
Abstract
This monograph contains the results of a study carried out by the Yakutsk Research Center for Complex Medical Problems, “Evaluating the health of the indigenous minorities of the Sakha Republic (Yakutia) and optimizing medical assistance using innovative technologies and telemedicine in indigenous settlements.” The child population was studied in 19 indigenous minority settlements, and the adult population was studied in 12 settlements.
Table of Contents
Introduction
Chapter 1. Literature Review
1.1. Current demographic trends
1.2. Morphological and physiological characteristics
1.3. Ethnic and regional disease patterns
Chapter 2. Methods and Materials
2.1. Overview of the study on children
2.2. Overview of the study on adults
Chapter 3. The State of Health of the Child Population
3.1. Demographic and health indicators
3.2. Data from clinic patients
3.3. Results of screening examinations
3.4. Physical development of the child
3.5. Blood pressure and taste sensitivity to salt
3.6. Sexual development and hormonal status
3.7. Genetic heterogeneity in non-classical 21-hydroxylase deficiency
Chapter 4. The State of Health of the Adult Population
4.1. Population trends during socio-economic transition
4.2. Major health care indicators
4.3. A profile of disease prevalence
4.4 Lipid metabolism
4.5. Social and health-related characteristics
Discussion
References
Introduction
Currently, in Russia, allocation of public health resources is highly standardized across the country, without any consideration for regional differences and ethnic-specific characteristics. Such an approach may be acceptable in European Russia, with its milder climate and relatively homogeneous population, but it is ill suited for the indigenous minority ethnic groups of Russia's Far North.
Due to its unique geography and ethnic composition, Yakutia is one of the more challenging regions in which to provide health care in Russia.
Yakutia has an area of 3,103.2 square kilometres, with a poorly developed transportation infrastructure, especially in the Far North, and a low population density. According to the Yakutia State Statistics Service (1998), the population density of the city of Yakutsk was 0.32 persons per square kilometre, while in a number of the Arctic regions, it ranged from 0.1 to 0.01 persons per square kilometre. Under these conditions, one of the most pressing public health issues is adequate provision of specialized medical care to all members of the population, regardless of location.
In 2002, the population of Yakutia was 949,300. People of Yakut ethnicity comprised 45.5% of the population, Evenks 1.9%, Evens 1.2%, Yukaghir 0.1% and Chukchi 0.1%. The northern indigenous minority peoples reside primarily in remote settlements, with poor transportation infrastructure, which understandably limits access to health care. Those who maintain a traditional lifestyle are most exposed to climate extremes. Endogamous marriages, not uncommon in remote settlements, serve to reinforce the physiological characteristics, which helped groups adapt to the environment. However, they also lead to a higher prevalence of genetic disorders. Taking transportation costs into account, health care spending is equivalent to, or even greater than, that for city populations.
There is thus a need for region-specific mechanisms for implementing government public health policies, and to improve public health services for the northern indigenous minority populations.
Chapter 1. Literature review
1.1. Current demographic trends
The social and economic reforms since the 1990s have had a negative effect on the demographic situation in the Russian Federation. Between 1987 and 2004, the birth rate in Russia fell from 17.2 to 10.5 per 1,000 population. During the same period, the mortality rate increased from 10.5 to 16.0 per 1,000 population. As a result, a significant decline in the natural rate of increase was observed over that period (from 6.7 in 1987 to 5.5 per 1,000 population in 2004). The population in Russia declined by 10,361,400 persons over that period (Citation1–Citation3).
The demographic crisis in Russia has diverted attention from the situation among northern indigenous minority populations. In recent years, the number of publications dedicated to studying population migration, mortality and births in these populations has declined. Yet these issues remain relevant. Social and economic conditions in regions inhabited by the northern indigenous minority populations have deteriorated significantly over the years since perestroika. Limited access to health care and public health resources are exacerbated by the extreme climate and the uneven settlement patterns over a large geographical area (Citation4–Citation6). Indigenous populations also play a large role in the government's efforts to exploit the North for industrial development, transportation and energy extraction (Citation7).
