
Abstract
Background
Cash transfers (CTs) are increasingly used as a strategy to alleviate poverty and improve child health outcomes in low- and middle-income countries. The Child Support Grant (CSG) is the largest CT programme in South Africa, and on the continent, targeting poor children from birth until the age of 18 with a monthly sum of R300 (USD30). Evidence on the CSG shows that early receipt of the grant is associated with improved child health outcomes. Since its implementation, one of the major concerns about the grant has been take-up rates, particularly for younger children. This paper reports results on take-up rates for 12-week-old infants residing in an urban township in South Africa.
Methods
This is a descriptive study utilising data from a community-based, cluster-randomised trial which evaluated a programme providing pregnancy and post-natal home visits by community health workers to 3,494 mothers in Umlazi township, South Africa.
Results
At the 12-week visit, half (52%) of the mothers who had enrolled in the study had applied for the CSG on behalf of their children, while 85% of the mothers who had not applied were still planning to apply. Only 38% (1,327) of all children had received the CSG.
Conclusions
In this study, many mothers had not applied for the CSG in the first few months after delivery, and only a third of children had accessed the grant. Further research is needed to understand what the current barriers are that prevent mothers from applying for this important form of social protection in the early months after delivery.
In recent years, cash transfer (CT) programmes have become popular policy instruments for reducing child poverty and improving a range of child health outcomes in low- and middle-income countries (Citation1–Citation3). Such CT programmes can take the form of conditional or unconditional cash grants, can be means-tested, and targeted or universal (Citation4, Citation5). Over the past decade, a strong evidence base has been built in low- and middle-income countries to show that CTs, even if transferring small amounts of money to poor children, can have a positive impact on child growth and nutritional status (Citation6–Citation8), school attendance and educational attainment (Citation9, Citation10), reduce child hunger, and reduce risky sexual behaviours amongst adolescent children (Citation11–Citation13). This strong evidence base has increased the urgency and call for countries to expand child-focused CT programmes, and, where take-up is low, to accelerate it.
In South Africa, the Child Support Grant (CSG) is the largest CT programme in the country and on the continent. It targets children from poor households who receive about USD30 per month from birth until the age of 18. To qualify for the grant, caregivers of CSG applicants have to earn less than 10 times the amount of the CSG (currently this amounts to <R3600 per year or <USD360 per year for single caregivers, and <R7200 per year or <USD720 per year for married or cohabiting couples) (Citation14).
Since its implementation, one of the major concerns about the CSG has been take-up rates, particularly for younger children (Citation15–Citation17). More recent evidence has reported take-up rates of about 60% for children under 2 years (Citation9, Citation17), and even lower take-up rates for children under 6 months (Citation17). Children who receive the CSG early after birth have been shown to achieve better growth (height-for-age) and nutritional status than children who receive it later (Citation7).
Methods
This paper reports results on CSG access, reasons for non-application and non-receipt among caregivers of 12-week-old children in Umlazi, a large urban township in Durban, South Africa. The study utilised data from a community-based, cluster-randomised trial which evaluated a programme providing pregnancy and post-natal home visits by community health workers (CHWs) to encourage exclusive breastfeeding (Citation18). In the control arm, mothers received home visits (one antenatal and two post-natal) from CHWs who advised them on the process of applying for a CSG; however, the CHW visits in the control arm had no effect on grant uptake at 12 weeks (relative risk 0.97; 95% CI: 0.90–1.03). Details of the trial are published elsewhere (Citation18, Citation19).
The main outcomes of the trial were measured at 12 weeks. Questions related to the CSG were included in the questionnaire with self-reported responses regarding whether a mother had applied for the CSG, whether they were intending to apply, and reasons for not applying. To apply for the CSG, a mother or primary caregiver of the child for whom the grant is sought needs to have the following documents: an identity document (ID) for the mother or primary caregiver, birth certificate of the child, and proof of income (or an affidavit confirming unemployment).
Ethical considerations
The analysis of CSG take-up was included in the trial protocol submitted for ethical approval. The Medical Research Council ethics review board (EC08-002) approved the trial study. A Community Advisory Board (CAB), consisting of local stakeholders, was established and acted as a liaison between the community and research staff.
