Abstract
Inuit Canadians are on average about 20 years younger and have a 10-year lower life expectancy than other Canadians. While there have been improvements in Inuit health status over time, significant health disparities still remain. This paper will review the peer-reviewed literature related to Inuit child, youth, and maternal health between 2000 and 2010, investigate which thematic areas were examined, and determine what proportion of the research is related to each group. Establishing areas of research concentrations and scarcities may help direct future research where it is needed. We followed a systematic literature review and employed peer-reviewed research literature on child, youth, and maternal health which were selected from 3 sources, MEDLINE, CINAHL, and the Circumpolar Health Bibliographic Database. The resulting references were read, and summarized according to population group and thematic area. The thematic areas that emerged by frequency were: infectious disease; environment/environmental exposures; nutrition; birth outcomes; tobacco; chronic disease; health care; policy, human resources; interventions/programming; social determinants of health; mental health and wellbeing; genetics; injury; and dental health. The 72 papers that met the inclusion criteria were not mutually exclusive with respect to group studied. Fifty-nine papers (82%) concerned child health, 24 papers (33%) youth health, and 58 papers (81%) maternal health. The review documented high incidences of illness and significant public health problems; however, in the context of these issues, opportunities to develop research that could directly enhance health outcomes are explored.
According to the 2006 Census, more than half of the Canadian Aboriginal population lived in urban centres Citation1; however, approximately 80% of the Inuit population of Canada still live in their traditional territories Citation2. Between 1996 and 2006, the Inuit population of Canada increased by 26%. This is a young population with an average age of 22 years compared to 40 years for non-Aboriginal Canadians Citation1. The life expectancy of the Inuit is on average 10 years less than for non-Aboriginal Canadians Citation3.
While there have been some gains in Inuit health status through advances in medical science and delivery of certain types of care which have led to a decline in the incidence of infectious diseases; chronic diseases, injuries, substance abuse have increased and have become significant concerns Citation4. Furthermore, there are remarkable differences between Inuit and non-Inuit Canadians for many indicators of health.
Inuit Canadians have higher rates of preterm birth, stillbirth, and infant death compared to other Canadians Citation5. Compounding these rates is that 9% of Inuit teenagers are parents, whereas 1.3% of other Canadian teenagers are parents Citation3. Young mothers are less likely to breastfeed, and are more likely to smoke and drink alcohol Citation6 Citation7. In fact, expecting Inuit mothers have the highest tobacco smoking rate in the country, at over 80% Citation8 Citation9. These factors, and others, contribute to poor health outcomes among infants and children Citation9 Citation10. The frequency of reported hunger among children is another important measure of a population's health status. Sixty-eight percent of Inuit children aged 6–14 years of age experienced being hungry, of which 57% reported being hungry every few months or more Citation11. The prevalence of hunger was 1.2% among other Canadian families (with children aged 11 years of less) based on 1994 data Citation12. An individual's self-reported rating of his/her health status is a commonly used measure of a populations’ health status. Only 52% of Inuit males and 48% of females aged 15 and older reported that their health status was excellent or very good Citation13, compared to 60% among other Canadians as a whole Citation14. Moreover, Inuit currently experience the highest levels of overcrowded (38%) and inadequate housing (31%) in the country (compared to 3 and 7% among other Canadians respectively) Citation15 Citation16.
Interrelated factors affect the health of Inuit populations and vary during a life course. These range from their social, economic, physical and demographic circumstances. According to Mary Simon, the President of Inuit Tapiriit Kanatami (ITK), “Solutions must be multi-faceted and multi-jurisdictional. Inuit know that change is needed and that youth are the key. Improving access to services and programs targeted at children, youth and their parents must be a priority in efforts to address the health inequities faced by Inuit” Citation17. Additionally, reviews of the Inuit health literature to date have highlighted a need for culturally-based health prevention interventions Citation18–Citation20, the return of childbirth to home communities Citation21, an understanding of the mechanisms through which the determinants of health affect Inuit women Citation22, and control of otitis media in Inuit children and youth Citation10.
Towards advancing Inuit health outcomes at the population level as advocated by ITK and other organizations representing Inuit Canadians Citation23, improvements to child, youth and maternal health are paramount. The present review will examine the peer-reviewed literature related to Inuit child, youth, and maternal health between 2000 and 2010. It will determine what proportion of the research was related to each of the 3 population groups, and establish which thematic areas were most common. Directions for future research will be proposed based on these findings.
Materials and methods
Search strategy
The publications included in the peer-reviewed research literature on child, youth, and maternal health were selected from 3 sources, MEDLINE, CINAHL and the Circumpolar Health Bibliographic Database, a project of the Canadian Institutes of Health Research (CIHR) Team in Circumpolar Health Research.
The keyword “Inuit”, with limits on the publication years from January 1, 2000 to December 31, 2010 was the first term used in the MEDLINE and CINAHL searches. Within these search results “children/child”; “youth/adolescents”; and “maternal” were accessed individually. Every resulting title was read to determine whether the paper's abstract should be read. After reading a paper's abstract, the paper's eligibility was determined. Papers were excluded if they were not in English; the Inuit population under study was not Canadian; the Inuit sample was not de-aggregated from Aboriginal or Indigenous data; the paper was a review, a letter, an editorial, or a discussion piece; the paper was a presentation abstract; the study evaluated a sampling measure or technique or biomarker; or the paper had an arctic or environmental focus without relating the findings to a particular population. A similar search strategy was used with the Searches in the Circumpolar Health Bibliographic Database.
Data analysis
The papers were read and summarized based on thematic area. The themes that emerged were: birth outcomes; chronic disease; dental health; environment/environmental exposures; genetics; health care, policy, human resources; infectious disease; injury; interventions/programming; mental health and wellbeing; nutrition; social determinants of health; and tobacco. Population group (child, youth, maternal) was considered within each thematic area. The data were extracted from published manuscripts therefore no institutional research ethics board approval was needed.
