
Abstract
Background
Nationally representative evidence on the burden and determinants of disability among older people in sub-Saharan Africa in general, and Uganda in particular, is limited.
Objective
The aim of this study was to estimate the prevalence and investigate the correlates of disability among older people in Uganda.
Design
We conducted secondary analysis of data from a sample of 2,382 older persons from the Uganda National Household Survey. Disability was operationalized as either: 1) having a lot of difficulty on any one question; 2) being unable to perform on any one question; or, 3) having some difficulty with two of the six domains. We used frequency distributions for description, chi-square tests for initial associations, and multivariable logistic regressions to assess the associations.
Results
A third of the older population was disabled. Among all older persons, disability was associated with advancement in age (OR=4.91, 95% CI: 3.38–7.13), rural residence (0.56, 0.37–0.85), living alone (1.56, 1.07–2.27), separated or divorced (1.96, 1.31–2.94) or widowed (1.86, 1.32–2.61) marital status, households’ dependence on remittances (1.48, 1.10–1.98), ill health (2.48, 1.95–3.15), and non-communicable diseases (NCDs) (1.81, 0.80–2.33). Gender was not associated with disability among older persons.
Conclusions
Disability was associated with advancement in age, rural residence, living alone, divorced/separated/widowed marital status, dependence on remittances, ill health, and NCDs. Interventions to improve health and functioning of older people need to focus on addressing social inequalities and on the early preventive interventions and management of NCDs in old age in Uganda.
Population ageing is a global phenomenon affecting both developed and developing countries with several implications. First, there is a rise in the prevalence of non-communicable diseases (NCDs) (Citation1–Citation3). Second, a double burden of diseases among older people in Africa, from infectious diseases of poverty and NCDs (Citation4). Third, disability among older persons, which is becoming an important area for research in developing countries (Citation5, Citation6).
Disability refers to the negative aspects of the interaction between an individual's health condition and his or her contextual factors and environmental factors. It implies having difficulties with activities of daily living (ADL) and instrumental activities of daily living (IADL), and mobility limitations (Citation1, Citation7). The Washington Group defined disability as having at least a severe difficulty or being unable to perform on any key ADL: sight, hearing, walking or climbing, and remembering or concentrating (Citation8, Citation9). Broadly, disability negatively affects health, wellbeing, physical functioning, and leads to social exclusion and limited access to healthcare among older people (Citation5, Citation10) (Citation11).
Globally, disability affects over 1 billion people (Citation12). A multi-country study covering 54 countries using World Health survey data estimated disability at 15% and higher in developing than developed countries (Citation13). In Uganda, the population of older persons increased from 1.1 million in 2002 to 1.3 million in 2010 (Citation14) and is expected to increase from 1.6 million in 2014 to 5.5 million by 2050 (Citation15). According to the 2011 Uganda Demographic and Health Survey (UDHS), the national prevalence of disability in Uganda was 19% (Citation16).
Disability among older people is associated with demographic, socio-economic, and health factors (Citation3, Citation10) (Citation17, Citation18). Female gender was associated with disability, where older women were at a higher risk of disability than their male counterparts (Citation3, Citation10) (Citation17, Citation18). Female gender was associated with disability in Malawi (Citation19), South Africa (Citation20), China (Citation21), and other developing countries (Citation1, Citation22–Citation24), as well as in the USA (Citation11). Hosseinpoor et al. (Citation24) attributed the gender differentials in disability to socio-economic inequalities between men and women. However, the 90+ Study in Southern California found no relationship between gender and disabilities (Citation25). Advancement in age increases the risk of disability among older people (Citation10, Citation25) in Nigeria (Citation17), Malaysia (Citation22), Singapore (Citation23), South Africa (Citation26), India (Citation27), Tanzania (Citation18), and in the USA (Citation11).
Rural residence has been found to reduce the risk of disabilities among older persons (Citation28) except in China (Citation21). The prevalence of disability has been reported to be higher among older persons who were not in union (single, divorced, or separated) compared to those who were married (Citation29) in China (Citation21), South Africa (Citation26), India (Citation27), and Uganda (Citation30).
Living alone is associated with health and disability status. In China, older persons who lived alone had poor health status including disability. Those who lived with others are supported emotionally and materially according to the social support theory (Citation29). Poverty status predisposes older persons to the risk of disability (Citation3), especially older women (Citation28) for both developed and developing countries. Poor socio-economic status was a risk factor for disability in the Netherlands (Citation31), Brazil (Citation1), Tanzania (Citation32), and Ghana (Citation33). Lack of/low education level of older persons was associated with disability (Citation1, Citation10) (Citation28). However, some studies have found no relationship between education and disability (Citation3).
