by providers about their motivation to help referred to the patients in their collective form as ‘the community’. Creating distance between oneself and the individuals that may suffer as a result of one's actions is a strategy people often use to reduce cognitive dissonance Citation61.
Overall, a further nine of the 22 items that were eliminated from the self-administered instrument were negatively phrased. These items came from a variety of sources including having been developed by authors. It is possible that these questions were less well understood. Culturally, it is also plausible that respondents might instinctively have been more likely to reject abruptly phrased negative statements. This phenomenon has been observed in cultures in which disagreement is not voiced directly Citation62.
Whilst the use of the factor analysis facilitated the achievement of a parsimonious instrument, it was precisely some of the constructs that are most intricately linked to the concept of motivation that did not perform well and were removed. Had the development not been constrained by the tight project schedule, more work could have been usefully invested to achieve their inclusion. For example, further qualitative research could have been undertaken to better understand and refine the constructs, whilst the possible effect of cognitive dissonance could have been explored through carefully moderated discussions of alternative views Citation56.
At pre-test the responses to all items about health worker behavior included in both the self-administered and the peer instruments were the same and, in both cases, overwhelmingly positive. This was despite indications to the contrary, for example, absenteeism and inter-disciplinary staff conflicts from the preliminary qualitative research. The sanctions that were further shown by this research to result from error making and the aforementioned confidentiality concerns may explain this.
The final version of the instrument is shown in , with an excerpt of the formatting provided in .
Fig. 2. Excerpt from final formatted version.
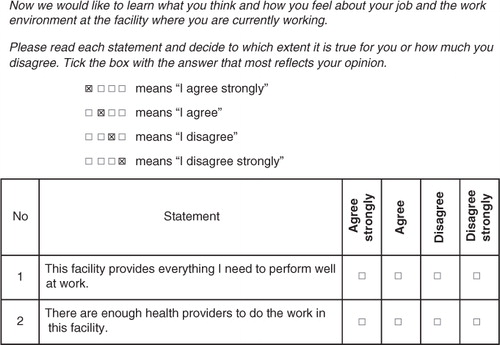
Table 3. Final version of the instrument with sources
Use of the final instrument in all three countries
Burkina Faso
In Burkina Faso, 47 of the respondents were female and 36 male. The mean age was 32 years, with the majority of respondents aged between 25 and 35 years. A total of 45 were single and 38 were married. Of those that were married, 16 lived in separation from their partner due to the rural nature of the posting, with seven living in separation from their children for the same reason. The mean number of dependents the providers were responsible for was five.
Sixty-five of the respondents may be classified as lower-level cadres (27 auxiliary midwives, 22 community outreach workers, and 16 auxiliary nurses), and 18 were more highly trained (16 registered nurses and 2 midwives). The respondents had undergone a mean total schooling time of 9 years. Seventy had been working in their positions and at their current health facility for 3 years or less. Just five respondents were working in their home district.
These findings bear testimony to the high levels of staff turnover and specific challenges of recruiting female providers to rural areas that were repeatedly raised by managers in the preliminary qualitative research. The latter was further lamented as having a negative effect upon the acceptability of MNH services. Most health staff were young with limited work experience. Many were also still single indicating that they were in the early stages of their career. The minority belonged to more highly trained cadres and very few actually originated from the rural areas in question. Almost half of those that are married live separated from their partner due to the rural nature of their posting.
Most of the variables (see the demographic section of for an overview) did not have an effect upon the mean responses (not shown). Age and length of time spent in one's current position were exceptions. As age had an effect in all three countries, it is discussed at a later stage.
shows that the longer a respondent has been at their current level, the more positive they become about the items pertaining to management items. It is possible that with time the respondents better understand the difficulties attached to, and efforts made to accomplish, managerial tasks in this context.
Table 4. Effect of time in current position on mean responses to the three main aspects in Burkina Faso
Ghana
In Ghana, all of the respondents were female. The mean age was 45 years, with the range spanning 23–62 years. A total of 23 were married, 13 were single, with a further 14 either widowed or divorced. Of those that were married, two lived in separation from their partner due to the rural nature of the posting, and three lived in separation from all or some of their children for the same reason. The respondents were responsible for a mean of five dependents each.