Evenks, Evens, Dolgans, Yukaghir and Chukchi comprise the indigenous minority groups living in Yakutia. The dying out of northern indigenous minority populations in the face of a growing non-native population has long been feared. This is connected to their small population, the high mortality rates, aggressive assimilation policies and other factors (Citation8–Citation10). This concept of the impending extinction of the indigenous minority peoples was popular in the medical establishment and often formed the conclusion when evaluating their state of health. In recent years, studies have shown that the pattern of demographic development of northern indigenous minority groups has changed significantly and is different from what statistics in previous years have shown (Citation6, Citation11–Citation13).
shows population dynamics for the indigenous minority populations of Yakutia, based on population censuses in 1989 and 2002 (Citation14, Citation15). During the period between 1989 and 2002, the indigenous minority population of Yakutia increased by 33%. The Evenk population increased by 26%; Even, 35%; and Chukchi, 27%. The Dolgan population more than tripled, while that of the Yukaghir increased by 1.6 times. Members of indigenous minority groups comprised 2.3% of the overall population in 1989, increasing to 3.5% in 2002 (Citation6, Citation12) (Citation13, Citation16).
Fig. 1.1. Change in size of indigenous minority populations in Yakutia between 1989 and 2002.
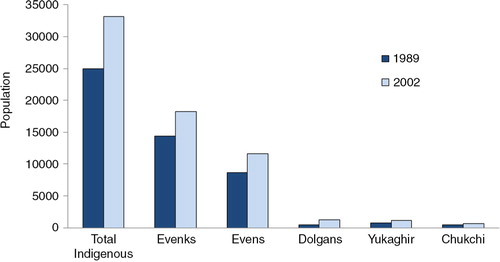
It is remarkable that such a significant increase in the indigenous minority population of Yakutia took place during this time of demographic crisis in the Russian Federation. Beginning in 1992, a population decline never before seen during peacetime was observed. Although the same trends of decreased birth rates and increased mortality were observed, the indigenous peoples of Yakutia never experienced depopulation. During the period between 1990 and 2005, the birth rate of the northern indigenous minority populations decreased by 38% (from 32.3 to 23.9 per 1,000 population). The mortality rate increased by 4% (from 9.4 to 10.1 per 1,000 population). The infant mortality rate, on the contrary, had declined from 25.6 per 1,000 live births during the 1990s to 15.3 per 1,000 live births during 2001–2005, a 40% reduction (Citation6). According to the Northern Indigenous Minority Peoples Institute of the Siberian division of the National Academy of Sciences, between 1985 and 1993, the Evenk birth rate fell by 11%, the Even birth rate by 24%, the Chukchi birth rate by 70% and the Yukaghir birth rate by 42%. Over the same period, the mortality rate in the indigenous minority populations increased by 27% collectively: 19% among Evenks, 39% among Evens, and a 3-fold increase in the Yukaghir and Dolgan populations (Citation17). Between 1990 and 2005, the average rate of natural increase of the northern indigenous minority groups decreased by 2.3 times, while remaining the highest of all ethnic groups in Yakutia. The average rate of natural increase of the minority indigenous groups was 13.8 per 1,000 population compared to 10.2 per 1,000 population for Yakuts and 2.6 per 1,000 population for the European settler population (Citation6).
A high rate of natural increase is characteristic of most northern ethnic groups. This has been noted by researchers in the past, as well as recently (Citation13, Citation18–Citation23). A high rate of natural increase over many generations speaks for this population's remarkable resilience, which can be attributed to the indigenous peoples’ legacy of self-preservation, flexibility, dynamism and aptitude for social mobility (Citation6, Citation24). One important survival tool of the indigenous minority groups is their tendency to assimilate. According to the Northern Indigenous Peoples Institute, in 1993, among the minority indigenous groups, the number of newborns with parents from different ethnic groups was between 5 and 9 times higher than in the Yakut population, and was somewhere between 52 and 92% (Citation17). According to Tyrylgin, 68% of members of the indigenous minority groups born between 1990 and 2005 had parents of different ethnicities, significantly higher than in the Yakut (16%) and settler populations (33%) (Citation6).