NCDs (e.g., diabetes, stroke, arthritis, and heart disease) are a major underlying cause of disabilities (Citation34). Studies have reported strong associations between NCDs (Citation17, Citation22) (Citation23, Citation35), depressive symptoms and dementia (Citation2, Citation22), stroke (Citation36), diabetes, and disability among older persons (Citation7).
There is limited research on the prevalence and correlates of disability using nationally representative samples among older persons in Africa in general, and Uganda in particular. Available scientific evidence is from World Health Organization (WHO) Study on global AGEing and adult health, Social Assistance Grants for Empowerment (SAGE) (Citation20, Citation37), or the INDEPTH network data (Citation20). However, many of these studies have not used nationally representative samples. For instance, in Tanzania, a community-based study of the Hai area estimated disability at 6% (Citation18). The few studies that investigated the prevalence and correlates of disabilities among older population in Uganda focused on HIV contexts rather than the general population (Citation30, Citation37). The aim of this paper was to determine the prevalence and correlates of disabilities in the older population in Uganda, using a nationally representative sample from the 2010 Uganda National Household Survey (UNHS) data.
Methods
Data
The study used the 2010 UNHS data. The UNHS used a two-stage stratified sampling. At the first stage, 712 enumeration areas were drawn using probability proportional to size. At the second stage, households were drawn using systematic sampling. A total of 6,800 households were interviewed in the survey (Citation14). Older persons were selected from the sample using the variable age. Persons aged 50 years and older were selected for further analysis, forming a sample of 2,628 older persons. The decision to select persons aged 50 years and above was based on the fact that several studies using WHO and INDEPTH network data define older persons starting at age 50 for African contexts (Citation27, Citation32) (Citation38, Citation39).
Explanatory variables
The UNHS data covered individual and household characteristics – demographic and socio-economic characteristics, disability, health, and housing conditions. Demographic factors included gender (male or female), age group, region, place of residence (rural or urban), living arrangement, relationship to household head, and marital status. Age was recoded into four age categories: 50–59, 60–69, 70–79, and 80+. Region had four categories (1=central, 2=eastern, 3=northern, and 4=western). Living arrangements were recoded into two categories (living alone or with others). Relationship to household head was recoded into three categories (1=head, 2=spouse, and 3=relative). Marital status was recoded into three categories (1=married, 2=separated or divorced or never married, and 3=widowed). Three never married older persons were merged with the separated and divorced category in the data because they were very few.
Socio-economic factors included education level, religion, household poverty status, household major source of earnings, learning technical skill, and ownership of bicycle. Education level was recoded into no education, primary and secondary, or higher education. Religion was recoded into Catholic, Anglican, Muslim, Pentecostal, Seventh Day Adventists, and others. Household poverty status was generated from household expenditures and recoded 1=poor if a household spent less than $1 a day and 0=not poor, if a household spent greater than $1 a day. Household major source of earnings was recoded into farming, wages, and remittances. Learning a technical skill and household bicycle ownership were binary (0=no, 1=yes).
Health-related information was collected on illnesses in the past 30 days preceding the survey, disability, self-reported NCDs (Citation14). Ill health was a binary variable (0=not sick, 1=sick). Self-reporting of diabetes, heart disease, and high blood pressure were used to estimate the prevalence of NCDs, recoded as binary variable (Citation14).
Outcome variable
Disability was measured by asking six questions on functional limitations on both ADLs and IADLs. ADLs, which mainly focused on body impairments included difficulties in seeing, hearing, walking, and concentrating or remembering. IADLs, which relate to personal care, were measured using difficulties with washing or bathing, feeding, dressing, and toileting as shown below.
Do you have difficulty seeing, even if he/she is wearing glasses?
Do you have difficulty hearing, even if he/she is wearing a hearing aid?
Do you have difficulty walking or climbing steps?
Do you have difficulty remembering or concentrating?
Do you have difficulty (with self-care such as) washing all over or dressing, feeding and toileting?
Do you have difficulty communicating (e.g. understanding others or others understanding him/her) because of a physical, mental, or emotional health condition?
