Abstract
Tick-borne encephalitis (TBE) is associated with higher morbidity and induces a stronger intrathecal immune activation than most other viral induced meningo-encephalitis. The aim of this study was to investigate cytokine concentrations in cerebrospinal fluid (CSF) and serum in relation to aetiology and clinical course. Cytokines were analysed by Enzyme-linked Immuno Assay (ELISA) from 44 patients with TBE and from 36 patients with aseptic meningo-encephalitis of other aetiology (non-TBE). Significantly increased CSF levels of Interferon-γ (IFN-γ), Interleukin-10 (IL-10), Interleukin-6 (IL-6), Interleukin-1 receptor antagonist (IL-1ra), and soluble CD8 receptor (sCD8) were detected in both cohorts. Tumour necrosis factor-α (TNF-α showed low levels or was not detected in CSF in any group in the acute stage. However, the CSF levels of IL-10 were significantly lower in TBE than in non-TBE cases 0–6 days after onset of encephalitis. The TBE patients with encephalitis had significantly lower IL-10 CSF levels later in the clinical course (day 7–18) than TBE patients with meningeal disease. Increased IFN-γ production, but low IL-10 secretion, may be of pathophysiological significance in TBE.
Introduction
Tick-borne encephalitis (TBE) is caused by a flavivirus. A Western TBE virus (TBEV) appears endemic in Scandinavia, parts of Central Europe, the Baltic region, and Russia Citation1. The disease is characterised by a protracted course with dominating encephalitic symptoms, rarely lethal, but with considerable morbidity at long-term follow-up Citation2 Citation3.
The pathophysiological mechanisms in TBE are not clarified. We have previously shown that TBE-patients react with a stronger intrathecal immune activation than patients with most other viral meningo-encephalitis indicated by CSF neopterin response Citation4. The proinflammatory T-helper 1(Th 1) response is partly regulated by IFN-γ, while the humoral immune response is induced by T-helper (Th 2) activity that is influenced by Interleukin-10 (IL-10) Citation5. The IL-10 is synthesised in the brain and acts to limit the neuronal damage by suppressing the inflammatory process in meningitis Citation6. Interleukin-1 receptor antagonist (IL-1ra) has a protective role in inflammatory reaction Citation7. Tumour necrosis factor-α (TNF-α) and Interleukin 6 (IL-6) are important in acute inflammatory responses Citation8. Activation of CD8 positive cells induces secretion of soluble CD8 receptor (sCD8) and may reflect ongoing T-cell activation of major importance in most viral infections in the CNS Citation9.
The aim of this study was to investigate whether intrathecal synthesis of cytokines arise in viral aseptic meningo-encephalitis, and to compare this response in TBE with non-TBE cases in relation to clinical course and outcome.
Methods
Study design and population
After informed consent, 80 consecutive patients with clinical symptoms and signs of acute viral meningitis, admitted to Danderyds and Huddinge Hospital, Sweden, entered a prospective study during 1991 to 1993. Forty-four of these patients had TBE. In the other 36 patients, aseptic meningo-encephalitis was of non-TBE aetiology and these were included prospectively as a reference group (non-TBE) (). Established diagnoses among non-TBE patients were enteroviral infection in 14 patients, Herpes simplex virus type 2 infection (HSV type 2) in 7 patients, and cytomegalovirus infection in one patient. In 14 patients the aetiology remained unknown. Cerebrospinal fluid and serum specimens were obtained on admission to hospital median 2 days; range 0–6 (Day 2) n=42, after 9 days; range 7–19 (Day 9) n=34, after 40 days; range 21–67 days (Week 6) n=52, and after 13 month; range 11–16 (1 year) n=32, after onset of meningo-encephalitis. The samples were stored at −20°C.
