Abstract
Objectives : To describe the effects of a broad empowerment programme among female sex workers (FSWs) in Bangalore,Footnote1
1Meaning ‘progress’ (in Kannada – an Indian language)
India, which seeks to develop the capacities of these women to address the issues that threaten their lives and livelihoods.Design : This study is based on a comprehensive, on-going HIV-prevention and empowering programme, known as Pragati, which reaches out to approximately 10,000–12,000 FSWs in Bangalore each year. The programme has been designed in collaboration with the sex worker community and provides a personalised set of services, which include STI prevention and treatment services, crisis-response facilities, de-addiction services, and microfinance support all of which have been tailored to adequately fulfil each woman's needs. During the period examined by this study, the programme reached out to 20,330 individual FSWs [median (IQR) age 28 (24–35) years]. The programme's personal records of the participating FSWs were used for this descriptive study.
Results : Between 2005 and 2010, the number of participating FSWs increased from 2,307 to 13,392. These women intensified their contact with the programme over time: the number of programme contacts increased from 10,351 in 2005 to 167,709 in 2010. Furthermore, data on the effects of crisis-response facilities, de-addiction and microfinance services, condom distribution schemes, and STI diagnosis and treatment showed an accumulating involvement of the participating FSWs in these programme services.
Conclusion : This programme, which focuses on social and economic empowerment among FSWs, is successful in reaching and involving the target population.
India has the world's third largest population of people living with HIV with an estimated 2.4 million (0.31%) people in 2009 Citation1. The majority of HIV infections in India (87.4%) are heterosexually transmitted due to unprotected sex Citation1. The HIV prevalence among high-risk groups in 2009 was 9.2% for injection drugs users (IDU); 7.3% for men who have sex with men (MSM); 2.5% for people with sexually transmitted infections (STIs); and 4.9% for female sex workers (FSWs). Commercial sex is considered to be the primary driver of the HIV epidemic in India, with an estimated 1.26 million FSWs living in India Citation1. Within the National AIDS Control Programme (NACP), that is now in its fourth phase (2012–2017), FSWs form one of the main targets of the effort to prevent new infections by interventions such as increasing condom use and treatment of STIs Citation1 Citation2. In line with these NACP initiatives, several intervention programmes have been launched in recent years, with a focus on high-risk groups in high HIV-prevalence areas in India Citation2–Citation4.
Pragati (meaning ‘progress’ in Kannada, an Indian language) is one of the leading innovative programmes, which have gone to scale in India. It is a large intervention programme among FSWs in Bangalore, the capital city of Karnataka with an estimated population of 9.59 million (Bangalore District) Citation5. The hypothesis of the programme is that FSWs should be socially and economically empowered to enable them to protect themselves from STIs, including HIV and AIDS, and other health threats. The main goals of the Pragati programme are to 1) reduce transmission of HIV and STIs, 2) improve the well-being of FSWs, and 3) develop the capacities of the women to protect and respond to key threats to their lives and livelihoods. The community of FSWs is organised in a sex workers collective called Swathi Mahila Sanga (SMS) and participates at all stages of the project, from conceptualisation and planning to implementation. The different activities through which the programme goals are implemented include access to drop-in centres with attached health clinics, referrals to clinics for STI and ART treatment, self-help groups for saving and credit activities, a de-addiction programme, and a crisis response mechanism for women who encounter violent behaviour.
The present article describes preliminary results of Pragati for the period between 2005 and 2010 and includes data on the performance of the different programme services.
Methods
The Pragati programme
The Pragati programme, which was launched in April 2005, was financially supported by the Bill and Melinda Gates Foundation, the Karnataka State AIDS Prevention Society (KSAPS), United Nations Development Programme (UNDP) (through its stigma reduction initiatives), and Vrutti (a livelihood resource centre). The programme is implemented by Swathi Mahila Sangha (SMS), a sex worker collective, in collaboration with Swasti, a health resource centre. SMS managed field operations, particularly community mobilisation and outreach activities, while Swasti was responsible for project management, financial management, organisation development of SMS, and technical support in areas such as strategy development, planning and monitoring, and evaluation. In addition, Swasti partner organization Vrutti was involved in setting up and managing the Women's Bank (Swathi Jyothi), and provided on-going technical support and capacity building. During the design phase, SMS and Swasti consulted members of the sex work community to understand their needs. These were prioritised and different services were designed to address these. Such community consultations continued throughout the programme period, with a minimum of two consultations annually. This helps to ensure that the programme continues to remain relevant to the community and continues to respond to the emerging needs of the community.