These six questions were originally coded into five categories (1=No, no difficulty, 2=Yes – some difficulty, 3=Yes – a lot of difficulty, 4=cannot perform at all, and 8=don't know). Among the older persons, there was only one ‘don't know’ response on sight disability.
Disability or being disabled was operationalized as either 1) having a lot of difficulty on any of the six indicators; 2) being unable to perform at all on any of the six indicators; or 3) having some difficulty with at least two of the six indicators. This approach to measuring disability has been used in other studies (Citation8, Citation9) (Citation13). Using these three aspects is better than using ‘having some difficulty on any indicator’ to measure disability (Citation40).
Statistical analyses were done in STATA version 12. In the first place, descriptive statistics (frequency and percent distributions) were analyzed to describe the sample. Second, statistical tests of associations between socio-economic, demographic, and health factors and disability were performed using chi-square tests. The level of statistical significance was set at 95% confidence interval (p=0.05). Finally, a full binary logistic regression model was done to predict the correlates of disability among older population in Uganda. Regression diagnostics included a link test and goodness of fit test.
Results
Descriptive characteristics of older persons
presents the descriptive characteristics of older persons stratified by gender. Overall, there was a higher percentage of older women than older men in the sample. The majority of the older men and women were aged 50–59 years and were from the eastern region. However, the proportion of older women was slightly higher than that of older men as age increased. Nine out of ten older men and women in the sample resided in rural areas and were not living alone. A higher percentage of men than women were household heads and were married.
Table 1 Distribution of older persons by demographic, socio-economics, health factors and disability, stratified by gender in Uganda
Older men were better off in terms of education levels than older women. The majority of the older men and women were Catholics and were from non-poor households – spent >$1 a day. A higher proportion of older men than women depended on farming and wages. However, a higher proportion of older women than men depended on remittances. An approximately similar proportion of one in five older men and women had learnt a technical skill or trade. More older men's households than women owned bicycles.
Overall, more than half (62%) were sick, with a higher proportion of women than men reporting having an illness in the last 30 days. About two in ten sampled reported at least one NCD (diabetes, heart disease, and high blood pressure) and a third had a disability. Similarly, a higher proportion of women than men reported having an NCD or a disability.
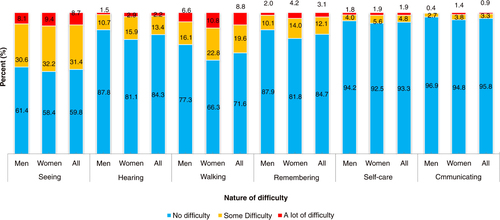
presents a detailed description of the type and severity of disability among older persons stratified by gender. Sight problem was the leading form of disability followed by walking or climbing difficulties, hearing, and concentrating or remembering difficulties (15%). Self-care and communication challenges were less common among the older population. Another striking feature from is that older women reported higher prevalence of either some or a lot of difficulty on all of the six domains represented.
Fig. 1 Nature and severity of disability among older people in Uganda.
Association between disability and demographic and socio-economic factors
also presents chi-square test results for assessment of associations between disability and socio-economic, demographic and health factors. Of all the variables, region, religion, and poverty status were not significantly associated with disability.
Among all older persons, the prevalence of disability was highest among women, oldest old – age 80+, rural residents, those living alone, and those widowed. In addition, disability was highest among those who depended on remittances, learnt technical skill, did not own a bicycle, and reported illness and an NCD.
The same pattern for the prevalence of disability was maintained among older men and women alone, except that the latter showed higher prevalence than the former on various demographic and socio-economic variables (). The prevalence of disability was higher among older women than men for the oldest old – 80+, rural residents, those living alone and the widowed. In addition, disability was higher among older women than men for those who reported having an illness in last 30 days and an NCD.
Multivariate results
presents the results of multivariable logistic regression of factors associated with disability among older persons stratified by gender. The risk of disability consistently increased with advancement in age for all older persons. Those aged 60–69; 70–79 and 80+ had increased odds of disability compared to those aged 50–59 years. Urban older persons were less likely to be disabled compared to rural older people. This pattern was the same for older women but not older men.
Table 2 Results of multivariable logistic regression of disability on socio-economic, demographic, and health-related factors among older people in Uganda
Similarly, all older persons who lived alone compared to those who lived with other people, were more likely to report disability. Living arrangement did not have a significant association among older men and women alone.