Yet, according to the past 2 censuses, a significant growth in the indigenous minority population has been registered in Yakutia, despite the reduction in natural increase. One important reason for this discrepancy is likely changes in record keeping. In the 1990s, the so-called nationality restoration process began. At this time, people who would previously have been considered Yakut or Russian for personal reasons or in order to better conform, including children of mixed ethnic origin, began changing their nationality to Evenk, Even and so on (Citation11, Citation24) (Citation25). According to Kuznetsov and Missonova, in the Even village of Dzhargalakh in Eveno-Bytantayskiy region, in 1991, 24 of 52 couples were of mixed ethnicity. All children born to these mixed couples were registered as Evens. An increase in the Dolgan population was in no small part due to assignment of natives of Anabarsky region to their own ethnicity, when they had formerly been considered Yakut (Citation11, Citation24).
A special demographic feature of the indigenous minority groups is their settlement over a large territory in small groups (Citation24–Citation26). The indigenous minority groups live in 79 settlements in 20 administrative regions of Yakutia (Citation27). A majority of these regions (11 of 20) are located in the Arctic. The Arctic region of Yakutia is vast and sparsely populated – the population density ranges from 0.1 to 0.3 persons per square kilometre (Citation6, Citation28). According to Tyrylgin, indigenous minorities comprise 24% of the population in Arctic Yakutia, a significantly higher proportion than in every other territorial zones of Yakutia (Citation6).
According to data from 1989 to 2002, the majority of members of indigenous minority groups lived in rural areas (Evenks – 77%; Evens – 69%; Dolgans – 88%; and Yukaghir – 61%) (Table ) (Citation6). However, over that period, an increase in city dwellers was observed in all indigenous ethnic groups, which is connected to the mass migration of the rural population to cities (Citation12, Citation13) (Citation14, Citation15) (Citation25) . Vinokurova, a long-term observer of migration patterns of the indigenous populations, reported that the greatest influx of indigenous peoples to cities occurred during the period of political and socio-economic reform (between 1985 and 1996). Vinokurova also noted an increase in young indigenous women living in cities (Citation24). The increase in migration of women of reproductive age to cities could lead to a growth in mixed marriages resulting in an increased mixed population. She considers that the urban migration contributes to increased dispersion of populations, aggravating the problem of ethnic survival (Citation24). Genetic researchers in Yakutia view migration patterns in indigenous minority groups as increasing genetic diversity in these populations, counteracting the effects of genetic drift and decreasing the risk of certain genetic disorders (Citation29, Citation30). Population studies conducted in indigenous minority settlements have shown that the smaller the ethnic group, the higher the proportion of members with genetic diseases (Citation30, Citation31).
Table 1.1. The indigenous minority populations of Yakutia by rural and urban residence, 1989 and 2002
The mass migration of indigenous women from their traditional homeland to cities results in a gender imbalance in these populations. Currently, in all groups except Evenks, the female population exceeds the male population. According to the 2002 census, in the Evenk population, for every 100 men there were 98 women (compared to 100 women in 1989). Among Evens, there were 153 women for every 100 men (an increase from 148 women in 1989); among Dolgans, 123 women (111 women in 1989); and among Yukaghir, 107 women (109 women in 1989). According to Tyrylgin, in northern indigenous populations, there are 14% fewer men than women. In the over-60 age group, there are 1.6 times more women than men (Citation6). Tyrylgin notes that women outnumber men in all major ethnic groups in Yakutia (Yakuts, Russians and indigenous minority groups). The proportion of men began to decrease in the 1990s, and this was observed to a greater extent in the older age groups (Citation28). Between 1990 and 2005, the decline in the male population was 1.5 times greater than in the female population (Citation6). This was undoubtedly connected to the high mortality rate of working-age men during the period of political and socio-economic reforms (Citation24). In 1990, the mortality rate of working-age men exceeded the mortality rate of women in the same age group by 4.2 times, falling to 3.5 times in 2004 (Citation32).