The respondents were midwives, public health nurses, or community health nurses. The 15 community health nurses are considered to be a lower-level cadre in the Ghanaian health system, although the entry condition of high school completion is higher for this group of cadres than in the other two countries. The respondents had undergone a mean total schooling time of 11.5 years. The mean number of years the respondents had been working at their current level was eight. The mean number of years they had been working at their current health facility was three, with a range of 1–12 years. A total of 26 of the respondents were working in their home district.
The profile of these health workers suggest that in Ghana there has been some success in recruiting more highly qualified staff to rural areas, although the total number of staff available at the facilities was lower overall. Moreover, the area of MNH was found to be exclusively staffed by women, with midwives sometimes also managing facilities. In these areas of rural Ghana, older, more experienced staff were also found and very few were separated from family members due to their work. This would suggest that retention policies are in place. Community health nurses are generally recruited from, and sponsored by, districts according to need. Upon qualifying they are then obliged to work in that district for a set period.
Most of the variables did not have an effect on the mean responses (not shown). Factors such as age, and time spent both in the current position and at the current facility were exceptions.
shows that, as in Burkina Faso, the longer the respondents work at their current level, the more positive their responses to the items about management aspects become. Again it is possible that with time the respondents’ appreciation of the efforts made by their managers’ increases.
Table 5. Effect of time in current position on mean responses to the three main aspects in Ghana
shows that as the time spent at the current facility increases, the responses to the items about individual dimensions of motivation become significantly less critical. It is plausible that with time the respondents become more in tune with how the community appreciates them, and see the impact of their work on the catchment's health status more clearly, which could serve to reinforce their motivation, commitment, and job satisfaction.
Table 6. Effect of time at current facility on mean responses to the three main aspects in Ghana
Tanzania
In Tanzania, 43 of the respondents were female and 19 male. The mean age was 40 years, with the range spanning 23–62 years. Thirty-nine were married, 20 were single, and a further three widowed. Five of those that were married lived in separation from their partner due to the rural nature of the posting. Four of these five also lived in separation from all or some of their children for the same reason. The respondents were responsible for a mean of six dependents each.
Forty-five of the respondents belonged to more highly trained professional groups (19 nurse midwives, 11 other types of nurse, 12 sub-cadres of physician, three health officers) and 17 were auxiliaries (medical or nurse attendants). The respondents had undergone a mean total schooling time of 8 years. The mean number of years spent working at the current level was nine, and at the current health facility seven. Twenty-two of the respondents were working in their home district.
These findings suggest that whilst lower-level cadres were not in the majority as in Burkina Faso (78%), they nonetheless accounted for a reasonable proportion (27%) of the workforce at the primary level facilities involved. The majority (69%) of the providers were female, but there was some male involvement. The findings further indicated that Tanzania, like Ghana but unlike Burkina Faso, has managed to post health workers from rural areas back to their home districts. The rates of separation from partner and children were thus also low. The mean time spent at the current facility was highest in Tanzania. This could either indicate that rural postings are open-ended and staff infrequently transferred in the study area, or reflect some success in staff retention.
Most of the variables did not have an effect upon the mean responses (not shown). The number of dependents the respondents were responsible for, age and the time spent at the current facility were exceptions.
The Tanzanian respondents were responsible for more dependents than those in the other settings. shows that the greater the number of dependents the more positive the respondents were in their mean responses to the items about individual aspects, such as the level of effort made, their motivation, job satisfaction, and commitment to remain at the facility. This could be due to the importance of the respondent's income to support these dependents, or to the way their profession or standing in the community brings other benefits to these dependents, which serve to further motivate them.
Table 7. Effect of the number of dependents upon mean responses to the three main aspects in Tanzania
shows that the longer the respondents remain at a facility the less critical their views about the management aspects. This could be because with time the respondents gain a greater understanding of the difficulties of managing a facility in such constrained, rural circumstances.