Results
Descriptive findings
Seventy-two papers met the inclusion criteria (). The most common theme was infectious disease. Environment/environmental exposures was second in frequency, and nutrition was third (). Child health was the most common focus of the papers included, followed closely by maternal health, then youth health. The cumulative thematic area content in counts the same paper more than once if it relates to more than 1 population group. Frequency of publications ranged from 1 to 16 a year (). The majority of the studies were cross-sectional in design. Several of the more recent publications were derived from regional surveys, including the Inuit Child Health Survey 2007–2008.
Fig. 1. The frequency of papers by thematic areas in 2000 to 2010 (n = 72).
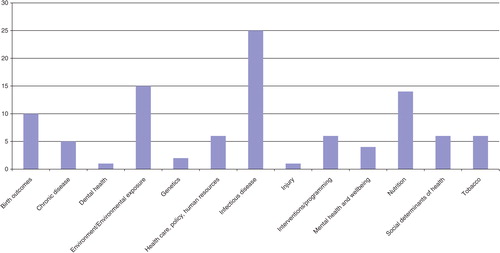
Fig. 2. Distribution of population group categories and the proportion of thematic area content by population group categories in 2000 to 2010.
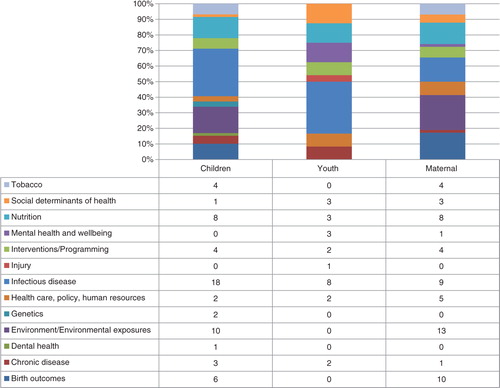
Fig. 3. Distribution of publications by year (2000 to 2010) n = 72.
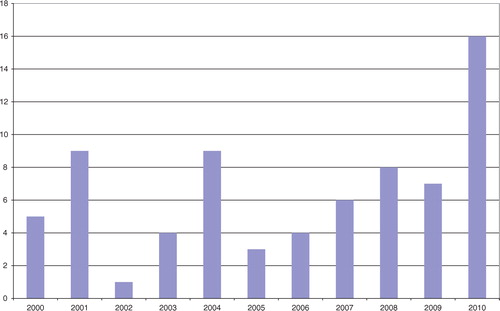
Table I. Summary of Canadian Inuit child, youth, and maternal health peer-reviewed literature by thematic area (2000 to 2010)
Findings by thematic areas
Infectious disease
Infectious diseases were reported in 25 papers representing 35% of the papers included in the review. The majority of these (72%) focused on child health (). Eight papers focused on youth. This represented the largest proportion of the youth literature, at 33% (). Opposite to the experience among the Innu of Newfoundland and Labrador, women of Inuit communities in the region were hospitalization due to pneumonia more often than men Citation24. Hospital admission for lower respiratory tract infections (LRTI) was approximately 11 times more frequent in Nunavik than in other Canadian regions Citation25. Within the Arctic regions of Canada and the United States, indigenous children had the highest rates of Haemophilus influenzae, serotype a Citation26. Rates of HPV were high among Inuit women compared to other women in Canada and the diversity in HPV types may contribute to the overall burden of infection among Inuit women Citation27. Factors associated with the high risk HPV were younger age and having 11 or more lifetime sexual partners Citation28. One study examined factors that were associated with zoonotic infections, specifically Toxoplasma gondii, and demonstrated that age, gender, schooling, and community of residence each influenced serostatus Citation29. A case study that examined characteristics that may be associated with sexually transmitted infections among Inuit youth discussed that, among other things, conversations that once occurred between generations about matters related to reproduction are no longer taking place Citation30. This knowledge gap about sexual health for Inuit youth was referred to elsewhere as well Citation31.
Factors associated with otitis media among Inuit children included: number of persons per bedroom; number of siblings with a history of the disease; age at first, second, and third visit to a nursing station for ear problems; use of formula versus non-formula in bottle-fed children Citation32; neonatal vitamin A deficiency Citation33; and organochlorines Citation34. The impact of these infections is significant. One in 5 youth experienced hearing loss with a demonstrable impact on school performance Citation35. Hearing screening and retesting was recommended for surveillance Citation36. Bronchiolitis was shown to be a serious health problem for Inuit children Citation37 Citation38. In addition they reported that all infants studied lived in crowded homes and were exposed to maternal smoking prenatally as well as environmental tobacco smoke at home Citation38. More recently, factors that have been associated with LRTIs among Inuit children are place of residence, lack of breast-feeding Citation39, reduced ventilation Citation40 Citation41, neonatal vitamin A deficiency Citation33 and above average levels of organochlorines Citation42, and PCBs Citation25.
Environment/environmental exposures
Of the 15 publications on environment or environmental exposure, 13 had a focus on maternal health and represented 22% of the maternal health literature (). Ten papers were relevant to child health topics, which represented 17% of the child health literature. The majority of papers that included an environmental exposure were by way of prenatal nutrition, such as through the consumption of fish or marine mammal fat to a health outcome in offspring. Outcomes of interest were children's neuromotor or behavioural development after adverse effects of prenatal mercury (Hg) Citation43, monomethylmercury (MeHg) Citation44, lead (Pb) Citation43 Citation45 Citation46 and polychlorinated biphenyls (PCBs) Citation43 Citation44 Citation46. A few papers associated contaminants, such as organochlorines Citation34 Citation42 and PCBs Citation25 with childhood acute infections. Others found high levels of exposure to lead Citation47 Citation48, Hg Citation48 and PCBs Citation49. The negative association of tobacco smoking Citation49 and the positive influence of breast-fed children mitigated the effects of these contaminants Citation44. One study demonstrated that despite widespread knowledge about the contaminants associated with country foods, consumption of these foods increased during pregnancy because of their known beneficial qualities Citation50. Two studies demonstrated an advantageous association of increased consumption of omega-3 fatty acids from fish, higher levels of on levels of HDL (“good”) cholesterol triacylglycerols, and better visual, cognitive, and motor development Citation51 Citation52.