The sustainability of the Pragati programme was a key objective from the outset, recognising that a programme for FSWs needed to be driven by the women themselves. Pragati involved the community at all stages – from conceptualisation and planning to implementation, with the community leaders involved in all decision-making forums, e.g. strategic planning and monthly review meetings. A shadow leadership approach (recognised by UNDP's ‘Capacity is Development’ initiative as one of the top case studies) was adopted from the start of the programme, with the SMS staff shadowing the Swasti staff in all key positions. Swasti focused on institutional strengthening of the SMS as well as building its leadership. SMS has grown from a membership of 13 in 2005 to 6,649 members in 2010 and has a decentralised leadership model with a central board and zonal boards (all democratically elected), which has helped ensure transparency, effective governance, and transition of leadership from those who founded SMS to the emerging second line of leadership. The programme has facilitated the creation of a common platform for FSWs in Bangalore, which works on issues common to all sex workers in the city.
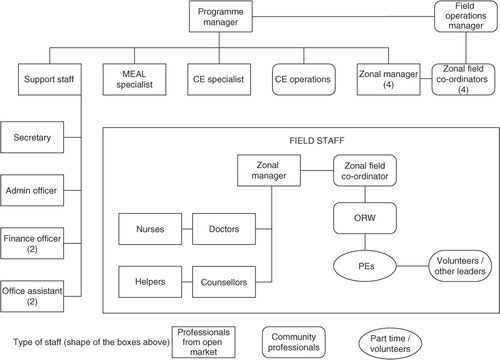
The main goal of the programme is to reduce HIV and STI transmission among FSWs and improve their well-being by developing their capacities. The programme is categorised into three broad areas of intervention: 1) protect and respond, which involves implementing an outreach strategy where peer educators and outreach workers start a dialogue with the women about the services and benefits offered through the programme. This strategy also involves sensitising primary and secondary stakeholders of the sex worker industry (such as brothel owners, pimps, and the police) to problems and needs of FSWs. 2) Improve their quality of life through identifying and addressing long-term development needs such as support for alcohol de-addiction, provision of saving and credit facilities, and creating options for alternative and diversified livelihoods. 3) Build the capacities of the women to address the issues that threaten their lives and livelihoods through strengthening group action and developing a strong collective of sex workers. An extensive explanation of the programme structure is shown in .
Fig. 1. Pragati programme structure. It shows the organisation structure of the Pragati programme staff. Peer educators (PE) and outreach workers (ORW) make up the backbone of the Pragati project at field level. Each PE is responsible for 60–120 FSWs to whom she regularly provides outreach services and encourages visiting the Pragati drop-in centres. These PEs are supported by an ORW, who is responsible for day-to-day monitoring of the PEs, providing them handholding support when required, establishing condom outlets, and the management of secondary stakeholders in her assigned area. Each ORW is responsible for 6–7 PEs. The ORWs report to zonal field coordinators who are from the sex worker collective. A zonal manager supports the field coordinators. There is an overall field operations manager from the sex worker collective (Swathi Mahila Sangha) and a programme manager from the technical support agency (Swasti Health Resource Center) who jointly oversee the project. MEAL = monitoring, evaluation and learning.
Empowerment strategy
The Pragati programme followed an empowerment approach (largely drawn from the work of Dr. Srilatha Batliwala Citation6, which places the women at the centre and seeks to address the internal and external factors that affect their vulnerability to HIV and STIs. The internal factors were the women's own beliefs, myths, and misconceptions; their low levels of confidence and capacity; lack of ability to bargain collectively; and their unquestioning acceptance of established power and social structures. The external factors were the violence and harassment afflicted upon the women, discrimination caused by social structures, and the legal framework within which the sex work industry operates. Taking into account the above factors, the programme set out to empower the women to 1) improve their ability to address their own well-being; 2) make informed choices; 3) access and control resources and; and 4) realise their rights. To achieve these overall outcomes, the programme focused on ways to improve the women's self-consciousness and confidence; build their capacities; strengthen individual and collective action; and reduce violence and harassment experienced by the women. The strategies used included capacity development, representation and democratisation, fostering leadership, creative advocacy, and alliance-building with stakeholders.
Programme setting
In 2004, the Karnataka State AIDS Control Society in collaboration with key NGOs and community-based organisations (CBO) led a mapping exercise in Bangalore to estimate the number of FSWs, thereby following the city's administrative division into seven zones. Two of the seven zones (zone 2 and 5) were already covered by targeted HIV interventions led by other NGOs/CBOs. Following the mapping, the Pragati programme was initiated in zone 1 and 3. These two zones were initially selected as SMS had been previously operating here. In November 2005, this was expanded to include zone 4 and 6. Zone 7 was not seen as a priority in 2005 as it had a small number of sex workers. As the number increased over the years, a separate state-funded intervention was initiated there in November 2008.