Table 8. Effect of time at current facility on mean responses to the three main aspects in Tanzania
shows that age had a significant effect on the responses in all three countries. In Burkina Faso and Tanzania, the older the respondents were, the more positive their responses to the items pertaining to performance aspects. This could be because they enjoy greater respect and appreciation of their work experience from the community and their co-workers. In Ghana, the older the respondent were, the more positive their responses to the items pertaining to individual aspects. Older respondents may be more reconciled with, and settled in, their rural placement and enjoy respect and appreciation which serve to reinforce their motivation, commitment, and job satisfaction. Others have also suggested that job satisfaction improves as the worker's age increases Citation63.
Table 9. The significant effect that age had upon different aspects across the three countries
Finally, the positive bias found in the peer results at pre-test were not replicated, reflecting that this was probably caused by concerns about confidentiality. shows that at first use of the final instrument in Burkina Faso and Tanzania, the peers were more critical in their assessment of their colleagues work behavior than the colleagues were about themselves. Four respondents from Tanzania returned the peer part of the instrument without having filled it in. In Ghana, the effect was different and the peers were less critical than the colleagues themselves.
Table 10. Differences between self and peer responses to the items about provider behavior from all three countries
The preliminary qualitative work can help to explain these differences; in Burkina Faso, the findings thereof suggested an openness between immediate colleagues, quite in contrast to the respect demonstrated for those in higher positions. Health workers in this setting were also very clear to separate ‘the team’ and its importance, from an individual's responsibilities – especially when it came to sanctions for poor behavior or performance at work; in Tanzania, the qualitative findings showed a degree of conflict between facility staff regarding the division of labor, as well as some snobbery between higher and lesser trained staff as also observed by others Citation18. The fact that four respondents did not fill out the peer part could indicate some discomfort with this type of assessment. In Ghana, a strong degree of competitiveness was found between the staff, which could explain why the respondents were very strict in their assessment of their own work behavior.
The results demonstrate that the instrument could be used in different languages with health workers of differing levels of schooling and training. The variables that had an effect upon the mean responses provide useful pointers on where to focus the planned, accompanying qualitative work so that any changes that the instrument may show over time can be better understood.
Transferability
There was never an intention to combine the datasets. However, there was an interest to see how well an instrument that was effectively finalized through a process of pre-testing held in one country of sub-Saharan Africa could be applied in another.
The fact that the instrument was found to require extensive introduction at pre-test had been expected, but was also a source of concern as the general level of health worker training at primary care level in Ghana was thought to be higher than in the other two countries. However, differences in the amount of introduction the instrument required in the field were not born out during their implementation in Tanzania and Burkina Faso, despite the data confirming the respondents’ lower average years of total schooling and the lesser availability of more highly qualified staff.
To further explore how the instruments had transferred, basic reliability testing was carried out using the baseline findings from Tanzania and Burkina Faso. The Cronbach's α for the Kiswahili version of the instrument was 0.820 overall, 0.633 for the management aspects, 0.619 for the performance aspects, and 0.753 for the individual aspects. The Cronbach's α for the French version was 0.808 overall, 0.615 for the management aspects, 0.516 for the performance aspects, and 0.762 for the individual health worker aspects. In both cases, the values may just be considered acceptable.
The concerns about the effects of translating from English into Kiswahili – a Bantu language with a completely different grammatical composition – being greater than those of translating into French were not confirmed. In both cases, despite the care taken to translate the instruments using the back-translation method and undertake further pre-testing to ensure comprehensibility before use, some of the internal consistency was lost. This is probably because of the highly context-specific nature of the concept of motivation Citation62, which the qualitative findings also revealed. The particularly low result from the performance aspects in Burkina Faso could have its roots in important differences found in this area by the preliminary qualitative research. This showed the use of performance management tools to be far lower, and the acceptability of encouragement and prize-giving as ways to motivate staff to be far higher than amongst the respondents from Ghana and Tanzania.
Conclusions
The results show that it is possible to undertake work of this nature at primary health care level, particularly if an effort is made to keep the formulation of the instrument as straightforward as possible and if the introduction thereof is undertaken in an appropriate and detailed manner.
However, such instruments require very lengthy preparatory periods and ongoing qualitative research during development to clarify and respond to areas of difficulty. A more extensive review of the anthropological literature and greater involvement of anthropologists in any future such endeavors is highly recommended.