Nutrition
Fourteen papers were connected to nutrition (). Overall, these publications were related to food availability and nutrient supplementation. The literature on nutrient supplementation was, for the most part, exploratory. For instance, the potential benefit of grain fortification with folic acid for decreasing the rate of congenital heart defects was the focus of 1 paper Citation53.
The nutritional adequacy of Inuit women's diets during pregnancy and while lactating was assessed along with access to traditional foods. Deficiencies were present in magnesium, zinc, calcium, folate, and vitamins E, A, C Citation54 Citation55, and D Citation56. One study demonstrated that traditional food contributed more to the diets of older Inuit women (aged 40–74) compared to younger Inuit women (18–39), where market food provided more to women's energy intake Citation57. Daily intake of fish for the Inuit in Inuvik was high (131 grams) and was positively associated with beneficial levels of HDL cholesterol and triacylglycerolds Citation51. Through 24-hour dietary interviews, it was determined that Inuit adults generate 6–40% of their daily energy from traditional food, whereas these foods contributed to only 0.4–15% of Inuit children's daily energy intake Citation58. Despite knowing about the presence of contaminants in traditional foods, a large proportion of Inuit pregnant women reported consuming high amounts of fish, beluga muktuk, seal meat, and seal fat because of the beliefs that these foods are beneficial during pregnancy Citation50. Egeland and colleague's work concerning food security among Inuit preschoolers demonstrated an urgent need for attention to this issue Citation59. They reported that approximately 70% of Inuit children lived in households rated as food insecure. Their primary care-givers reported experiencing times in the past year when their children skipped meals (76%), went hungry (90%), or did not eat for a whole day (60%). One work highlighted the complex interaction of many factors resulting in food insecurity. Beyond food affordability, factors such as budgeting, food quality and availability, absence of a full-time hunter in the household, poverty and addiction are all important considerations Citation60. Another study assessed what factors were important to community members concerning the development of chronic disease programming. The key cultural themes that emerged were perceived healthiness of country foods, food sharing, and importance of family Citation61.
Birth outcomes
Ten papers examined birth outcomes (). Genetic predisposition was proposed as an explanation for high rates of certain heart defects Citation62. A periconceptual diet higher in folate and vitamin A was recommended to reduce birth defects. Culturally appropriate public health efforts to encourage the periconceptual use of multivitamin supplements were suggested Citation53. Three papers showed that Inuit have unique risk profiles for adverse pregnancy outcomes Citation5 Citation63 Citation64. Preventing preterm births, sudden infant death syndrome (SIDS) and infection-related infant mortality were suggested as target areas for Inuit populations Citation64. Furthermore, the degree of isolation in Inuit-inhabited areas on these outcomes was considered Citation5 Citation63. Sustaining midwifery care in the North is consistent with Inuit beliefs about pregnancy and childbirth Citation65 Citation66, and literature on midwifery-led births demonstrated comparable birth outcomes to physician-led deliveries Citation67 Citation68.
Health care, policy, and human resources
Six publications related to this broad thematic area (). None of the papers presented specific policy recommendations. Of all the thematic areas included in this review, these findings varied the most. The impact of 2 infectious disease outbreaks in an arctic community highlighted the drain on health care resources caused by these events Citation69. A paper by Douglas brought attention to the need for accommodating Inuit beliefs about pregnancy in biomedical practices Citation65. A paper by Houd and colleagues based on 5 years of retrospective data advocated local birthing rather than evacuation to a larger community Citation70. Hanrahan's work documented the dissatisfaction Inuit and Innu individuals experience when using urban health centres to which they had been referred Citation71. This work, based on a large sample of interviews (n=143), summarized key areas for health care delivery improvements. A paper by Wilkins and colleagues (2008) did not address any health care challenges directly; however, they asserted that the 12-year gap in life expectancy between Inuit-inhabited areas and other Canadian regions demonstrates a dramatic disparity in health status. It was the opinion of these authors that rectifying this significant gap in life expectancy would require significant policy improvements Citation72.
Interventions and programming
Six publications had an intervention or programming component. Two papers related to birthing practices. One paper retrospectively assessed the need for community evacuation to a larger community or health centre from the small community of Inukjuak in 1998–2002 Citation70. Of 182 births, 4.5% of women or their newborns required to be evacuated for various reasons. In a larger study from 14 Inuit communities in Nunavut between 1989 and 2000, birth outcomes were not significantly different when comparing Inuit midwives to Western physicians after adjustment for maternal age, marital status, parity, education, infant sex and plurality, community size, and community-level random effects Citation67.
A pilot study was successful in demonstrating an improvement in speech intelligibility scores by using sound field amplifications in a classroom setting. With a 26% prevalence of hearing loss among Inuit children in Nunavik, this tool has potential to advantage these students Citation73. With only a 9% Inuit sample, an investigation explored the experiences of receiving HIV testing services. Overall, these youth felt they were treated with care, although there were some concerns of discrimination and hostility Citation74.
Using randomized trial approaches, the acceptability and safety of using microencapsulated-iron sprinkles for prevention of iron deficiency anaemia was assessed Citation75, and the usability of home heat recovery ventilators to reduce childhood respiratory illnesses was tested Citation40. In both analyses, the study design was effective in evaluating a chronic disease issue. Gittelsohn and colleagues did not evaluate or assess a program but discussed including the perceived healthiness of country foods, food sharing, and the importance of family Citation61. The paper is included in this section because of the applicability of the findings to developing Inuit-specific programming for community-based chronic disease prevention programs.