A significant relationship existed between marital status and disability for all older persons and had different directions for older men and women. Older people, who were divorced/separated/never married and widowed, were more likely to be disabled compared to those who were married. Among older men alone, having no partner (divorced/separated/never married) increased the odds of disability. Among older women alone, being widowed increased the odds of disability.
Education level was a significant correlate of disability among older men only. Older men with primary education had increased odds of disability.
Older men who depended on remittances had increased odds of disability compared to those who depended on farming. However, older women who depended on wages had decreased odds of disability compared to those who depended on farming. Older women who had a technical skill had increased odds and those whose households owned a bicycle had decreased odds of disability.
Finally, illness during last 30 days and self-reported NCDs were significantly associated with disability among men, women and all older persons. All older persons who were sick and reported an NCD had increased odds of disability. This pattern was observed for both older men and women.
Discussion
Burden of disability
The prevalence of disability among older persons in Uganda (33%) is higher than that of the general population (4%) according to the 2002 census (Citation41) and the 2010 UNHS estimate of 16% (Citation14). It is still higher than the 2011 UDHS rate of 20% (Citation16). Studies elsewhere have reported that disability is higher among older population than the younger or general population (Citation13). For example, in Malaysia, disability was reported to be highest (25%) among those aged 60 and older compared to those younger than age 60 (Citation22). A multi-country study using World Health Survey data among 57 countries reported disability ranging from 24% among older men to 40% in older women, which were higher than those of lower ages (Citation24).
Correlates of disability
As expected, advancement in age was associated with disability among men, women and all older persons. Irrespective of gender, advancement in age leads to the depreciation in the physical functioning of body organs and systems. In addition, advanced age is associated with NCDs that elevate the risk of disability among older people. Our result is in consonance with other studies in Nigeria (Citation17), Ghana (Citation33), rural South Africa (Citation26), Tanzania (Citation32), the United States (Citation25), Malaysia (Citation22), and Brazil (Citation1).
Rural residence was associated with a higher risk of disability than urban residence for all older persons and older women only. This finding is because of rural–urban differentials in socio-economic status and access to healthcare, to the disadvantage of the former. In addition, older persons tend to migrate to rural areas when they either retire or develop some disability and/or a debilitating chronic health condition (Citation42). However, a study in Brazil reported contrasting results that rural older persons were less likely to report disability (Citation1, Citation28). In addition, there is no clear explanation that can be given for the inconsistent results for older men.
Living alone was associated with disability among all older persons. Living alone, an indicator of vulnerability, has been associated with disability among older people in Uganda (Citation43). According to the social model of disability and intergenerational solidarity (Citation9), older persons living alone are deprived of emotional and physical support from their adult children and the ‘direct health promotional effect of marriage, social support from spouse’ (Citation29). Furthermore, access to adequate healthcare during ill health becomes a challenge for such older persons (Citation9). Subsequently, health conditions that would be prevented such as cataracts might go untreated and lead to total blindness. However, living alone had no significant association with older men and women alone.
Divorced/separated/widowed marital status was associated with disability among men and women. For older women only, being widowed was a bigger problem because about half (49%) of them were widowed. Having no spouse leads to loneliness and depression among older people. Loneliness and depression has been reported to increase the risk of disability among older people (Citation2, Citation25) (Citation30, Citation44). Depression resulting from the presence of NCDs, in the absence of emotional support from a partner, can lead to disability also.
Dependence on remittances was associated with disability among older men and all older persons. Being dependent on remittances implies higher likelihood of disability compared to dependence on farming or wages (older women). Those who depend on remittances are disabled and unable to fend for themselves, requiring their relatives to send them assistance to survive. In contrast, older people who are engaged in farming or who receive wages, are still physically fit and hence do not need remittances compared to those who are disabled. Thus, disability calls for significant dependence; the need for care and support from adult children or relatives (Citation45).
Furthermore, disability was significantly associated with ill health and NCDs. Older persons find difficulties in accessing healthcare and are therefore, more likely to be sick. Similarly, reporting at least an NCD (such as diabetes, heart disease, and hypertension), was strongly associated with disability among older persons. Diabetes (Citation2, Citation7) (Citation35, Citation46), heart disease (Citation10, Citation25) (Citation34), and hypertension (Citation2, Citation10) (Citation30) have been strongly associated with disability among older people.
Although gender was significantly associated with disability at bivariate analysis (), it became insignificant at multivariate analysis (), contrary to findings from several other studies (Citation3, Citation13) (Citation17, Citation20) (Citation24, Citation30). For example, in Malawi, older women were more likely to be disabled than older men (Citation19). It is not clear why there were no gender differentials in the prevalence of disability among older persons in Uganda.