Results
Application for receipt of the CSG
presents data on indicators of CSG application and receipt. Among the 3,494 children whose caregivers were interviewed at 12 weeks, 1,828 (52%) had applied for the CSG. A large proportion of mothers did have the required documents needed for the application with 86% of mothers possessing an ID book and 73% of infants having a birth certificate. Amongst mothers who had not applied, 1,415 (85%) reported that they still intended to apply for the grant. Reasons for not applying for the CSG ranged from not possessing an ID document (161/251, 64%), to not qualifying for the CSG because of reported financial status that mothers perceived to be higher than the official means-tested threshold (54/251, 21%). Given the importance of early receipt, it is concerning that almost half (48%) of the mothers in this study had still not applied for the grant 3 months after giving birth.
Fig. 1 CSG application and reasons for not applying.
*Five mothers gave more than one reason for not applying.
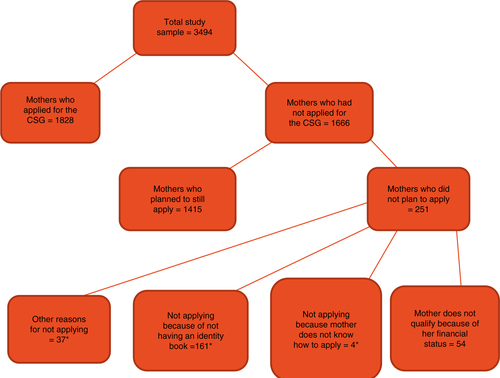
Very few mothers attributed not applying for the CSG to lack of knowledge about the application process (4/251, 1.5%). These results are encouraging as they are in sharp contrast to the situation in the early years after the CSG was implemented, where many eligible caregivers did not apply for the CSG because they did not know what the process entailed (Citation15, Citation20), and where not possessing a birth certificate was one of the major administrative barriers to CSG receipt (Citation17).
CSG receipt
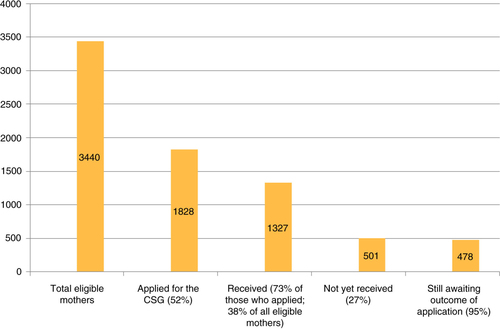
Of the 1,828 children who applied for the CSG, 1,327 (73%) had received it at 12 weeks. However, in the total sample only 38% were in receipt of the grant (). Among the 501 non-recipients, 478 (95%) were not in receipt of the CSG at 12 weeks because they were still waiting for their applications to be processed. The turn-around time for CSG receipt is 21 working days after an application has been submitted, and thus a number of these applicants could have still been within that window period.
Fig. 2 Cascade showing CSG receipt at 12 weeks post-delivery.
Conclusion
While knowledge about the CSG application process seems to have improved since the early years of the grant's implementation, this study has shown that overall only 38% of children, the great majority of whom are likely to have been eligible for the CSG, were in receipt of the grant by 12 weeks of age, despite the majority of mothers possessing the administrative requirements (ID book and birth certificate). From these results, it is clear that the major reason for low receipt in this group of infants is that mothers initiate application for the CSG late. Further qualitative research is needed to understand what the current barriers are that prevent mothers from applying for this important form of social protection in the early months after delivery.
Conflict of interest and funding
The authors declare that they have no competing interests. The research study component was funded through a grant to Save the Children's Saving Newborn Lives programme, from the Bill & Melinda Gates Foundation. TD, DS, and DJ are also supported by the South African National Research Foundation.
References
- Paes-Sousa R, Santos LM, Miazaki ES. Effects of a conditional cash transfer programme on child nutrition in Brazil. Bull World Health Organ. 2011; 89: 496–503. [PubMed Abstract] [PubMed CentralFull Text].
- Samson M, van Niekerk I, Mac Quene K. Designing and implementing social transfer programmes. 2006; Cape Town: EPRI.