Social determinants of health
There were 6 papers that related to the social determinants of health (). In studies examining food security Citation59, suicidal ideation and behaviour with depression Citation76 Citation77, discussions about the social determinants of health such as family responsibilities or language led to culturally appropriate explanations. Richmond's work elaborated on the importance of social support to positive health outcomes Citation78. In a comparison of Cree, Inuit and non-Aboriginal women of Quebec, it was the Aboriginal women who, as well as experiencing a higher burden from tobacco smoking and alcohol drinking for instance, also have heavier family responsibilities Citation79. Heavier family responsibilities can cause stress, and negate personal care and wellbeing.
Tobacco
Of the 72 papers reviewed, 6 focussed primarily on tobacco (). Of these, none had a focus on youth health despite high rates of smoking in this population. Much of the tobacco-related literature focused on the relationship between tobacco (often maternal smoking during pregnancy and second-hand smoke) and lower respiratory tract infections among children Citation38 Citation39 Citation41. Mehaffey et al. demonstrated that when Inuit women did not smoke or reported smoking less than 5 cigarettes a day early in their pregnancies, the birth outcomes of their infants were equal or superior compared to other Canadian infants Citation8.
Chronic disease
Five papers demonstrated the high chronic disease burden affecting Inuit peoples in Canada (). The number of overweight children reported in the target period was higher than previously reported Citation80. Rates of respiratory conditions were found to be high, but varied by geographical location, socioeconomic status, demographic characteristics Citation81, and tobacco use. The distribution of several health conditions for Inuit populations was worse than for other Canadians and other Aboriginal populations. These health disparities contribute to the increasing gap in life expectancy between the Inuit and other Canadians Citation82.
Mental health and wellbeing
Mental health and wellbeing were the foci of 3 publications (). After compiling data from several cross-sectional surveys in Quebec, smoking, drug use, and mental disorders were more prevalent among Inuit women than other women in the province Citation79. Two papers with a youth focus dealt with suicide. With high rates of completed suicides among Inuit populations, 1 study sought to examine the characteristics of Inuit people who died by suicide in Nunavik between 1982 and 1996 using a case-control approach Citation77. Completed suicides were more likely to be male and have had a lifetime psychiatric diagnosis than controls and had more contact with health care services in the year before their death and over their lifetime. The other study used a cross-sectional methodology to assess suicidal ideation and behaviour Citation76, and found associations between higher suicidal tendencies and increased anxiety and alcohol use, but not with depression or gender. Suicidal ideation occurred more frequently among younger persons, whereas those using local native language were less likely to report a wish to die.
Genetics
Two papers were concerned with genetics (). The first found that while Inuit children had a low intake of calcium per day, calcium absorption appeared to be more efficient in children with a bb vitamin D receptor genotype. This may represent a genetic adaptation to dietary constraints in the North Citation83. The other paper with a genetic focus described the occurrence of a condition known as glycogen storage disease type III (GSD III), and had a sample size of 4 Inuit children Citation84.
Dental health
The only paper that had a dental health theme utilized data from the Nunavut Inuit Child Health Survey 2007–2008 Citation85. The paper found a high incidence of poor oral health among children. Parental rating of their child's oral and dental health was also low. Factors associated with reported caries were milk, which had a protective association, and sugar, which had a negative association.
Injury
One paper focussed on youth health and examined prevention of injury mortality Citation86. Using population-based data from the Northwest Territories, this work showed an increased risk of death from injuries among individuals with being male, having an age greater than 14, living in more remote communities, living above 66 degrees latitude, and self-identifying as Dene or Inuit.
Discussion
The agenda for the past decade of Canadian Inuit health research has not mapped well to the realities of the population's demographic, or to the prevailing health statuses, of these population groups. Overall, the peer-reviewed literature was concentrated in the areas of infectious diseases and environmental contaminants, particularly among children. These findings do not correspond with the issues and areas of concern from the perspective of Canadian Inuit organizations that are in place to represent Inuit communities across the country. These organizations emphasize the importance of understanding the social determinants of health, prevention and cessation of tobacco use, principally among expecting women, and encourage efforts towards the improvement of mental health and wellbeing, particularly of youth Citation87–Citation89.
This review documents high incidences of illness and significant public health problems, but demonstrates that there are opportunities to work on research in areas that may enhance health outcomes. We suggest that a thorough, inclusive review of non-peer reviewed literature, for instance reports by organizations and programs with a focus on Inuit health should be performed. The peer-reviewed literature does not adequately capture the social determinants of health such as socioeconomic status, educational attainment, spirituality, and community infrastructure. These are more likely captured in the non-peer reviewed literature and would be helpful in conceptualizing and developing culturally fluent programs and interventions. More regionally-led and community-driven studies could be developed based on the Inuit-specific content in the national census data and the Inuit Health Survey. Finally, advocacy organizations such as Inuit Tapiriit Kanatami (ITK), and research organizations such as the Institute of Circumpolar Health are now well positioned to work towards protecting and enhancing the health of Canada's Inuit populations in collaboration with researchers, communities, and governments.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Related Research Data
References
- Statistics Canada. Aboriginal Peoples in Canada in 2006: Inuit, Metis and First Nations, 2006 Census. Aboriginal Peoples, 2006 Census. Ottawa: Statistics Canada. 2008. Catalogue no. 97-558-XIE. 12. p.
- Environs. Urban Aboriginal Peoples Study: main report. Toronto, Canada: Environics Institute. 2010. 30. p.
- Statistics Canada. Projections of the Aboriginal populations, Canada, provinces and territories, 2001 to 2017. ; Ottawa, Canada: Statistics Canada. 2010. Catalogue no. 91-547-XIE. [cited 2012 July 12]. Available from: http://www.statcan.gc.ca/pub/89-645-x/2010001/c-g/c-g013-eng.htm.