Limitations of data
Several limitations merit discussion. First, self-reported prevalence of NCDs and disability is most likely to be lower than the actual prevalence of either condition, among older people in Uganda. This paper utilized secondary data where indicators of disability were self-reported. The cross sectional nature of the data is limiting. It is difficult to tell whether disability occurred earlier or after the onset of NCDs among older persons.
Second, it was also difficult to distinguish disabilities from birth and those which were a result of occupational hazards and/or a result of advancement in age, though it was clear that increment in age led to a significant increase in the prevalence of disability among older persons. Despite these limitations, the paper contributes to filling the knowledge gap concerning the prevalence and correlates of disability among older persons in Uganda.
Conclusions and recommendations
Disability was associated with advancement in age, rural residence, living alone, separated/divorced or widowed marital status, and dependence on remittances, sickness, and self-reported NCDs. Therefore, socio-economic vulnerabilities are associated with disability among older persons in Uganda. Surprisingly, gender was not a significant predictor of disability in Uganda.
In order to limit the risk of disability in old age, there is the need for interventions aimed at improving the health of older persons through early prevention and management of NCDs in Uganda. This is because as age increases, the risk of disability from NCDs also increases.
Second, there is a need to reduce socio-economic inequalities among older persons in Uganda. The SAGE, a pilot initiative entailing social cash transfers by the Government in 14 districts, should be rolled out to the entire country in order to promote social protection and improve wellbeing of older persons in Uganda. Special attention should be paid to those who live alone and depend on remittances , as they are more vulnerable compared to other older persons who live with other people.
Third, there is a need for further older persons’ focused research, ideally longitudinal in design that addresses the broad spectrum of ageing and related pertinent issues such as health, living arrangements and intergenerational support in Uganda. This would contribute to a better estimation of NCDs and disability among the older population, and provide a firmer basis for policy advice. Similarly, further investigations to ascertain the association between mental health and disability among older people in African settings should be given priority. The discourse on gender and disability also requires more research especially in sub-Saharan African countries in general and Uganda in particular.
Conflict of interest and funding
There is no conflict of interest declared.
Acknowledgements
The authors thank the Uganda Bureau of Statistics for permission to use the UNHS data and acknowledge the valuable comments and contributions of the members of the Doctoral Committee (DC): Dr. Valerie Golaz, Dr. Gideon Rutaremwa, and Dr. Sandra Kasoma. We acknowledge the valuable comments and review of the manuscript from Prof. Donald Cole. The technical support of Simon Kyewalyanga of Uganda Bureau of Statistics, on the merging of the UNHS data is recognized. This research was partially supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Wellcome Trust (UK) (Grant No: 087547/Z/08/Z), the Department for International Development (DfID) under the Development Partnerships in Higher Education (DelPHE), the Carnegie Corporation of New York (Grant No: B 8606), the Ford Foundation (Grant No: 1100-0399), Google.Org (Grant No: 191994), SIDA (Grant No: 54100029) and MacArthur Foundation (Grant No: 10-95915-000-INP).
We are grateful to the funding received from DAAD Uganda for payment of Stephen's tuition, functional fees and research allowance. We also acknowledge the support of Population Association of America (PAA) for his participation in the 2014 conference in Boston, where this paper was first presented.
Related Research Data
References
- Melzer D, Parahyba MI. Socio-demographic correlates of mobility disability in older Brazilians: results of the first national survey. Age Ageing. 2004; 33: 253–9.
- Sousa RM, Ferri CP, Acosta D, Albanese E, Guerra M, Huang Y, etal. Contribution of chronic diseases to disability in elderly people in countries with low and middle incomes: a 10/66 dementia research group population-based survey. Lancet. 2009; 374: 1821–30.
- Strobl R, Muller M, Emeny R, Peters A, Grill E. Distribution and determinants of functioning and disability in aged adults – results from the German KORA-Age study. BMC Publ Health. 2013; 13: 137.
- Mba CJ. The health condition of older women in Ghana: a case study of Accra city. J Int Wommens Stud. 2006; 8: 171–84.
- Ofstedal M, Zimmer Z, Hermalin A, Chan A, Chuang Y-L, Natividad J, etal. Short-term trends in functional limitation and disability among older Asians: a comparison of five Asian settings. J Cross Cult Gerontol. 2007; 22: 243–61.