Table 1. Demographic data, clinical course, and classification in patients (n=80) with tick-borne encephalitis (TBE) and other viral meningitis (non-TBE)
Viral diagnosis
Tick-borne encephalitis was diagnosed by the demonstration of specific IgM activity (µ-capture IgM ELISA) in serum, verified with a significant rise in complement-fixing activity between acute- and convalescent-phase sera Citation10. Enteroviral infection was diagnosed by isolation of the virus from CSF (n = 4), and/or faecal sample (n = 5) in GMK-AH1/RD cells Citation11, or significant rise in, or high, IgG (n = 2) activity in combination with significant change in paired IgM titres (n = 12) Citation12 , or significant rise in complement-fixing activity (n = 5), or by demonstration of enteroviral RNA (n = 2) by polymerase chain reaction (PCR) in CSF Citation13. Extraction was performed with the method described as ‘GuSCN-DNA/RNA’ Citation14. The HSV type 2 was diagnosed by the demonstration of HSV DNA in CSF by polymerase chain reaction (PCR) (n = 7) and/or intrathecal synthesis of anti-HSV activity by capture-ELISA in CSF and serum Citation15 Citation16 Citation17 .
Cytokine levels in cerebrospinal fluid
Interleukin-10, IFN-γ, IL-1ra, TNF-α, and IL–6 were analysed with EIA methods (Quantikine, R&D systems Europe, Oxon, UK), TNF-α and IL-6 with EASIA (Medgenix Diagnostix, Brussels, Belgium), as well as soluble CD8 antigen (T-cell Sciences Inc., Cambridge, MA). Normal serum reference values were established by assessing 30 healthy blood donors (Blood transfusion unit, Karolinska Hospital, Sweden) and normal CSF values by analysing 30 patients undergoing examination for headache without detectable organic disease (Department of Neurology, Karolinska University Hospital, Sweden). Normal values: IL-10 ≤ 1.6 pg/ml in serum and ≤2.2 pg/ml in CSF, IFN-γ ≤ 1.0 u/ml in serum and ≤1.0 u/ml in CSF, IL-1ra ≤ 670 pg/ml in serum and ≤436 pg/ml in CSF, sCD8 ≤ 427 in serum and ≤43 u/ml in CSF, TNF-α ≤ 95 pg/ml in serum and ≤66 pg/ml in CSF, and IL-6 ≤ 24 pg/ml in serum and ≤6.0 in CSF. Upper normal limits for cytokine concentrations were calculated as the mean plus two standard deviations.
Statistical analysis
Comparisons between groups were performed using the Mann-Whitney U-test for non-parametric continuous independent variables (cytokine samples), proportions were compared using Fisher's exact test, and the Spearman Rank Correlation was used in calculating correlations.
Results
The clinical outcome, classification, and other demographic data are presented in . Six TBE patients (14%) developed severe myelitis and/or radiculitis followed by paresis of the spinal nerves. One patient with TBE developed tetraparesis requiring assisted ventilation.
Interferon-γ and interleukin-10
Interferon-γ concentrations () in the CSF were increased on day 2 in both TBE and non-TBE cases, and decreased rapidly after 6 days. The CSF levels of IFN-γ exceeded serum levels in the majority of patients during early stage of disease indicating intrathecal synthesis. At 1-year follow-up, the intrathecal levels of IFN-γ were normal. There were no significant differences in IFN-γ CSF concentrations between TBE and non-TBE at any time point. Initial (day 2) CSF levels exceeded the upper normal limit in 19/24 (79%) of TBE patients and in 11/18 (61%) of non-TBE patients. On day 9, 4/19 (21%) CSF samples in TBE patients and 2/15 (13%) in non-TBE were elevated. The corresponding figures were 3/25 (12%) and 0/27, respectively, in week 6 and after 11–13 months, levels were normal in all patients. No correlation between the IFN-γ concentration and severity of disease or appearance of encephalitis were found.
Fig. 1. IFN-γ- (u/ml) and IL-10- (pg/ml) in CSF and in serum in patients with TBE or aseptic meningo-encephalitis of other aetiology (non-TBE). Line plot: CSF and serum concentrations (geometric mean). Box plot: CSF concentrations (percentiles: 10, 25, 50, 75, and 90%). Normal upper limits (horizontal line): IFN-γ in the CSF < 1.0 u/ml and in serum ≤ 1.0 u/ml; IL-10 in the CSF ≤ 2.2 pg/ml and in serum ≤ 1.6 pg/ml.