- Bjerregaard P, Young TK, Dewailly E, Ebbesson SOE. Indigenous health in the Arctic: an overview of the circumpolar Inuit population. Scand J Public Health. 2004; 32: 390–5. 10.3402/ijch.v71i0.18383.
- Luo Z-C, Senecal S, Simonet F, Guimond E, Penney C, Wilkins R. Birth outcomes in the Inuit-inhabited areas of Canada. CMAJ. 2010; 182: 235–42. 10.3402/ijch.v71i0.18383.
- Al-Sahab B, Lanes A, Feldman M, Tamim H. Prevalence and predictors of 6-month exclusive breastfeeding among Canadian women: a national survey. BMC Pediatr. 2010; 10: 20. 10.3402/ijch.v71i0.18383.
- Lee MJ. Marihuana and tobacco use in pregnancy. Obstet Gynecol Clin North Am. 1998; 25: 65–83. 10.3402/ijch.v71i0.18383.
- Mehaffey K, Higginson A, Cowan J, Osborne GM, Arbour LT. Maternal smoking at first prenatal visit as a marker of risk for adverse pregnancy outcomes in the Qikiqtaaluk (Baffin) Region. Rural Remote Health. 2010; 10: 1484.
- Egeland GM, Faraj N, Osborne G. Cultural, socioeconomic, and health indicators among Inuit preschoolers: Nunavut Inuit Child Health Survey, 2007–2008. Rural Remote Health. 2010; 10: 1365.
- Victorino CC, Gauthier AH. The social determinants of child health: variations across health outcomes – a population-based cross-sectional analysis. BMC Pediatr. 2009; 9: 53. 10.3402/ijch.v71i0.18383.
- Statistics Canada. Aboriginal Peoples survey. Table 6–1: Inuit children aged 6 to 14 who experienced hunger and how often they experienced hunger. Ottawa, Canada: Statistics Canada; 2006. Catalogue no. 89-637-X. [cited 2012 Jul 12]. Available from: http://www.statcan.gc.ca/pub/89-637-x/2008002/tab/tab6-1-eng.htm..
- McIntyre L, Connor SK, Warren J. Child hunger in Canada: results of the 1994 National Longitudinal Survey of Children and Youth. CMAJ. 2000; 163: 961–5.
- Zukewick N. Aboriginal Peoples Survey. Inuit health and social conditions, supporting data tables. Ottawa: Statistics Canada. 2006.
- Statistics Canada. Self-rated health, by age group and sex, household population aged 12 and over, Canada, provinces, territories, health regions (June 2005 boundaries) and peer groups, every 2 years (CANSIM Table 105–0422). Ottawa: Statistics Canada. 2006. [cited 2012 July 23]. Available from: http://www4.hrsdc.gc.ca/[email protected]?iid=10..
- Statistics Canada. Aboriginal Peoples in Canada in 2006: Inuit Métis and First Nations, 2006 Census. Table 11: Number and percentage of Inuit and non-Aboriginal people living in crowded dwellings, Canada and Inuit regions, 2001 and 2006. Statistics Canada. Ottawa, 2008. Catalogue no. 89-636-x. [cited 2012 July 23]. Available from: http://www.statcan.gc.ca/pub/89-636-x/2008001/tab/tab11-eng.htm..
- Statistics Canada. Aboriginal Peoples in Canada in 2006: Inuit, Métis and First Nations, 2006 Census. Table 12: Number and percentage of Inuit and non-Aboriginal people living in dwellings requiring major repairs, Canada and Inuit regions, 2001 and 2006. Statistics Canada. Ottawa, 2008. Catalogue no. 89-636-x. [cited 2012 July 23]. Available from: http://www.statcan.gc.ca/pub/89-636-x/2008001/tab/tab12-eng.htm..
- Inuit Tapiriit Kanatami. Infant mortality among Canadian Inuit approaching Third World levels [media release]. ; 2009. [cited 2012 July 23]. Available from: http://www.itk.ca/media-release/infant-mortality-among-canadian-inuit-approaching-third-world-levels..
- Lawrence HP. Oral health interventions among Indigenous populations in Canada. Int Dent J. 2010; 60(Suppl 2): S229–34.
- Orr P. Adherence to tuberculosis care in Canadian Aboriginal populations, Part 1: definition, measurement, responsibility, barriers. Int J Circumpolar Health. 2011; 70: 113–27.
- Orr P. Adherence to tuberculosis care in Canadian Aboriginal populations, Part 2: a comprehensive approach to fostering adherent behaviour. Int J Circumpolar Health. 2011; 70: 128–40.
- Douglas V. Childbirth among the Canadian Inuit: a review of the clinical and cultural literature. Int J Circumpolar Health. 2006; 65: 117–32.
- Healey GK, Meadows LM. Inuit women's health in Nunavut, Canada: a review of the literature. Int J Circumpolar Health. 2007; 66: 199–214.
- Pauktuutit. Three decades of success: Pauktuutit health projects and accomplishments. Pauktuutit. Ottawa, 2012. [cited 2012 Apr 16]. Available from: http://pauktuutit.ca/index.php/three-decades-of-success-pauktuutit-health-projects-and-accomplishments/?lang=iu.
- Alaghehbandan R, Gates KD, MacDonald D. Hospitalization due to pneumonia among Innu, Inuit and non-Aboriginal communities, Newfoundland and Labrador, Canada. Int J Infect Dis. 2007; 11: 23–8. 10.3402/ijch.v71i0.18383.
- Dallaire F, Dewailly E, Vezina C, Muckle G, Weber J-P, Bruneau S, et al.. Effect of prenatal exposure to polychlorinated biphenyls on incidence of acute respiratory infections in preschool Inuit children. Environ Health Perspect. 2006; 114: 1301–5. 10.3402/ijch.v71i0.18383.