- Soares S, Osório G, Soares R, Veras F, Medeiros M, Zepeda E. Conditional cash transfers in Brazil, Chile and Mexico: impacts upon inequality. 2007; New York: United Nations Development Program.
- Van Oorschot W. Ben-Arieh A, Gal J. Troublesome targeting: on the multilevel causes of nontake-up. Into the promised land: issues facing the welfare state. 2001; Westport, CT: Preager. 239–56.
- Barrientos A. Conditions in antipoverty programmes. J Poverty Soc Justice. 2011; 19: 15–26.
- Duflo E. The effects of old age pension on child health in South Africa. 1999; Cambridge: Massachusetts Institute of Technology.
- Aguero JM, Carter MR, Woolard I. The impact of unconditional cash transfers on nutrition: the South African Child Support Grant. 2006; Washington, DC: Centre for Global Development.
- Fernald LC, Gertler PJ, Neufeld LM. Role of cash in conditional cash transfer programmes for child health, growth, and development: an analysis of Mexico's oportunidades. Lancet. 2008; 371: 828–37. [PubMed Abstract] [PubMed CentralFull Text].
- DSD, SASSA, UNICEF. The South African Child Support Grant Impact Assessment: evidence from a survey of children, adolescents and their households. 2011; Pretoria: UNICEF South Africa.
- Gertler P. Mexico's PROGRESA: using a conditional cash transfer to invest in human capital. 2003. Available from: http://www.sarpn.org/documents/d0001083/P1196-Gertler_Mexico_Presentation.pdf .
- Cluver L, Boyes M, Orkin M, Pantelic M, Molwena T, Sherr L. Child-focused state cash transfers and adolescent HIV-infection risks: a prospective multi-site study in South Africa. Lancet Glob Health. 2013; 1: 362–70.
- Baird S, Garfein RS, McIntosh CT, Özler B. Effect of a cash transfer programme for schooling on prevalence of HIV and herpes simplex type 2 in Malawi: a cluster randomised trial. Lancet. 2012; 379: 1320–9. [PubMed Abstract].
- De Walque D, Dow WH, Nathan R, Abdul R, Abilahi F, Gong E, etal. Incentivising safe sex: a randomised trial of conditional cash transfers for HIV and sexually transmitted infection prevention in rural Tanzania. BMJ open. 2012; 2: e000747. [PubMed Abstract] [PubMed CentralFull Text].
- SASSA. Your Grants 2013/2014. Pretoria: Development DoS. Available from: http://www.sassa.gov.za/index.php/knowledge-centre/grant-booklets .
- Kola S, Braehmer S, Kanyane M, Morake R, Kimmie Z. Phasing in the Child Support Grant: a social impact study. 2000; Johannesburg: Community Agency for Social Enquiry.
- Noble M, Wright G, Barnes H, Noble S, Ntshongwana P, Gutierrez-Romere R. The Child Support Grant: a sub-provincial analysis of eligibility and take up in January 2005. 2005; Pretoria,: Republic of South Africa: Department of Social Development.
- Zembe-Mkabile W, Doherty T, Sanders D, Jackson D, Chopra M, Swanevelder S, etal. Why do families still not receive the child support grant in South Africa? A longitudinal analysis of a cohort of families across South Africa. BMC Int Health Hum Rights. 2012; 12: 24. [PubMed Abstract] [PubMed CentralFull Text].
- Tomlinson M, Doherty T, Ijumba P, Jackson D, Lawn J, Persson LÅ, etal. Goodstart: a cluster randomised effectiveness trial of an integrated, community-based package for maternal and newborn care, with prevention of mother-to-child transmission of HIV in a South African township. Trop Med Int Health. 2014; 19: 256–66. [PubMed Abstract].
- Tomlinson M, Doherty T, Jackson D, Lawn JE, Ijumba P, Colvin M, etal. An effectiveness study of an integrated, community-based package for maternal, newborn, child and HIV care in South Africa: study protocol for a randomized controlled trial. Trials. 2011; 12: 236. [PubMed Abstract] [PubMed CentralFull Text].
- Sogaula N, Jackson D, McCoy D, Karaolis N, Sanders D, Chopra D. Child health care: what's the point when there is no food at home?. 2001. South Africa: Children First.