The effort needed to adapt such an instrument for use in different countries within the region of sub-Saharan Africa should not be underestimated.
QUALMAT
The QUALMAT research project funded as part of the 7th Framework Programme of the European Union (grant agreement 22982) is a collaboration between the Centre de Recherche en Santé de Nouna (Burkina Faso), Ghent University (Belgium), Heidelberg University (Germany), Karolinska Institute (Sweden), Muhimbili University of Health and Allied Sciences (Tanzania), and Navrongo Health Research Centre (Ghana). The overall objective of this research is to improve the motivation and performance of health workers and ultimately the quality of pre-natal and maternal care services. The intervention packages include the development and implementation of a system of performance based incentives and a computer-assisted CDSS based on WHO guidelines. The interventions are evaluated in a pre-post controlled study design in rural Burkina Faso, Ghana, and Tanzania between the years 2009 and 2014.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Author contributions
HP: was involved in the literature review and development of the instruments, coordinated their translation using the back-translation method, led the analysis, prepared the first draft of the paper.
MTL: led the development of the instruments, contributed substantially to the paper.
CW: was involved in the literature review, development and refinement of the instruments, contributed to the paper.
GAA: contributed to the development of the instrument, undertook the pre-test, collected and analyzed the baseline data in Ghana.
DCVK: contributed to the development of the instrument, tested the Kiswahili version, collected and analyzed the baseline data in Tanzania.
MK: contributed to the development of the instrument, tested the French version, collected the baseline data in Burkina Faso.
JB: technically supported the development and finalization of the instruments and the analysis of the baseline data.
GKW: backstopped the development of the instruments and the interpretation of the baseline data and contributed to the article.
MM: gave feedback on the literature review, provided input for the discussion on why certain constructs may not have worked well, contributed to the article.
RS: designed the study, contributed to developing the instruments, contributed to the article.
Acknowledgements
Untold gratitude is extended to the providers in Ghana, Tanzania, and Burkina Faso who agreed to invest their time and use the instrument.
To Maurice Yé and Ali Sié from Burkina Faso, to Siriel Massawe from Tanzania, and John Williams from Ghana and other colleagues from the partner institutions that partook in the validation of the instruments.
Whilst developing the pre-test version of the instrument in March/April 2011, the following experts kindly responded to a request for literature and documents: John Arudo, Marjolein Dielemann, Carmen Dolea, Delanyo Dovlo, Riitta-Liisa Kolehmainen-Aitken, Evelyn Kortum, Tim Martineau, Margaret Usher-Patel.
Thanks are extended to Valerie Louis for her help in preparing and translating the data-entry mask, to Vitus Atuah Atanga for his support with the analysis of the Ghana data and to Kirsten Külker for her assistance with the graphic and design work on the conceptual framework.
Related Research Data
References
- Franco L, Bennett S, Kanfer R, Stubblebine P. Determinants and consequences of health worker motivation in hospitals in Jordan and Georgia. Soc Sci Med. 2004; 58: 343–55. 10.3402/gha.v5i0.19120.
- Dussault G, Dubois CA. Human resources for health policies: a critical component in health policies. Hum Resour Health. 2003; 1: 1.10.3402/gha.v5i0.19120.
- Kak N, Burkhalter B, Cooper MA. Measuring the competence of healthcare providers. Bethesda, MD: Published for the US. Agency for International Development by the Quality Assurance (QA) Project. ; 2001. Available from: http://www.hciproject.org/sites/default/files/Measuring%20the%20Competence%20of%20HC%20Providers_QAP_2001.pdf [cited 23 March 2012].
- Southgate L, Dauphinee D. Maintaining standards in British and Canadian medicine: the developing role of the regulatory body. BMJ. 1998; 316: 697–700. 10.3402/gha.v5i0.19120.
- Leonard KL, Masatu MC, Vialou A. Getting doctors to do their best: the roles of ability and motivation in health care quality. J Hum Resour. 2007; 42: 682–700.
- Maestad O, Torsvik G. Improving the quality of health care when health workers are in short supply. Christian Michelsen Institute. Bergen, 2008
- Leonard KL, Masatu MC. Professionalism and the know-do gap: exploring intrinsic motivation among health workers in Tanzania. Health Econ. 2010; 19: 1461–77. 10.3402/gha.v5i0.19120.