- IHME. The global burden of disease: generating evidence, guiding policy. 2013; Seattle, WA: Institute for Health Metrics and Evaluation.
- Wong E, Backholer K, Gearon E, Harding J, Freak-Poli R, Stevenson C. Diabetes and risk of physical disability in adults: a systematic review and meta-analysis. The Lancet Diabetes & Endocrinology. 2013; 1: 106–14. [PubMed Abstract] [PubMed CentralFull Text].
- Braithwaite J, Mont D. Disability and poverty: a survey of World Bank poverty assessments and implications. ALTER-Eur J Disabil Res. 2009; 3: 219–32.
- Mont D. Measuring disability prevalence. World Bank Social Protection Discussion Paper. 2007; Washington, USA: World Bank.
- Medhi GK, Hazarika NC, Borah PK, Mahanta J. Health problems and disability of elderly individuals in two population groups from same geographical location. J Assoc Physicians India. 2006; 54: 539–44. [PubMed Abstract].
- Ostchega Y, Harris TB, Hirsch R, Parsons VL, Kington R. The prevalence of functional limitations and disability in older persons in the US: data from the National Health and Nutrition Examination Survey III. J Am Geriatr Soc. 2000; 48: 1132–5. [PubMed Abstract].
- WHO. The world report on disability. 2011; Geneva, Switzerland: World Health Organization.
- Mitra S, Sambamoorthi U. Disability prevalence among adults: estimates for 54 countries and progress toward a global estimate. Disabil Rehabil. 2014; 36: 940–7.
- UBOS. Uganda National Household Survey 2009–2010. Socio-economic module. 2010; Kampala, Uganda: Uganda Bureau of Statistics. Abridged report.
- UN. World population prospects: the 2010 revision. 2013; New York: United Nations, Department of Economic and Social Affairs, Population Division.
- UBOS, ICF International. Uganda demographic and health survey 2011. 2012; Kampala, Uganda: UBOS.
- Abdulraheem IS, Oladipo AR, Amodu MO. Prevalence and correlates of physical disability and functional limitation among elderly rural population in Nigeria. J Aging Res. 2011; 2011: 369894.
- Dewhurst F, Dewhurst MJ, Gray WK, Orega G, Howlett W, Chaote P, etal. The prevalence of disability in older people in Hai, Tanzania. Age Ageing. 2012; 41: 517–23.
- Payne CF, Mkandawire J, Kohler HP. Disability transitions and health expectancies among adults 45 years and older in Malawi: a cohort-based model. PLoS Med. 2013; 10: e1001435.
- Nyirenda M, Chatterji S, Falkingham J, Mutevedzi P, Hosegood V, Evandrou M, etal. An investigation of factors associated with the health and well-being of HIV-infected or HIV-affected older people in rural South Africa. BMC Publ Health. 2012; 12: 259.
- Tang Z, Wang HX, Meng C, Wu XG, Ericsson K, Winblad B, etal. The prevalence of functional disability in activities of daily living and instrumental activities of daily living among elderly Beijing Chinese. Arch Gerontol Geriatr. 1999; 29: 115–25.
- Hairi NN, Bulgiba A, Cumming RG, Naganathan V, Mudla I. Prevalence and correlates of physical disability and functional limitation among community dwelling older people in rural Malaysia, a middle income country. BMC Publ Health. 2010; 10: 492.
- Ng TP, Niti M, Chiam PC, Kua EH. Prevalence and correlates of functional disability in multiethnic elderly Singaporeans. J Am Geriatr Soc. 2006; 54: 21–9.
- Hosseinpoor AR, Williams JS, Jann B, Kowal P, Officer A, Posarac A, etal. Social determinants of sex differences in disability among older adults: a multi-country decomposition analysis using the World Health Survey. Int J Equity Health. 2012; 11: 52.
- Berlau DJ, Corrada MM, Peltz CB, Kawas CH. Disability in the oldest-old: incidence and risk factors in the 90+ study. Am J Geriatr Psychiatr. 2012; 20: 159–68.
- Gómez-Olivé FX, Thorogood M, Clark B, Kahn K, Tollman S. Assessing health and well-being among older people in rural South Africa. Glob Health Action. 2010; 2: 23–35.
- Hirve S, Juvekar S, Lele P, Agarwal D. Social gradients in self-reported health and well-being among adults aged 50 and over in Pune District, India. Glob Health Action. 2010; 2: 88–95.