- Bruce MG, Deeks SL, Zulz T, Navarro C, Palacios C, Case C, et al.. Epidemiology of Haemophilus influenzae serotype a, North American Arctic, 2000–2005. Emerg Infect Dis. 2008; 14: 48–55. 10.3402/ijch.v71i0.18383.
- Hamlin-Douglas LK, Coutlee F, Roger M, Franco EL, Brassard P. Prevalence and age distribution of human papillomavirus infection in a population of Inuit women in Nunavik, Quebec. Cancer Epidemiol Biomarkers Prev. 2008; 17: 3141–9. 10.3402/ijch.v71i0.18383.
- Hamlin-Douglas LK, Coutlee F, Roger M, Hanley J, Franco EL, Brassard P. Determinants of human papillomavirus infection among Inuit women of northern Quebec, Canada. Sex Transm Dis. 2010; 37: 377–81.
- Messier V, Levesque B, Proulx JF, Rochette L, Libman MD, Ward BJ, et al.. Seroprevalence of Toxoplasma gondii among Nunavik Inuit (Canada). Zoonoses Public Health. 2009; 56: 188–97. 10.3402/ijch.v71i0.18383.
- Steenbeek A, Tyndall M, Rothenberg R, Sheps S. Determinants of sexually transmitted infections among Canadian Inuit adolescent populations. Public Health Nurs. 2006; 23: 531–4. 10.3402/ijch.v71i0.18383.
- Cole M. Youth sexual health in Nunavut: a needs-based survey of knowledge, attitudes and behaviour. Int J Circumpolar Health. 2004; 63(Suppl 2): S270–3.
- Bruneau S, Ayukawa H, Proulx JF, Baxter JD, Kost K. Longitudinal observations (1987–1997) on the prevalence of middle ear disease and associated risk factors among Inuit children of Inukjuak, Nunavik, Quebec, Canada. Int J Circumpolar Health. 2001; 60: 632–9.
- Cameron C, Dallaire F, Vezina C, Muckle G, Bruneau S, Ayotte P. Neonatal vitamin A deficiency and its impact on acute respiratory infections among preschool Inuit children. Can J Public Health. 2008; 99: 102–6.
- Dewailly E, Ayotte P, Bruneau S, Gingras S, Belles-Isles M, Roy R. Susceptibility to infections and immune status in Inuit infants exposed to organochlorines. Environ Health Perspect. 2000; 108: 205–11. 10.3402/ijch.v71i0.18383.
- Ayukawa H, Bruneau S, Proulx J-F, Macarthur J, Baxter J. Otitis media and hearing loss among 12–16-year-old Inuit of Inukjuak, Quebec, Canada. Int J Circumpolar Health. 2004; 63(Suppl 2): S312–4.
- Ayukawa H, Lejeune P, Proulx JF. Hearing screening outcomes in Inuit children in Nunavik, Quebec, Canada. Int J Circumpolar Health. 2004; 63(Suppl 2): S309–11.
- Banerji A. High rates of hospitalisation for bronchiolitis in Inuit children on Baffin Island. Int J Circumpolar Health. 2001; 60: 375–9.
- Banerji A, Bell A, Mills EL, McDonald J, Subbarao K, Stark G, et al.. Lower respiratory tract infections in Inuit infants on Baffin Island. CMAJ. 2001; 164: 1847–50.
- Banerji A, Greenberg D, White LF, Macdonald WA, Saxton A, Thomas E, et al.. Risk factors and viruses associated with hospitalization due to lower respiratory tract infections in Canadian Inuit children: a case-control study. Pediatr Infect Dis J. 2009; 28: 697–701. 10.3402/ijch.v71i0.18383.
- Kovesi T, Zaloum C, Stocco C, Fugler D, Dales RE, Ni A, et al.. Heat recovery ventilators prevent respiratory disorders in Inuit children. Indoor Air. 2009; 19: 489–99. 10.3402/ijch.v71i0.18383.
- Kovesi T, Gilbert NL, Stocco C, Fugler D, Dales RE, Guay M, et al.. Indoor air quality and the risk of lower respiratory tract infections in young Canadian Inuit children. CMAJ. 2007; 177: 155–60. 10.3402/ijch.v71i0.18383.
- Dallaire F, Dewailly E, Muckle G, Vezina C, Jacobson SW, Jacobson JL, et al.. Acute infections and environmental exposure to organochlorines in Inuit infants from Nunavik. Environ Health Perspect. 2004; 112: 1359–65. 10.3402/ijch.v71i0.18383.
- Despres C, Beuter A, Richer F, Poitras K, Veilleux A, Ayotte P, et al.. Neuromotor functions in Inuit preschool children exposed to Pb, PCBs, and Hg. Neurotoxicol Teratol. 2005; 27: 245–57. 10.3402/ijch.v71i0.18383.
- Boucher O, Bastien CH, Saint-Amour D, Dewailly E, Ayotte P, Jacobson JL, et al.. Prenatal exposure to methylmercury and PCBs affects distinct stages of information processing: an event-related potential study with Inuit children. Neurotoxicology. 2010; 31: 373–84. 10.3402/ijch.v71i0.18383.
- Fraser S, Muckle G, Despres C. The relationship between lead exposure, motor function and behaviour in Inuit preschool children. Neurotoxicol Teratol. 2006; 28: 18–27. 10.3402/ijch.v71i0.18383.
- Plusquellec P, Muckle G, Dewailly E, Ayotte P, Begin G, Desrosiers C, et al.. The relation of environmental contaminants exposure to behavioral indicators in Inuit preschoolers in Arctic Quebec. Neurotoxicology. 2010; 31: 17–25. 10.3402/ijch.v71i0.18383.