Participants
Between April 2005 and October 2010, all FSWs who solicited sex in the four selected zones out of the designated seven in the city of Bangalore were eligible for participation in the Pragati programme. These women were approached by peer educators and outreach workers (all former or current FSWs) of Pragati at the FSWs soliciting areas in the city. They motivated the FSWs to visit the drop-in centres by explaining what services are provided there. Within the four programme zones of Bangalore, several drop-in centres were accessible to offer the FSWs a safe place to rest and relax, take a shower, have a meal, meet peers, and to get in contact with the Pragati staff. During these contacts, FSWs were informed about the different services and areas of support available for them. Upon registration, data on socio-economic status and sex work details of the participating FSWs were obtained. Subsequently, the women could participate in the various activities of Pragati.
Pragati project activities
The various activities of Pragati range from social and economic empowerment tools like crisis-response teams that try to diminish the amount of violence and harassment that FSWs face, and financial support by microfinance systems, to health-related components such as de-addiction programmes, condom use promotion, and STI prevention and treatment strategies. Services at the drop-in centres included provision of information and counselling on HIV and AIDS; demonstration of correct and consistent condom use; distribution of free and social marketed male and female condoms; HIV and syphilis tests; de-addiction programmes; facilities for taking a bath, sleep, and entertainment; provision of relevant legal information; and saving as well as credit facilities through a microfinance institution, exclusively for FSWs. Data on services provided at the drop-in centres were recorded. When experiencing health problems, women could visit one of the participating clinics (programme-linked clinics or private referral clinics). Inside each drop-in centre, a clinic was organised where medical staff were present to provide health-related counselling, medical examinations, and treatment when needed.
Violence redressal
FSWs are easy targets for violence and harassment. One of the primary concerns of the women identified during the planning phase of the project was violent behaviour towards them by perpetrators ranging from clients, fellow sex workers, police, criminals, regular partners (not clients or husbands), to lovers and husbands. A violence redressal mechanism was established within Pragati to address issues related to violence, harassment, and trafficking. A rapid response team of women in sex work is now available (24/7) to extend timely medical, legal, and psycho-social support to the victims. This mechanism (called Swathi Nyaya Sanjeevani) educates the FSWs on their legal rights and strives to empower the women to defend themselves. It also sensitises the perpetrators of violence (such as police, criminals, pimps, and brokers in the sex working industry), on issues related to FSWs, and promotes awareness of women's rights among them. Swathi Nyaya Sanjeevani takes proactive steps to prevent violence by identifying volatile regions and establishing violence watch committees for vigilant monitoring of warning signs.
Alcohol de-addiction
Consumption of alcohol has led to many FSWs becoming alcohol dependent. When intoxicated, the women are frequently not in a strong position to insist on the use of condoms, which accentuates their risk for STI and HIV infection. Under the influence of alcohol, many women are also harassed by their clients and peers. Swathi Chetana facilitates alcohol de-addiction among women. This programme ensures that the women undergo de-addiction counselling, promotes the reduction in alcohol consumption, and motivates the women to give up alcohol. Additionally, Swathi Chetana has established linkages with the local government hospital. The hospital facilitates initial consultations with a psychiatrist or a psychologist.
Microfinance
Financial constraints are one of the precipitating factors for women to enter sex work. FSWs struggle not only with earning a decent income, but also with ensuring that the money is kept safely away from violent perpetrators who steal it from them. Many women do not have documented proof of identity; some even live in the streets. Such barriers prevent the women from accessing mainstream financial services. At times, the women take loans from non-mainstream financial services (such as money lenders) who charge exorbitant interest rates. Financial insecurity can also make them fall prey to the lures of clients who offer a better payment for sex without condoms, which increases their vulnerability to STI and HIV infection. Pragati facilitated the formation of Swathi Jyothi Mahila Vividhodesha Souhardha Sarkari Niyamita, a microfinance institution, which offers a savings bank, recurring deposit, and term loan services to the members. This institution is managed as a cooperative bank and owned by the FSWs. Women who are registered with Pragati and have membership in SMS can open a savings account and walk in to any of the drop-in centres to deposit money into their own accounts.