- Kreitner R. Management6th ed. Houghton Mifflin Company. Boston MA, 1995
- Denhardt RB, Denhardt JV, Aristigueta MP. Managing human behaviour in public and nonprofit organisations. Sage, Thousand Oaks. CA, 2008
- Campbell JP, McCloy RA, Oppler SH, Sager CE. A theory of performance. In: Schmitt E, Borman WC, Associates. Personnel selection in organizations. San FranciscoCA: Jossey-Bass. 1993, pp. 35–70.
- Pardee RL. Motivation theories of Maslow, Herzberg, McGregor and McClelland. A literature review of selected theories dealing with job satisfaction and motivation. ; 1990. Available from: http://www.eric.ed.gov/PDFS/ED316767.pdf [cited 24 June 2012].
- Dolea C, Adams O. Motivation of health care workers-review of theories and empirical evidence. Cah Sociol Demogr Med. 2005; 45: 135–61.
- Kanungo RN, Mendonca M. Introduction: motivational models in developing countries. Work motivation: models for developing countries. Kanungo RN, Mendonca MSage. New Delhi, 1994; 14–24.
- Janssen PPM, Jonge JD. Specific determinants of intrinsic work motivation, burnout and turnover intentions: a study among nurses. J Adv Nurs. 1999; 29: 1360–9. 10.3402/gha.v5i0.19120.
- World Health Organization. The World Health Report 2006 – working together for health. Geneva: WHO. 2006. Available from: http://www.who.int/whr/2006/whr06_en.pdf [cited 24 June 2012].
- Stamps P. Nurses and work satisfaction: an index for measurement2nd ed. Health Administration Press. Chicago IL, 1997
- Martín J, Cortés JA, Morente M, Caboblanco M, Garijo J, Alberto R. Características métricas del Cuestionario de Calidad de Vida Profesional (CVP-35). Gac Sanit. 2004; 18: 129–36. 10.3402/gha.v5i0.19120.
- Chandler CIR, Chonya S, Mtei F, Reyburn H, Whitty CJM. Motivation, money and respect: a mixed methods study of Tanzania non-physician clinicians. Soc Sci Med. 2009; 68: 2078–88. 10.3402/gha.v5i0.19120.
- Mbindyo PM, Blaauw D, Gilson L, English M. Developing a tool to measure health worker motivation in district hospitals in Kenya. Hum Resour Health. 2009; 7: 40.10.3402/gha.v5i0.19120.
- Mbindyo P, Gilson L, Blaauw D, English M. Contextual influences on health worker motivation in district hospitals in Kenya. Implement Sci. 2009; 4: 43.10.3402/gha.v5i0.19120.
- Manongi RN, Marchant TC, Bygbjerg IC. Improving motivation among primary health care workers in Tanzania: a health worker perspective. Hum Resour Health. 2006; 4: 6.10.3402/gha.v5i0.19120.
- Dieleman M, Cuong PV, Anh LV, Martineau T. Identifying factors for job motivation of rural health workers in North Viet Nam. Hum Resour Health. 2003; 1: 10.10.3402/gha.v5i0.19120.
- Wiskow C. Personalmanagement im Gesundheitssystem Kameruns: wenn Reformen auf Menschen treffen [Personnel management in the health system in Cameroon: when reforms and people meet]. Verlag Hans Jacobs. Lage, 2001
- Satchi M, Temple J. Labor markets and productivity in developing countries. Rev Econ Dyn. 2009; 12: 183–204. 10.3402/gha.v5i0.19120.
- Machungwa PD, Schmitt N. Work motivation in a developing country. J Appl Psychol. 1983; 68: 31–42. 10.3402/gha.v5i0.19120.
- Herselman S. Performance motivation among employees of a wholesale company. S Afr J Ethnol. 2001; 24: 1–10.
- Mulinge M, Mueller CW. Employee job satisfaction in developing countries: the case of Kenya. World Dev. 1998; 26: 2181–99. 10.3402/gha.v5i0.19120.