- Parahyba MI, Veras R, Melzer D. Disability among elderly women in Brazil. Rev Saude Publica. 2005; 39: 383–90.
- Wang H, Chen K, Pan Y, Jing F, Liu H. Associations and impact factors between living arrangements and functional disability among older Chinese adults. PLoS One. 2013; 8: e53879.
- Scholten F, Mugisha J, Seeley J, Kinyanda E, Nakubukwa S, Kowal P, etal. Health and functional status among older people with HIV/AIDS in Uganda. BMC Publ Health. 2011; 11: 886.
- Koster A, Bosma H, Broese van Groenou MI, Kempen GI, Penninx BW, van Eijk JT, etal. Explanations of socioeconomic differences in changes in physical function in older adults: results from the Longitudinal Aging Study Amsterdam. BMC Publ Health. 2006; 6: 244.
- Mwanyangala MA, Mayombana C, Urassa H, Charles J, Mahutanga C, Abdullah S. Health status and quality of life among older adults in rural Tanzania. Glob Health Action. 2010; 3 2142, doi: http://dx.doi.org/10.3402/gha.v3i0.2142 .
- Debpuur CY, Welaga P, Wak G, Hodgson A. Self-reported health and functional limitations among older people in the Kassena-Nankana District, Ghana. Glob Health Action. 2010; 3 doi: http://dx.doi.org/10.3402/gha.v3i0.2151 .
- Fried LP, Guralnik JM. Disability in older adults: evidence regarding significance, etiology, and risk. J Am Geriatr Soc. 1997; 45: 92–100. [PubMed Abstract].
- Wray LA, Ofstedal MB, Langa KM, Blaum CS. The effect of diabetes on disability in middle-aged and older adults. J Gerontol A Biol Sci Med Sci. 2005; 60: 1206–11.
- Woo J, Ho SC, Yu LM, Lau J, Yuen YK. Impact of chronic diseases on functional limitations in elderly Chinese aged 70 years and over: a cross-sectional and longitudinal survey. J Gerontol A Biol Sci Med Sci. 1998; 53: M102–6.
- Nyirenda M, Newell ML, Mugisha J, Mutevedzi PC, Seeley J, Scholten F, etal. Health, wellbeing, and disability among older people infected or affected by HIV in Uganda and South Africa. Glob Health Action. 2013; 6: 19201. doi: http://dx.doi.org/10.3402/gha.v6i0.19201 [PubMed Abstract].
- Gómez-Olivé FX, Thorogood M, Clark B, Kahn K, Tollman S. Self-reported health and health care use in an ageing population in the Agincourt sub-district of rural South Africa. Glob Health Action. 2013; 6: 19305. doi: http://dx.doi.org/10.3402/gha.v6i0.19305 .
- Kyobutungi C, Egondi T, Ezeh A. The health and well-being of older people in Nairobi's slums. Glob Health Action. 2010; 3 doi: http://dx.doi.org/10.3402/gha.v3i0.2138 .
- Barberger-Gateau P, Rainville C, Letenneur L, Dartigues JF. A hierarchical model of domains of disablement in the elderly: a longitudinal approach. Disabil Rehabil. 2000; 22: 308–17.
- UBOS. Uganda population and housing census. 2002; Kampala, Uganda: Uganda Bureau of Statistics.
- Litwak E, Longino CF. Migration patterns among the elderly: a developmental perspective. Gerontologist. 1987; 27: 266–72.
- Golaz V, Rutaremwa G. The vulnerability of older adults: what do census data say? An application to Uganda. Afr Popul Stud. 2011; 26: 605–22.
- Tsang A, Von Korff M, Lee S, Alonso J, Karam E, Angermeyer MC, etal. Common chronic pain conditions in developed and developing countries: gender and age differences and comorbidity with depression-anxiety disorders. J Pain. 2008; 9: 883–91.
- Uwakwe R, Ibeh CC, Modebe AI, Bo E, Ezeama N, Njelita I, etal. The epidemiology of dependence in older people in Nigeria: prevalence, determinants, informal care, and health service utilization. A 10/66 dementia research group cross-sectional survey. J Am Geriatr Soc. 2009; 57: 1620–7.
- Hjelm K, Atwine F. Health-care seeking behaviour among persons with diabetes in Uganda: an interview study. BMC Int Health Hum Right. 2011; 11: 11.