Promotion of condom use
Through communication for behavioural change as well as the distribution of condoms, Pragati promotes correct and consistent condom use among the FSWs. Every woman registered in the project is assessed to understand whether she has heard about, seen, or ever used condoms. The outreach team and counsellors provide demonstrations to familiarise the women with condom use and to emphasise the importance of consistent and correct use of condoms. Information on the various brands of condoms is given, and after assessing the client volume, women are provided with the required number of condoms. The programme has also established condom stock points at hotspots and maintains a distribution system to replenish it and thereby ensures that women have easy access to condoms when they need them.
Sexually transmitted infections
The FSWs who experience health problems, can visit one of the clinics in the Pragati programme for a medical examination and treatment. In these clinics, STIs are diagnosed using syndromic case management, in line with the methods suggested in the WHO guidelines Citation7, and implemented in India according to National AIDS Control Organisation (NACO) guidelines Citation8 Citation9. Reported syndromes of STIs included genital ulcers, inguinal swellings, vaginal discharge, cervicitis, and lower abdominal pain. All symptoms of the same STI, which were reported within 7 days of a previous visit (14 days for vaginitis, 21 days for inguinal swelling), were considered as the same episode of that STI.
STI treatment
All women presenting with STI symptoms received immediate treatment in conformity with the syndromic case management guidelines issued by NACO Citation7–Citation9. Irrespective of the presence of symptoms, each woman who visited any of the participating clinics for the first time or whose last visit was more than 3 months (April 2005 to March 2010) or 6 months (from April 2010 onwards) ago, received presumptive treatment for asymptomatic infections. The treatment regimens are presented in .
Table 1. STI treatment packs
Statistical analysis
Data were analysed using descriptive statistics and are presented as mean with standard deviation, median with inter quartile range (IQR), or frequency, as appropriate. Follow-up time was calculated from the date of the first contact to the date of the last contact and expressed in years. Person-time was calculated as the sum of follow-up time and expressed in person-years. Contact rates were calculated as the sum of contacts with the programme divided by the sum of person-years. Incidence rates of STIs were calculated as the sum of STI episodes divided by the sum of person-years. Both contact rates and incidence rates were stratified by year in order to examine trends over time. All analyses were performed with PASW Statistics release 18.0, SPSS Inc., Chicago, Illinois.
Results
Participants
Between 1 January 2005 and 31 October 2010, a total of 20,330 FSWs were enrolled in Pragati (). Their median age (IQR) was 28 (24–35) years, and the educational level was relatively low with almost half of the participants (49.4%) being illiterate. The participating FSWs were evenly distributed over the four zones of Bangalore, which are covered by the programme. Most FSWs solicited for sex work at home (39.9%); on the street, in parks, or other public places (30.5%); or in a rented room (15.9%). Nearly half of the FSWs (48.3%) were married, 10.0% were widowed, and 23.7% were divorced, separated from, or deserted by their husband. In 2005, when Pragati had just started, data from 2,307 FSWs were recorded during their first contact with the programme. This number increased to 10,751 FSWs in 2006 and to 13,932 FSWs who had been in contact with the programme in 2010.
Table 2. Characteristics of participating female sex workers over time (n = 20,330)
Contacts
In total, 649,438 contacts with the programme were recorded for the 20,330 FSWs between 2005 and 2010 (, ). These contacts included peer educator contacts, contacts with programme clinics, and contacts with referral clinics. At the start of the programme in 2005, four drop-in centres were opened as well as four programme clinics. After 4 years, in 2009, there were eight drop-in centres, eight programme clinics, and 90 referral clinics available for the participating FSWs. In 2010, four drop-in centres, four programme clinics, and 80 referral clinics were available. The total number of contacts with the programme increased from 10,351 contacts in 2005 to 167,709 contacts in 2010, which was primarily driven by the peer educator contacts. The contact rate for programme clinics declined between 2005 and 2010, while the contact rate for referral clinics increased during this period ().
Fig. 2. Contacts with the programme over time. Bars represent the total number of contacts per year. Line represents the contact rate over time (contacts/person-year).