- Kamoche K. Contemporary developments in the management of human resources in Africa. J World Bus. 2011; 46: 1–4. 10.3402/gha.v5i0.19120.
- Franco LM, Bennett S, Kanfer R. Health sector reform and public sector health worker motivation: a conceptual framework. Soc Sci Med. 2002; 54: 1255–66. 10.3402/gha.v5i0.19120.
- Bennett S, Franco LM, Kanfer R, Stubblebine P. The development of tools to measure the determinants and consequences of health worker motivation in developing countries. Major Applied Research 5, Technical Paper 2. BethesdaMD: Partnerships for Health Reform Project, Abt Associates Inc. 2001. Available from: http://phrplus.org/Pubs/m5tp2.pdf [cited 24 June 2012].
- Penn-Kekana, L, Blaauw D, San TK, Monareng D, Chege J. Nursing staff dynamics and implications for maternal health provision in public health facilities in the context of HIV/AIDS. Report for Population Council and Frontiers in Reproductive Health. ; 2005. Available from: http://www.popcouncil.org/pdfs/frontiers/FR_FinalReports/SA_QOC.pdf [cited 24 June 2012].
- McAuliffe E, Bowie C, Manafa O, Maseko F, MacLachlan M, Hevey D, et al.. Measuring and managing the work environment of the mid-level provider – the neglected human resource. Hum Resour Health. 2009; 7: 13.10.3402/gha.v5i0.19120.
- Campbell JP, Pritchard RD. Motivation theory in industrial and organisational psychology. Handbook of industrial and organisational psychology. Dunnette MDRand McNally. Chicago IL, 1976; 63–130.
- Bandura A. Self-efficacy mechanism in human agency. Am Psychol. 1982; 37: 122–47. 10.3402/gha.v5i0.19120.
- Farmer S, Seers A. Time enough to work – employee motivation and entrainment in the workplace. Time Soc. 2004; 13: 265.10.3402/gha.v5i0.19120.
- Hackman JR, Oldham GR. Motivation through the design of work: test of theory. Organ Behav Hum Perform. 1976; 16: 250–79. 10.3402/gha.v5i0.19120.
- Prytherch H, Kakoko DCV, Leshabari MT, Sauerborn R, Marx M. Maternal and new-born health care providers in rural Tanzania: in-depth interviews exploring influences on motivation, performance and job satisfaction. Rural Rem Health. 2012; 12: 2072.
- Mathauer I, Imhoff I. Health worker motivation in Africa: the role of non-financial incentives and human resource management tools. Hum Resour Health. 2006; 4: 24.10.3402/gha.v5i0.19120.
- Bradley S, McAuliffe E. Mid-level providers in emergency obstetric and newborn health care: factors affecting their performance and retention within the Malawian health system. Hum Resour Health. 2009; 7: 14.10.3402/gha.v5i0.19120.
- Mbilinyi D, Daniel ML, Lie GT. Health worker motivation in the context of HIV care and treatment challenges in Mbeya Region, Tanzania: a qualitative study. BMC Health Serv Res. 2011; 11: 266.10.3402/gha.v5i0.19120.
- Bennett S, Franco LM. Public sector health worker motivation and health sector reform: a conceptual framework. Major Applied Research 5, Technical Paper 1. BethesdaMD: Partnerships for Health Reform Project, Abt Associates Inc. 1999. Available from: http://www.hrhresourcecenter.org/node/1095 [cited 24 June 2012].
- Schuler SR, McIntosh EN, Goldstein MC, Pande BR. Barriers to effective family planning in Nepal. Stud Fam Plann. 1985; 16: 260–70. 10.3402/gha.v5i0.19120.
- Leonard KL, Masatu MC. Comparing vignettes and direct clinician observation in a developing country context. Soc Sci Med. 2005; 61: 1944–51. 10.3402/gha.v5i0.19120.
- Marquez L. Helping healthcare providers perform according to standards. BethesdaMD: Published for the US. Agency for International Development (USAID) by the Quality Assurance Project. 2001. Available from: http://158.132.116.146/adh/4_4Sframework/3_Services_n_commodities/1_Healthsystem/Marquez_providers_standards.pdf [cited 23 March 2012].