The literature emphasizes the demographic youthfulness of northern indigenous minority groups (Citation6, Citation12) Citation13, (Citation20, Citation21, Citation26, Citation33). According to the 2002 census, the median age of Evenks was 23.8 years, 24.7 years among Evens and 24.4 years among Yukaghir. Dolgans were the youngest ethnic group in Yakutia, with a median age of 18.9 years (Table ). These figures differ appreciably from those seen in the Russian Federation (37 years), the Far Eastern Federal Okrug (34 years) and Yakutia as a whole (31 years), where the population is aging. The indigenous minority groups of Yakutia had the largest proportion of the population who were children (32%) and the lowest proportion of the population who were aged 60 and older (7%). Recent studies show that the size of the northern indigenous child population continues to grow. According to Dranaeva and Burtseva, between 2005 and 2007, the absolute number of children aged 17 and younger belonging to indigenous minority groups in Yakutia increased from 9,021 to 9,414, and the number of children aged 14 and under grew from 7,433 to 7,886 (Citation23).
Table 1.2. Median age and distribution of indigenous minority populations in Yakutia by age group, 1989 and 2002
The young age structure of the indigenous minority population of Yakutia can be a positive factor for the future demographic growth of these groups. However, the demographic youthfulness of the northern indigenous ethnic groups also reflects their low life expectancy (Citation6, Citation26,Citation33), due to high mortality rates in the younger age groups, especially from causes such as trauma, poisoning, accidents, homicide and suicide (Citation22, Citation24,Citation25, Citation34–Citation38). Deaths from accidental causes are directly correlated with the prevalence of binge drinking and alcoholism (Citation33, Citation36,Citation39). Most researchers agree that it is predominantly young men who die from accidents associated with alcohol consumption (Citation24,Citation36, Citation37,Citation38, Citation40) . Average life expectancy in indigenous minority groups is between 44.7 and 54 years for men and 55.6 and 65 years for women (Citation5, Citation24).
Between the last 2 censuses, the number of marriages increased among the indigenous peoples. However, further analysis revealed some negative trends. Between 1989 and 2002, the number of people who had never been married increased in all indigenous ethnic groups. This was especially pronounced in the Even population among both men (45% increase) and women (51% increase). This is significantly higher than in Yakutia as a whole, where the number of unmarried men increased by 10% and the number of unmarried women increased by 39%. In 2002, the proportion of Even men who had never been married was 44.4%, compared with 28.8% in Yakutia as a whole. Nearly half of the over-16 male Even population had never been married, severely limiting the already limited opportunities for reproduction in such a small ethnic group. In addition, the divorce rate sharply increased among the indigenous minority populations. During the period between censuses, the number of divorces among Evenks (men and women), Evens (women) and Yukaghir (men and women) increased by more than 2 times (Citation13–Citation15).
The results of the last census showed an improvement in the education level of the indigenous minority populations (Table ). In 2002, 34% of Evenks over the age of 15 had a professional-level education (compared to 21% in 1989). For Evens, it increased from 23 to 34%, and from 26 to 38% for Yukaghir. In 2002, the proportion of individuals with basic general education and higher were 92% of Evenks, 91% of Evens, 91% of Dolgans and 92% of Yukaghir – slightly higher than in the Russian Federation as a whole (90%) (Citation14, Citation15).
Table 1.3. Education level of indigenous minority populations in Yakutia, 1989 and 2002
In summary, the following demographic trends can be identified among the indigenous minority groups in Yakutia:
Population growth in all ethnic groups
Mass migration of the rural population to cities
Young age structure
Women outnumber men
A growth in the number of never-married and divorced individuals alongside an increase in the number of married couples
Increase in education level of the population
1.2. Morphological and physiological characteristics
Exposure to the environment of the Far North is a source of stress to the human body (Citation22, Citation41–Citation43). These stressors include lengthy, cold winters; extreme variation in day length; a lower partial pressure of oxygen; windy conditions; severe drops in atmospheric pressure; and variations in geomagnetic fields (Citation22, Citation41,Citation42, Citation44,Citation45). Besides the extreme environmental conditions, the unfavourable social and economic conditions in the North have an impact on human health (Citation4, Citation6,Citation22, Citation41,Citation46).
The peoples of the North, living for thousands of years under extreme conditions, are the product of natural selection. Genes promoting survival in such an environment were selected for in this population's evolution (Citation20, Citation21,Citation45, Citation47,Citation48). The health of the indigenous Arctic populations is a result of the social and historical development of the population's life skills over many generations (Citation49). Through the course of this adaptation, certain anthropometric characteristics of the indigenous populations have emerged (Citation50, Citation51).