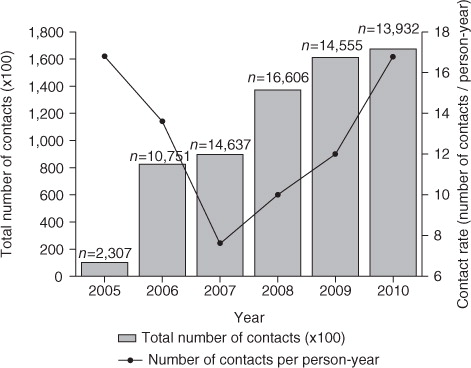
Table 3. Programme contacts over time
Violence redressal
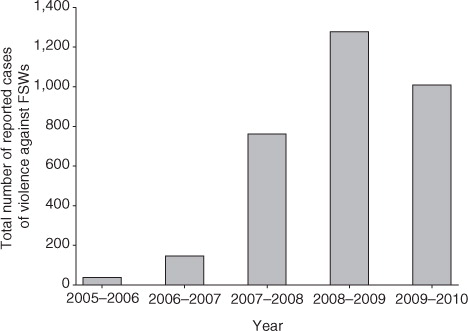
During the period 2005–2010, Swathi Nyaya Sanjeevani dealt with a total of 3,242 reported cases related to violence against FSWs in Bangalore. The annual number of reported cases increased from 40 cases in 2005–2006; 148 cases in 2006–2007; 763 cases in 2007–2008; 1280 cases in 2008–2009; to 1011 cases in 2009–2010 (). The reporting period was 1 April–30 March of the next year. In most cases, a response was initiated within 24 hours. The majority of the reports were related to violence by the police (37%). The other major perpetrators were partners (14%), other FSWs (12%), and husbands (9%).
Fig. 3. Reported cases of violence against FSWs per year (2005–2010). Bars represent the total number of reported cases of violence against FSWs per year. Reporting period was 1 April–30 March of the next year.
Alcohol de-addiction
During a period of 5 years (April 2005–March 2010), 1,377 FSWs were identified and referred for alcohol de-addiction. Of those women, 433 underwent treatment. The participation in the alcohol de-addiction programme increased from 0 women in 2005–2006; 21 women in 2006–2007; 110 women in 2007–2008; 71 women in 2008–2009; to 231 women in 2009–2010 (reporting period was 1 April–30 March of the next year).
Microfinance
There were in total 3,053 FSWs who joined as shareholders of the cooperative bank during 2007–2010. More than half of them (52%; 1578 individuals) opened savings accounts. The number of women who opened a savings account increased from 488 women in 2007–2008; 501 women in 2008–2009; to 589 women in 2009–2010 (reporting period was 1 April–30 March the next year). Over 1,700 women opened recurrent deposit accounts. Total savings through various schemes of the bank during 2007–2010 accumulated to 2.2 million rupees (approximately 38,500 USD). The total amount of loans that were distributed to 406 women equalled 4.5 million rupees (approximately 79,000 USD).
Condom distribution
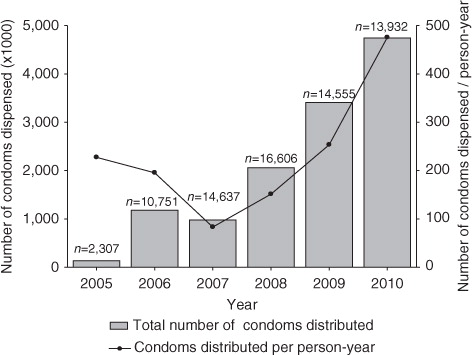
The number of distributed condoms increased sharply between 2005 and 2010, with 140,248 condoms distributed in 2005 to 4,748,943 condoms distributed in 2010 (). Additionally, the number of condoms distributed per person-year also increased over time, from 227 condoms/person-year in 2005 to 475 condoms/person-year in 2010 (). In 2010, across four zones, 285 condom outlets catered to the requirement of women in sex work.
Fig. 4. Condoms distributed per year (2005–2010). Bars represent the total number of distributed condoms per year. Line represents the number of condoms distributed per person-year.
Sexually transmitted infections
Overall, there were 53,762 episodes of STIs recorded between 2005 and 2010, for 14,162 individual FSWs. This resulted in a mean STI incidence rate of 0.97 STIs/person-year (). The most frequently diagnosed STIs were cervicitis (50.6% of the total STIs) and vaginitis (41.4%) ().
Fig. 5. Diagnosed STIs and STI incidence rate over time. Bars represent the total number of diagnosed STIs per year. Line represents the STI incidence rate over time (STI/person-year).