- Mutizwa-Mangiza D. The impact of health sector reform on public sector health worker motivation in Zimbabwe. Partnerships for health reform project. Major Applied Research 5, Working Paper 4. Bethesda., USA; 1998. Available from: http://www.healthsystems2020.org/content/resource/detail/1033/ [cited 24 June 2012].
- Perry C, LeMay N, Rodway G, Tracy A, Glaer J. Validating a work group climate assessment tool for improving the performance of public health organisations. Hum Resour Health. 2005; 3: 10.10.3402/gha.v5i0.19120.
- Lin PY. The correlation between management and employee motivation in Sasol Polypropylene business. , South Africa, Master's thesis submitted to the Faculty of Economics and Management Sciences, University of Pretoria; 2007. Available from: http://upetd.up.ac.za/thesis/available/etd-08042008-192827/unrestricted/dissertation.pdf [cited 23 March 2012].
- National Health Development Plan., Plan national de développement sanitaire 2011–2020, [National Health Development Plan]Ouagadougou. ; 2011. Available from: http://www.cooperacionaragon.com/ongs/attachments/197_8-%20PLAN%20NACIONAL%20DE%20DESARROLLO%20SANITARIO_PNDS_2011-2020_Version_finale_SP-PNDS.pdf [cited 21 March 2012].
- Tanzanian Ministry of Health and Social Welfare. (MOHSW): human resources for health strategic plan 2008–2013. Dar-es-Salaam. ; 2008. Available from: http://hdptz.esealtd.com/fileadmin/documents/Key_Sector_Documents/HRH_Documents/Human_Resources_for_Health_Strategic_Plan-_2008--2013_.pdf [cited 24 June 2012].
- Snow RC, Asabir K, Mutumba M, Koomson E, Gyan K, Dzodzomenyo M, et al.. Key factors leading to reduced recruitment and retention of health professionals in remote areas of Ghana: a qualitative study and proposed policy solutions. Hum Resour Health. 2011; 9: 13.10.3402/gha.v5i0.19120.
- Airhihenbuwa CO. On being comfortable with being uncomfortable: centering an Africanist vision in our gateway to global health. Health Educ Behav. 2007; 34: 31–42. 10.3402/gha.v5i0.19120.
- Fontaine JRJ. Equivalence. Encyclopedia of social measurement. Kempf-Leonard KAcademic Press. San Diego CA, 2005; 803–13.
- Guadagnoli E, Velicer WF. Relation of sample size to the stability of component patterns. Psychol Bull. 1988; 103: 265–75. 10.3402/gha.v5i0.19120.
- Fisseni HJ. Lehrbuch der Psychologischen Diagnostik3rd ed. Hogrefe. Göttingen, 2004
- Nunnaly J. Psychometric theory. McGraw-Hill. New York NY, 1978
- Spencer DG, Myers S. Social psychology3rd ed. McGraw-Hill Ryerson. TorontoCanada, 2006
- Cohen J. Statistical power analysis for the behavioural sciences2nd ed. Lawrence Erlbaum Associate Publishers. Hillsdale NJ, 1988
- Smith PB. Acquiescent response bias as an aspect of cultural communication style. J Cross Cult Psychol. 2004; 35: 50–61. 10.3402/gha.v5i0.19120.
- Maslach C, Jackson SE. Maslach burnout inventory manual2nd ed. Consulting Psychologists Press Inc. Palo Alto CA, 1993
- Thorsen VC, Tharp ALT, Meguid T. High rates of burnout among maternal health staff at a referral hospital in Malawi: a cross-sectional study. BMC Nurs. 2011; 10: 9.10.3402/gha.v5i0.19120.
- Bandura A. Social learning theory. Prentice Hall. Eaglewood Cliff NJ, 1977
- Fischer R, Miu-Chi Lun V. Measuring cognition and motivation across cultural groups. Handbook of motivation and cognition across cultures1st ed. Sorrentino RM, Yamaguchi SAcademic Press. San Diego CA, 2008; 565, 567–89.
- Lee R, Wilbur E. Age, education, job tenure, salary, job characteristics and job satisfaction: a multivariate analysis. Hum Relat. 1985; 38: 781–91. 10.3402/gha.v5i0.19120.