- Boucher O, Muckle G, Saint-Amour D, Dewailly E, Ayotte P, Jacobson SW, et al.. The relation of lead neurotoxicity to the event-related potential P3b component in Inuit children from arctic Quebec. Neurotoxicology. 2009; 30: 1070–7. 10.3402/ijch.v71i0.18383.
- Dewailly E, Ayotte P, Bruneau S, Lebel G, Levallois P, Weber JP. Exposure of the Inuit population of Nunavik (Arctic Quebec) to lead and mercury. Arch Environ Health. 2001; 56: 350–7. 10.3402/ijch.v71i0.18383.
- Butler Walker J, Seddon L, McMullen E, Houseman J, Tofflemire K, Corriveau A, et al.. Organochlorine levels in maternal and umbilical cord blood plasma in Arctic Canada. Sci Total Environ. 2003; 302: 27–52. 10.3402/ijch.v71i0.18383.
- Muckle G, Ayotte P, Dewailly E, Jacobson SW, Jacobson JL. Determinants of polychlorinated biphenyls and methylmercury exposure in inuit women of childbearing age. Environ Health Perspect. 2001; 109: 957–63. 10.3402/ijch.v71i0.18383.
- Dewailly E, Blanchet C, Gingras S, Lemieux S, Holub BJ. Fish consumption and blood lipids in 3 ethnic groups of Quebec (Canada). Lipids. 2003; 38: 359–65. 10.3402/ijch.v71i0.18383.
- Jacobson JL, Jacobson SW, Muckle G, Kaplan-Estrin M, Ayotte P, Dewailly E. Beneficial effects of a polyunsaturated fatty acid on infant development: evidence from the inuit of arctic Quebec. J Pediatr. 2008; 152: 356–64. 10.3402/ijch.v71i0.18383.
- Arbour L, Rupps R, MacDonald S, Forth M, Yang J, Nowdluk M, et al.. Congenital heart defects in Canadian Inuit: is more folic acid making a difference?. Alaska Med. 2007; 49(Suppl 2): S163–6.
- Berti PR, Soueida R, Kuhnlein HV. Dietary assessment of Indigenous Canadian Arctic women with a focus on pregnancy and lactation. Int J Circumpolar Health. 2008; 67: 349–62.
- Egeland GM, Berti P, Soueida R, Arbour LT, Receveur O, Kuhnlein HV. Age differences in vitamin A intake among Canadian Inuit. Can J Public Health. 2004; 95: 465–9.
- El Hayek J, Egeland G, Weiler H. Vitamin D status of Inuit preschoolers reflects season and vitamin D intake. J Nutr. 2010; 140: 1839–45. 10.3402/ijch.v71i0.18383.
- Blanchet C, Dewailly E, Ayotte P, Bruneau S, Receveur O, Holub BJ. Contribution of selected traditional and market foods to the diet of Nunavik Inuit women. Can J Diet Pract Res. 2000; 61: 50–9.
- Kuhnlein HV, Receveur O. Local cultural animal food contributes high levels of nutrients for Arctic Canadian indigenous adults and children. J Nutr. 2007; 137: 1110–4.
- Egeland GM, Pacey A, Cao Z, Sobol I. Food insecurity among Inuit preschoolers: Nunavut Inuit Child Health Survey, 2007–2008. CMAJ. 2010; 182: 243–8. 10.3402/ijch.v71i0.18383.
- Beaumier MC, Ford JD. Food insecurity among Inuit women exacerbated by socioeconomic stresses and climate change. Can J Public Health. 2010; 101: 196–201.
- Gittelsohn J, Roache C, Kratzmann M, Reid R, Ogina J, Sharma S. Participatory research for chronic disease prevention in Inuit communities. Am J Health Behav. 2010; 34: 453–64. 10.3402/ijch.v71i0.18383.
- Arbour L, Gilpin C, Millor-Roy V, Platt R, Pekeles G, Egeland GM, et al.. Heart defects and other malformations in the Inuit in Canada: a baseline study. Int J Circumpolar Health. 2004; 63: 251–66.
- Luo Z-C, Wilkins R. Degree of rural isolation and birth outcomes. Paediatr Perinat Epidemiol. 2008; 22: 341–9. 10.3402/ijch.v71i0.18383.
- Luo Z-C, Wilkins R, Platt, Robert W, Kramer MS, Fetal Infant Health Study Group of the Canadian Perinatal Surveillance, System. Risks of adverse pregnancy outcomes among Inuit and North American Indian women in Quebec, 1985–97. Paediat Perinat Epidemiol. 2004; 18: 40–50. 10.3402/ijch.v71i0.18383.
- Douglas VK. Converging epistemologies: critical issues in Canadian Inuit childbirth and pregnancy. Alaska Med. 2007; 49(Suppl 2): S209–14.
- Douglas VK. The Inuulitsivik Maternities: culturally appropriate midwifery and epistemological accommodation. Nurs Inq. 2010; 17: 111–7. 10.3402/ijch.v71i0.18383.
- Simonet F, Wilkins R, Labranche E, Smylie J, Heaman M, Martens P, et al.. Primary birthing attendants and birth outcomes in remote Inuit communities – a natural “experiment” in Nunavik, Canada. J Epidemiol Community Health. 2009; 63: 546–51. 10.3402/ijch.v71i0.18383.
- Van Wagner V, Epoo B, Nastapoka J, Harney E. Reclaiming birth, health, and community: midwifery in the Inuit villages of Nunavik, Canada. J Midwifery Womens Health. 2007; 52: 384–91. 10.3402/ijch.v71i0.18383.
- Orr P, McDonald S, Milley D, Brown R. Bronchiolitis in Inuit children from a Canadian central arctic community, 1995–1996. Int J Circumpolar Health. 2001; 60: 649–58.
- Houd S, Qinuajuak J, Epoo B. The outcome of perinatal care in Inukjuak, Nunavik, Canada 1998–2002. Int J Circumpolar Health. 2004; 63(Suppl 2): 239–41.