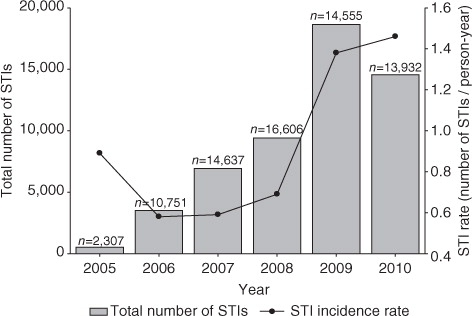
Table 4. Number of diagnosed STIs over time
STI treatment
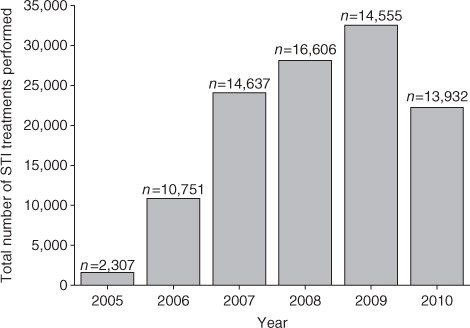
The distribution of treatment ‘packs’ for the diagnosed STIs increased over time () from 1,638 distributed packs in 2005 to 22,283 packs in 2010.
Fig. 6. Distributed STI treatment packages over time. Bars represent the total number of STI treatment packages that were distributed per year.
Cost efficiency
The Pragati programme through effective leveraging of resources, partnerships, and achieving scale has been cost-efficient. The programme cost per participating sex worker per year of Pragati during 2005–2010 was approximately INR 2,017 (US$38), which is comparable to INR 2,000 (U$38) per sex worker as prescribed by the guidelines of NACO Citation10. However, the targeted interventions among FSWs under the national programme were HIV prevention centric with limited efforts towards violence reduction and collectivisation. Pragati, at similar costs, offered a more comprehensive set of HIV vulnerability reduction activities such as services (i.e. microfinance, violence redressal and reduction); anti-trafficking activities; social protection; alcohol de-addiction; individual, group, and institutional capacity building. More importantly, the cost per participating sex worker in the Pragati declined between 2005 and 2010 as the programme's scale increased: the cost per participating sex worker (reporting period 1 April–30 March of the next year) was INR 2,992 (US$56) in 2005–2006; INR 2,142 (US$40) in 2006–2007; INR 2,429 (US$46) in 2007–2008; INR 1,672 (US$32) in 2008–2009; and INR 1,628 (US$31) in 2009–2010.
Discussion
Overall, this study has shown that the Pragati programme has had a beneficial effect on the lives and livelihoods of the 20,330 participating FSWs in Bangalore, India. Between 2005 and 2010, the number of women who received help from a crisis-response team increased, more women participated in alcohol de-addiction programmes, and the number of saving accounts and distributed microfinance loans was expanded. Furthermore, condom use increased over time, and more FSWs were treated for STIs. In contrast to these findings, the number of STIs and the STI incidence rate increased over time.
There have been several studies that indicate the disproportionate burden of HIV in FSWs compared to other women Citation11, and these studies have investigated the effectiveness of different intervention programmes Citation12 Citation13. However, to our knowledge, this study is the first showing longitudinal follow-up in a large group of FSWs in India and reporting data of the empowering strategy on such a wide range of social, economic, and health-related variables. Previous studies that analysed the effect of behavioural interventions on STIs primarily focussed on interventions to change sexual behaviour, promote condom use, and educate about effective management of STIs Citation14 Citation15. Although these interventions appeared to be effective in reducing STI prevalence and incidence, it was also suggested to further explore other, more potent behavioural change strategies that might show even more favourable results Citation13–Citation16.
Study limitations
The present study has limitations. First, the Pragati programme is an observational registration of 20,330 FSWs in four zones of Bangalore. Components of the programme were developed and ranked in priority in discussion with the participants. As such, different components were implemented while the programme was on-going, based on the needs of the women. This could complicate the analyses of the effectiveness of these components in the 1st years of the enrolment of the programme. Second, STIs were diagnosed according to syndromic case management. Therefore, trends in specific causes of STIs are unavailable. However, syndromic case management is more accurate than diagnosis based on clinical judgment alone, even in experienced hands, and more cost-effective for some syndromes than the use of laboratory tests Citation7. A major advantage of syndromic case management in populations such as FSWs is that with the use of flowcharts to guide toward diagnosis, treatment can be provided immediately at first contact, thereby reducing secondary cases and infectiousness Citation17. Although it has been shown that there is a wide variation between self-reporting of morbidity and syndromic- and aetiology-based diagnosis of STIs Citation18, syndromic case management remains the best available option in low-income settings when diagnostic testing facilities are unavailable for high-risk populations like FSWs. Finally, it would have been interesting to analyse the proportion of FSWs who had been able to create options for an alternative livelihood and leave the commercial sex-work business, as a result of participation in the Pragati programme. Unfortunately, no follow-up data were available for FSWs who had left the programme.