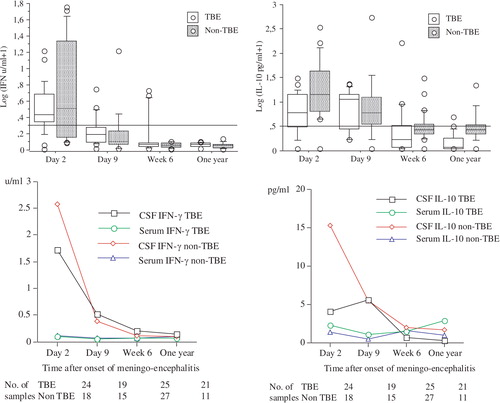
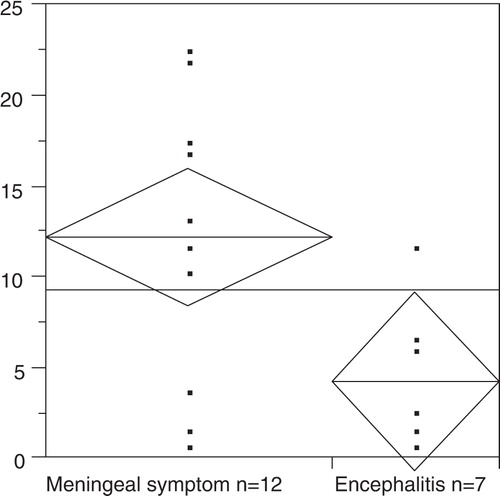
The CSF-levels of IL-10 () exceeded serum levels in the majority of patients during early stage of disease indicating intrathecal synthesis. The initial (day 2) CSF levels of IL-10 in TBE patients were significantly lower than in non-TBE (p = .01). Later in the course of the disease the CSF concentrations decreased and showed no differences between TBE and non-TBE patients. However, there was a considerable overlap in CSF levels between patients with non-TBE and those with TBE. The TBE cases with moderate to severe encephalitis (n=21) had significantly lower IL-10 concentrations in the CSF than TBE patients with predominantly meningeal symptoms (p = .02) at day 10 (geometric mean 3 pg/ml, range 0.7–12 and 13 pg/ml, range 0.7–23, respectively) (). Elevated IL-10 was found in 17/24 (71%) TBE cases and in 17/18 (94%) non-TBE (p = .05) 2 days after onset of disease. This difference remained between day 9 (TBE 14/19, 74% and non-TBE 12/15, 80%) and week 6 (TBE 5/25, 20% and non-TBE 10/27, 37%). The IL-10 levels were elevated in one of 21 CSF samples at 1 year in TBE and in three CSF samples of 11 in non-TBE.
Fig. 2. Concentrations of IL-10 (pg/ml) at 10 days (range 7–18) after onset of meningo-encephalitis in patients with TBE (n=19). Icons: the central bar represents the mean of the group, the height represents 95% confidence interval and the width represents the sample size.
Tumour necrosis factor-α and Interleukin-6
The TNF-α concentrations were generally low regardless of aetiology. The TBE patients exhibited no evidence for intrathecal synthesis of TNF-α with only one of 10 samples above upper normal limit day 2 (geometric mean 10.0 pg/ml, range 1–85) and all normal after 1 year. No differences between the groups were noted regarding clinical course or outcome and TNF-α levels.
Interleukin-6 CSF concentrations were initially high in all patients regardless of aetiology, with no significant differences between TBE (geometric mean 261 pg/ml, range 4–585) and non-TBE (geometric mean 212 pg/ml, range 7–527) and exceeded serum levels in the majority of patients indicating intrathecal synthesis. The CSF levels decreased rapidly within 1–3 weeks. Early in the clinical course (day 2) 26/27 (96%) of the samples in TBE patients and 19/19 (100%) samples in non-TBE were above normal limit. Of the TBE patients (geometric mean 23 pg/ml, range 2–611) 16/22 (73%) and of the non-TBE patients (geometric mean 7 pg/ml, range 1–490) 9/17 (53%), all had concentrations exceeding the upper normal limit on day 9. The corresponding figures were 3/26 (12%) and 0/27, respectively, in week 6. All normalised after 11–13 months.