- Hanrahan MC. Identifying the needs of Innu and Inuit patients in urban health settings in Newfoundland and Labrador. Can J Public Health. 2002; 93: 149–52.
- Wilkins R, Uppal S, Fines P, Senecal S, Guimond E, Dion R. Life expectancy in the Inuit-inhabited areas of Canada, 1989 to 2003. Health Rep. 2008; 19: 7–19.
- Eriks-Brophy A. The benefits of sound field amplification in classrooms of Inuit students of Nunavik: a pilot project. Speech Hear Serv Sch. 2000; 4: 324–35.
- Worthington C, Jackson R, Mill J, Prentice T, Myers T, Sommerfeldt S. HIV testing experiences of Aboriginal youth in Canada: service implications. AIDS Care. 2010; 22: 1269–76. 10.3402/ijch.v71i0.18383.
- Christofides A, Schauer C, Sharieff W, Zlotkin SH. Acceptability of micronutrient sprinkles: a new food-based approach for delivering iron to First Nations and Inuit children in Northern Canada. Chronic Dis Can. 2005; 26: 114–20.
- Haggarty JM, Cernovsky Z, Bedard M, Merskey H. Suicidality in a sample of Arctic households. Suicide Life Threat Behav. 2008; 38: 699–707. 10.3402/ijch.v71i0.18383.
- Boothroyd LJ, Kirmayer LJ, Spreng S, Malus M, Hodgins S. Completed suicides among the Inuit of northern Quebec, 1982–1996: a case-control study. CMAJ. 2001; 165: 749–55.
- Richmond CAM. The social determinants of Inuit health: a focus on social support in the Canadian Arctic. Int J Circumpolar Health. 2009; 68: 471–87.
- Lavallee C, Bourgault C. The health of Cree, Inuit and southern Quebec women: similarities and differences. Can J Public Health. 2000; 91: 212–6.
- Galloway T, Young TK, Egeland GM. Emerging obesity among preschool-aged Canadian Inuit children: results from the Nunavut Inuit Child Health Survey. Int J Circumpolar Health. 2010; 69: 151–7.
- Crighton EJ, Wilson K, Senecal S. The relationship between socio-economic and geographic factors and asthma among Canada's Aboriginal populations. Int J Circumpolar Health. 2010; 69: 138–50.
- Peters PA. Causes and contributions to differences in life expectancy for Inuit Nunangat and Canada, 1994–2003. Int J Circumpolar Health. 2010; 69: 38–49.
- Sellers EAC, Sharma A, Rodd C. Adaptation of Inuit children to a low-calcium diet. [Erratum appears in CMAJ. 2003 Sep 16;169:545]. CMAJ. 2003; 168: 1141–3.
- Zimakas PJA, Rodd CJ. Glycogen storage disease type III in Inuit children. CMAJ. 2005; 172: 355–8. 10.3402/ijch.v71i0.18383.
- Pacey A, Nancarrow T, Egeland GM. Prevalence and risk factors for parental-reported oral health of Inuit preschoolers: Nunavut Inuit Child Health Survey, 2007–2008. Rural Remote Health. 2010; 10: 1368.
- Mo D. Injury mortality risk assessment and targeting the subpopulations for prevention in the Northwest Territories, Canada. Int J Circumpolar Health. 2001; 60: 391–9.
- ITK. Health indicators of Inuit Nunangat within the Canadian context 1994–1998 and 1999–2003. Ottawa, Canada: Inuit Tapiriit Kanatami. 2010. 1. p.
- NAHO. Exploring models for quality maternity care in First Nations and Inuit communities: a preliminary needs assessment: final report on findings. Ottawa, Canada: National Aboriginal Health Organization. 2006. 32. p.
- ITK. Social determinants of Inuit health in Canada: a discussion paper. Ottawa, Canada: Inuit Tapiriit Kanatami. 2007. 5. p.
- Dallaire F, Dewailly E, Vezina C, Bruneau S, Ayotte P. Portrait of outpatient visits and hospitalizations for acute infections in Nunavik preschool children. Can J Public Health. 2006; 97: 362–8.
- Dawar M, Clark M, Deeks SL, Walop W, Ahmadipour N. A fresh look at an old vaccine: does BCG have a role in 21st century Canada?. Int J Circumpolar Health. 2004; 63(Suppl 2): S230–6.
- Greenberg D, Banerji A, Friedman MG, Chiu C-H, Kahane S. High rate of Simkania negevensis among Canadian inuit infants hospitalized with lower respiratory tract infections. Scand J Infect Dis. 2003; 35: 506–8. 10.3402/ijch.v71i0.18383.
- Christofides A, Schauer C, Zlotkin SH. Iron deficiency and anemia prevalence and associated etiologic risk factors in First Nations and Inuit communities in Northern Ontario and Nunavut. Can J Public Health. 2005; 96: 304–7.
- Healey SM, Aronson KJ, Mao Y, Schlecht NF, Mery LS, Ferenczy A, et al.. Oncogenic human papillomavirus infection and cervical lesions in aboriginal women of Nunavut, Canada. Sex Transm Dis. 2001; 28: 694–700. 10.3402/ijch.v71i0.18383.
- Luo ZC, Senecal S, Simonet F, Guimond E, Penney C, Wilkins R. Birth outcomes in the Inuit-inhabited areas of Canada. CMAJ. 2010; 182: 235–42. 10.3402/ijch.v71i0.18383.
- Dallaire R, Muckle G, Dewailly E, Jacobson SW, Jacobson JL, Sandanger TM, et al.. Thyroid hormone levels of pregnant inuit women and their infants exposed to environmental contaminants. Environ Health Perspect. 2009; 117: 1014–20.
- Willows ND, Dewailly E, Gray-Donald K. Anemia and iron status in Inuit infants from northern Quebec. Can J Public Health. 2000; 91: 407–10.