Interpretation of the results
How can our results be explained? Most findings of the present analysis are in line with the increased empowerment of the participating FSWs. First, the number of contacts with the programme increased over time, suggesting social empowerment of the participating women. In the first 3 years (2005–2007), a decrease in the contact rate was seen, which was followed by an increase in the last years of the study period (2007–2010). A possible explanation is that the FSWs who were enrolled in the programme in the first years were a motivated selection of all 20,330 participating FSWs and had an above average number of programme contacts. The relatively small number of FSWs who were present in the programme in 2005 (n=2,307) and 2006 (n = 10,751) could have resulted in an inflated contact rate in these years. From 2007 onwards, the annual number of participating FSWs was on average about 15,000 and the contact rate showed a steady increase from that moment onwards. Second, the FSWs in Pragati increasingly used the available crisis-response mechanism and the violence watch committees between 2005 and 2010, which shows the need for these facilities. Third, the alcohol de-addiction programme showed a sharp increase in participating women within the study period. In the absence of success rates of the de-addiction programme, we still may assume that it has most likely improved the social as well as economic functionality of the women who successfully completed the treatment. Not only has it helped the women to overcome their addiction, a supplementary effect is that this has probably reduced their odds of exposure to HIV infection by ensuring correct and consistent condom use during sex. Unfortunately, no follow-up data were available on the sustainable effects of the de-addiction programme, which complicates the interpretation of these findings. Fourth, the microfinance mechanism has helped over 1,500 women in sex work to open a savings or deposit account during the study period, which helped to provide greater financial security. Fifth, the condom distribution showed a steady increase during the study period, which could be an example of a favourable change in sexual behaviour of the FSWs. Finally, the STI incidence rate that was seen between 2005 and 2010 seems to imply a reverse effect of the programme efforts. Our hypothesis is that that the increase in episodes of STI is not a ‘true’ increase in incidence of STI episodes but rather a consequence of detection bias: the enhanced empowerment with more regular check-ups in the clinic allowed more timely diagnosis of STIs at a less severe stage. This presumed decrease in the under-diagnosis and under-treatment of STIs could be overshadowed by the findings on the increasing STI incidence rate, but could well be another achievement of the programme. It will be interesting to see if the trend reverses in future analyses of the programme, as other studies imply that a longer follow-up period is needed Citation4 Citation19 Citation20. Although the presented data indicate that the Pragati programme has succeeded in establishing a multifaceted empowering programme for FSWs, additional analyses focussed on the effectiveness of the discrete programme activities on outcome measurements are necessary to further clarify their role in improving the well-being of the participating FSWs. Furthermore, it might be interesting to evaluate if certain subgroups of FSWs are differentially susceptible for the effects of the Pragati activities.
Conclusion
In conclusion, our results show that a programme focused on social and economic empowerment among FSWs, combined with medical treatment, is successful in reaching and involving the target population. Women frequently used the facilities offered in drop-in centres and clinics involved in the programme. Future studies and analyses should focus on the evaluation of different aspects of empowerment programmes and the effects.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Acknowledgements
We are very grateful to and thank all of the female sex workers for participating in the Pragati project. We are very grateful to Benoy Peter, Coordinator, Knowledge Management and Policy Shaping, Swasti Health Resource Centre, for his assistance. Pragati is being implemented as a partnership between Swathi Mahila Sanga, a community-based organisation of women in sex work; Swasti, a health resource centre that focuses on the social and management dimensions in the health sector, and the Karnataka Health Promotion Trust, an implementation and funding agency. The Pragati project is funded by the Bill and Melinda Gates Foundation – Avahan's Sankalp programme. We thank all these organisations for their contribution to the Pragati project and this paper.
Notes
1Meaning ‘progress’ (in Kannada – an Indian language)
Related Research Data
References
- National AIDS Control Organisation, Ministry of Health and Family Welfare Government of India. (2011). Annual Report 2009–2010. Available from: http://www.nacoonline.org [cited 7 May 2012]..
- Kumar R, Mehendale SM, Panda S, Venkatesh S, Lakshmi PVM, Kaur M, et al.. Impact of targeted interventions on heterosexual transmission of HIV in India. BMC Public Health. 2011; 11: 549.10.3402/gha.v5i0.19279.
- Gutierrez JP, PcPherson S, Fakoya A, Matheou, Bertozzi SM. Community-based prevention leads to an increase in condom use and a reduction in sexually transmitted infections (STIs) among men who have sex with men (MSM) and female sex workers (FSW): the Frontiers Prevention Project (FPP) evaluation results. BMC Public Health. 2010; 10: 497.10.3402/gha.v5i0.19279.