Interleukin-1 receptor antagonist and soluble CD8 receptors
The IL-1ra was initially increased in all TBE patients (geometric mean 2835 pg/ml, range 1642–3957) and in non-TBE (geometric mean 2621 pg/ml, range 109–4865), exceeding serum levels in all cases indicating intrathecal synthesis. Higher levels were noted in non-TBE than in TBE, although not reaching statistical significance. The IL-1ra and IL-10 levels correlated significantly to each other between day 2 to 9 (p < .01). A normalisation was found in all cases thereafter.
Elevated levels of sCD8 were demonstrated initially in CSF on median day 2 in both TBE patients (geometric mean 48 u/ml, range 4.5–251) and non-TBE (geometric mean 66 u/ml, range 9–978), without significant difference between the groups. The levels were initially higher in non-TBE, with considerable overlap between patients. The concentrations increased in TBE patients between week 1 and week 6 and reached higher levels in TBE patients than in non-TBE, although the difference did not reach statistical significance. The proportion of positive CSF samples on day 2 was 10/16 (63%) in TBE and 6/13 (46%) in non-TBE. On day 9, sCD8 levels were above the normal limit in 18/20 (90%) of TBE patients and in 10/13 (77%) in non-TBE. At week 6, 16/20 (80%) CSF samples in TBE and 5/14 (36%) in non-TBE were elevated (p = .01). At 1 year, 3/19 (16%) samples were elevated in TBE patients and none in the non-TBE patients.
Discussion
The major issue of this study was the balance between proinflammatory and B-cell activity cytokine responses in CNS in relation to the clinical course and outcome of aseptic meningo-encephalitis. Overall in the initial course of TBE as well as in non-TBE-cases, we found increased intrathecal IL-10. However, in severe TBE as compared to TBE with predominantly meningeal symptoms there was significantly lower intrathecal IL-10 levels at second CSF sampling at 7–19 days after onset of symptoms. The IL-10 can downregulate IFN-γ synthesis and probably acts as an immunosuppressive cytokine that inhibits the formation of proinflammatory Type 1 cytokine cascade. A low production of IL-10, however, may result in delayed or inhibited downregulation of inflammatory mediators (IL-1, TNF-α, IL-6) and more severe encephalitis in TBE. In addition, it may result in low induction of anti-TBE-antibody production. This may influence the development of severe TBE disease caused by an increased inflammatory reaction in the CNS due to IFN-γ activity and infiltrating mononuclear cells or reduced production of neutralising antibodies. However, IFN-γ activity is necessary to inhibit viral replication and is important in generating cytotoxic defence to most viral infection Citation18. IFN-γ concentrations in CSF were elevated during the acute phase of aseptic meningitis irrespective of aetiology. In human studies different lymphocyte subsets may produce both proinflammatory and downregulatory response depending on antigen presentation Citation19. The IL-10 modulates the immune response and also acts with a downregulating impact on MHC II-restricted antigen-presenting capacity in macrophages and monocytes Citation20 Citation21. The downregulating ability of IL-10 is linked to Th 2 response and has also been shown in HIV infection Citation22. A study on another flaviviral disease showed that Japanese encephalitis virus decreases the expression of IL-10 in the CNS Citation23. The level of proinflammatory cytokines was inversely proportional to the decrease of IL-10 and the endogenous IL-10 production was blocking the neuronal death.