- Ng M, Gakidou E, Levin-Rector A, Khera A, Murray CJ, Dandona L. Assessment of population-level effect of Avahan, an HIV-prevention initiative in India. Lancet. 2011; 378: 1643–52. 10.3402/gha.v5i0.19279.
- Census of India, provisional population totals. (2011). Available from: http://censusindia.gov.in/2011census/censusinfodashboard/index.html. [cited 7 May 2012]..
- Batliwala S. The meaning of women's empowerment: new concepts from action. In: Sen G, Germaine A, Chen LC, Population policies reconsidered: health, empowerment and rights. Harvard MA: Harvard Center for Population and Development Studies. 1994, pp. 76–88.
- WHO. (2003). Guidelines for the management of sexually transmitted infections. NLM classification WC. 142, 1–91. Publisher: WHO, Geneva.
- National AIDS Control Organization, Ministry of Health and Family Welfare Government of India. (2011). National guidelines on prevention, management and control of reproductive tract infections including sexually transmitted infections. 1–87. 2007. Available from: http://www.nacoonline.org [cited 7 May 2012].
- National AIDS Control Organization, Ministry of Health and Family Welfare Government of India. (2011). Operational guidelines for programme managers and service providers for strengthening STI/RTI services. 1–94. 2007. Available from: http://www.nacoonline.org [cited 7 May 2012]..
- National AIDS Control Organization, Ministry of Health and Family Welfare Government of India. (2011). Targeted Interventions under NACP III Operational guidelines Volume 1, Core high risk groups. 2007. Available from: http://www.nacoonline.org [cited 26 September 2012]..
- Baral S, Beyrer C, Muessig K, Poteat T, Wirtz AL, Decker MR, et al.. Burden of HIV among female sex workers on low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2012; 12: 538–49. 10.3402/gha.v5i0.19279.
- Dandona R, Dandona L, Gutierrez JP, Kumar AG, McPherson S, Samuels F, et al.. ASCI FPP Study Team. High risk of HIV in non-brothel based female sex workers in India. BMC Public Health. 2005; 5: 87.10.3402/gha.v5i0.19279.
- Mayaud P, Mabey D. Approaches to the control of sexually transmitted infections in developing countries: old problems and modern challenges. Sex Transm Infect. 2004; 80: 174–82. 10.3402/gha.v5i0.19279.
- Reza-Paul S, Beattie T, Syed HU, Venukumar KT, Venugopal MS, Fathima MP, et al.. Declines in risk behaviour and sexually transmitted infection prevalence following a community-led HIV preventive intervention among female sex workers in Mysore, India. AIDS. 2008; 22(Suppl. 5):S91–100. 10.3402/gha.v5i0.19279.
- Wariki WM, Ota E, Mori R, Koyanagi A, Hori N, Shibuya K. Behavioral interventions to reduce the transmission of HIV infection among sex workers and their clients in low- and middle-income countries. Cochrane Database Syst Rev. 2012; 2: CD005272.
- Gangopadhyay DN, Chanda M, Sarkar K, Niyogi SK, Chakraborty S, Saha MK, et al.. Evaluation of sexually transmitted diseases/human immunodeficiency virus intervention programs for sex workers in Calcutta, India. Sex Transm Dis. 2005; 32: 680–4. 10.3402/gha.v5i0.19279.
- Amin AR. Enhanced syndromic case management of reproductive tract infection/sexually transmitted infection cases as per National AIDS Control Organization guidelines. Indian J Sex Transm Dis and AIDS. 2010; 31: 61–2. 10.3402/gha.v5i0.19279.
- Ray K, Muralidhar S, Bala M, Kumari M, Salhan S, Gupta SM, et al.. Comparative study of syndromic and etiological diagnosis of reproductive tract infections/sexually transmitted infections in women in Delhi. Int J Infect Dis. 2009; 13: e352–9. 10.3402/gha.v5i0.19279.
- Jana S, Basu I, Rotheram-Borus MJ, Newman PA. The Sonagachi project: a sustainable community intervention programme. AIDS Educ Prev. 2004; 16: 405–14. 10.3402/gha.v5i0.19279.
- Williams JR, Foss AM, Vickerman P, Watts C, Ramesh BM, Reza-Paul S, et al.. What is the achievable effectiveness of the India AIDS Initiative intervention among female sex workers under target coverage? Model projections from Southern India. Sex Transm Infect. 2006; 82: 372–80. 10.3402/gha.v5i0.19279.