Interleukin-6 (IL-6) is a mediator of the cytokine cascade with impact on the humoral response in viral disease Citation24. In our study the humoral pathway mediated by IL-6 indicated no differences in intrathecal expression between TBE and non-TBE patients. Low intrathecal TNF-α level was found, as in other studies Citation25. TNF-α precedes IL-6 production and the peak activity may be passed at onset of meningo-encephalitis, when the first CSF sample was obtained. In diseases with ischemic tissue damage and persisting viral replication, TNF-α levels may be elevated for longer time points. In herpes simplex encephalitis, TNF-α peaked in early convalesce phase 2 to 6 weeks after onset of encephalitis Citation9. The initial high IL-1ra levels in both study cohorts may act as a shelter against inflammation by downregulating IL-1 mediated/induced cytokine expression in both TBE and non-TBE cases.
Cytokines are produced intrathecally in patients with viral meningo-encephalitis. Different viral aetiologies produce unique inflammatory responses via different pathogenic pathways. Patients with a more protracted course may represent a different individual response to the pathogenic pattern of TBE. This theory is supported by the present results. A restricted downregulatory proinflammatory cytokine response may be a part of the pathogenic course in TBE that results in more severe encephalitis than in non-TBE cases. Decreased IL-10 expression in the CSF of TBE patients after the first week of disease may indicate more aggressive encephalitis secondary to a more disseminated viral spread in accordance with the study on Japanese encephalitis Citation23. Treatment with substances blocking proinflammatory cytokines or anti-inflammatory drugs may be beneficial. Alternatively, stimulation of an early downregulatory Th 2 cytokine response may protect the patient from more severe encephalitis.
Informed consent was obtained from all patients and the local ethical committee approved the study.
Conflict of interest and funding
Grant support: Medical Research Council (B95-16X-09924-04B) and The Development Fund of Danderyd Hospital.
Acknowledgements
We thank Ms Kerstin Lövgren, Department of Infectious Diseases, Danderyd Hospital, for excellent help with patient care and collecting the samples.
References
- Lindquist L, Vapalahti O. Tick-borne encephalitis. Lancet. 2008; 371: 1861–71.
- Günther G, Haglund M, Lindquist L, Forsgren M, Sköldenberg B. Tick-borne encephalitis in Sweden in relation to aseptic meningo-encephalitis of other etiology: a prospective study of clinical course and outcome. J Neurol. 1997; 244: 230–8.
- Haglund M, Forsgren M, Lindh G, Lindquist L. A 10-year follow-up study of tick-borne encephalitis in the Stockholm area and a review of the literature: need for a vaccination strategy. Scand J Infect Dis. 1996; 28: 217–24.
- Günther G, Haglund M, Lindquist L, Sköldenberg B, Forsgren M. Intrathecal production of neopterin and beta 2 microglobulin in tick-borne encephalitis (TBE) compared to meningoencephalitis of other etiology. Scand J Infect Dis. 1996; 28: 131–8.
- Mosmann TR, Coffman RL. TH1 and TH2 cells: different patterns of lymphokine secretion lead to different functional properties. Annu Rev Immunol. 1989; 7: 145–73.
- Strle K, Zhou JH, Shen WH, Broussard SR, Johnson RW, Freund GG, et al.. Interleukin-10 in the brain. Crit Rev Immunol. 2001; 21: 427–49.
- Ramilo O, Saez-Llorens X, Mertsola J, Jafari H, Olsen KD, Hansen EJ, et al.. Tumor necrosis factor alpha/cachectin and interleukin 1 beta initiate meningeal inflammation. J Exp Med. 1990; 172: 497–507.
- Teranishi T, Hirano T, Arima N, Onoue K. Human helper T cell factor(s) (ThF). II. Induction of IgG production in B lymphoblastoid cell lines and identification of T cell-replacing factor-(TRF) like factor(s). J Immunol. 1982; 128: 1903–8.
- Aurelius E, Andersson B, Forsgren M, Sköldenberg B, Strannegard Ö. Cytokines and other markers of intrathecal immune response in patients with herpes simplex encephalitis. J Infect Dis. 1994; 170: 678–81.
- Heinz FX, Roggendorf M, Hofmann H, Kunz C, Deinhardt F. Comparison of two different enzyme immunoassays for detection of immunoglobulin M antibodies against tick-borne encephalitis virus in serum and cerebrospinal fluid. J Clin Microbiol. 1981; 14: 141–6.
- Glimåker M, Abebe A, Johansson B, Ehrnst A, Olcen P, Strannegård O. Detection of enteroviral RNA by polymerase chain reaction in faecal samples from patients with aseptic meningitis. J Med Virol. 1992; 38: 54–61.
- Samuelsson A, Skoog E, Forsgren M. Aspects on the serodiagnosis of enterovirus infections by ELISA. Serodiagn Immunother Infect Dis. 1990; 4: 395–406.
- Glimåker M, Johansson B, Olcen P, Ehrnst A, Forsgren M. Detection of enteroviral RNA by polymerase chain reaction in cerebrospinal fluid from patients with aseptic meningitis. Scand J Infect Dis. 1993; 25: 547–57.
- Casas I, Powell L, Klapper PE, Cleator GM. New method for the extraction of viral RNA and DNA from cerebrospinal fluid for use in the polymerase chain reaction assay. J Virol Methods. 1995; 53: 25–36.
- Aurelius E, Johansson B, Sköldenberg B, Staland A, Forsgren M. Rapid diagnosis of herpes simplex encephalitis by nested polymerase chain reaction assay of cerebrospinal fluid. Lancet. 1991; 337: 189–92.
- Aurelius E, Johansson B, Sköldenberg B, Forsgren M. Encephalitis in immunocompetent patients due to herpes simplex virus type 1 or 2 as determined by PCR or type-specific antibody assays of cerebrospinal fluid. J Med Virol. 1991; 27: 591–4.
- Forsgren M, Skoog E, Jeansson S, Olofsson S, Giesecke J. Prevalence of antibodies to herpes simplex virus in pregnant women in Stockholm in 1969, 1983 and 1989: implications for STD epidemiology. Int J STD AIDS. 1994; 5: 113–6.
- Huang S, Hendriks W, Althage A, Hemmi S, Bluethmann H, Kamijo R, et al.. Immune response in mice that lack the interferon-gamma receptor. Science. 1993; 259: 1742–5.
- Cardell S, Sander B, Moller G. Helper interleukins are produced by both CD4 and CD8 splenic T cells after mitogen stimulation. Eur J Immunol. 1991; 21: 2495–500.
- de Waal Malefyt R, Haanen J, Spits H, Roncarolo MG, te Velde A, Figdor C, et al.. Interleukin 10 (IL-10) and viral IL-10 strongly reduce antigen-specific human T cell proliferation by diminishing the antigen-presenting capacity of monocytes via downregulation of class II major histocompatibility complex expression. J Exp Med. 1991; 174: 915–24.
- Gallo P, Sivieri S, Rinaldi L, Yan XB, Lolli F, De Rossi A, et al.. Intrathecal synthesis of interleukin-10 (IL-10) in viral and inflammatory diseases of the central nervous system. J Neurol Sci. 1994; 126: 49–53.
- Maggi E, Mazzetti M, Ravina A, Annunziato F, de Carli M, Piccinni MP, et al.. Ability of HIV to promote a TH1 to TH0 shift and to replicate preferentially in TH2 and TH0 cells. Science. 1994; 265: 244–8.
- Swarup V, Ghosh J, Duseja R, Ghosh S, Basu A. Japanese encephalitis virus infection decrease endogenous IL-10 production: correlation with microglial activation and neuronal death. Neurosci Lett. 2007; 420: 144–9.
- Moskophidis D, Frei K, Lohler J, Fontana A, Zinkernagel RM. Production of random classes of immunoglobulins in brain tissue during persistent viral infection paralleled by secretion of interleukin-6 (IL-6) but not IL-4, IL-5, and gamma interferon. J Virol. 1991; 65: 1364–9.
- Glimåker M, Kragsbjerg P, Forsgren M, Olcen P. Tumor necrosis factor-alpha (TNF alpha) in cerebrospinal fluid from patients with meningitis of different etiologies: high levels of TNF alpha indicate bacterial meningitis. J Infect Dis. 1993; 167: 882–9.