The northern indigenous groups share many common features, physiologically and in terms of body composition. According to Alekseeva's concept of “adaptive types,” genetically unrelated populations living in the same region under the same bioclimatic conditions share similar morphophysiological characteristics (Citation20). This concept was confirmed by the work of Veselukhin, who found significant similarities in the physiology of 3 unrelated Arctic indigenous groups – Chukchi, Evens and Yakuts (Citation52).
Based on her years of studying anthropological characteristics of Nenets, Chukchi, Inuit and Saami, Alekseeva identified an “Arctic adaptive type,” characterized by high body density, increased musculoskeletal development, increased skeletal strength, cylindrical chest shape and the near absence of individuals with an asthenic body type (Citation20). Reports in the literature about body fat deposition in northern indigenous peoples are, however, contradictory. For example, Brown, studying the body fat deposition in the Inuit of North America, proposed the role of a thicker layer of subcutaneous adipose tissue as an adaptation to cold (Citation53). Deryabin and Purundzhan have found evidence of a significantly thicker subcutaneous layer of adipose tissue in the abdomen in Yakuts (Citation54). According to Degtyareva and Guryeva, the indigenous residents of Yakutia have a significantly higher body fat content than non-natives (Citation55, Citation56). However, Ducros showed that the Inuit of Greenland have a thinner layer of adipose tissue than the Japanese, Americans and Belgians (Citation57). Similar results were obtained by Alekseeva, who found that Arctic groups had thinner adipose tissue layers than groups living in temperate or continental climates (Citation20, Citation21).
A number of researchers studying the morphology of indigenous northern populations noted the relatively high weight of Arctic indigenous peoples coupled with a shorter-than-average height (Citation20, Citation21,Citation53–Citation58). According to those researchers, adult men's weight varied between 56.3 and 63.0 kg, and women's varied between 47.3 and 52.7 kg. Body length in men was between 156.8 and 167.2 cm, and in women it was between 147.1 and 158.6 cm.
The majority of researchers studying the morphological features of northern indigenous populations noted a tendency towards mesomorphic features: high body density, short stature and well-developed musculature.
There is a considerable literature on the morphology of the northern indigenous populations at different periods of post-natal development (Citation58–Citation64). A child's physical developmental indicators are dependent on anthropologic type, formed over the course of the population's evolution under certain environmental conditions (Citation21, Citation65–Citation67). The results of studies carried out in different regions of the Far North found that anthropometric indicators of most children in the study population are consistent with norms for their age group (Citation50, Citation62,Citation68–Citation70). However, several researchers found that the anthropometric indicators of indigenous children were in the lower percentiles compared with Russian and international norms (Citation51, Citation71,Citation72). Moreover, many researchers found a significant lag in height and weight indicators in indigenous children compared with non-indigenous children in almost all age groups (Citation60, Citation61,Citation71, Citation73–Citation75). According to those researchers, the observed ethnic differences are a reflection of the way of life, sociocultural status and dietary habits.
Several studies have shown that newborn children from indigenous groups show no lag in physical development compared with non-native newborns (Citation9, Citation58,Citation59, Citation68,Citation76, Citation77). This lack of difference in height and weight indicators persists until school age, but by puberty the difference is statistically significant (Citation9, Citation51,Citation73, Citation76,Citation78). This led Chasnyk and others to propose, based on data from Khanty and Nenets children, that having spent childhood in the tundra is one of the factors determining height and weight (Citation51).
Many years of studying physical development characteristics of indigenous and non-indigenous populations in Yakutia and Taymyrsky, Evenkiysky and Yamalo-Nenetsky Autonomous Okrugs revealed significant differences in rate of sexual maturity. A majority of authors agree that sexual maturity is delayed in children from indigenous northern groups compared with settler children and children living at mid-latitudes. These studies showed that children from indigenous groups exhibit secondary sex characteristics at an older age and, in girls, later menarche (Citation61, Citation75,Citation79, Citation80).
In addition to inter-population differences, a number of intra-population differences were revealed. Among children from indigenous groups in Yakutia, differences in physical and sexual development were found based on location of residence. The further north a child lived, the lower the height and weight indicators, and the later the appearance of secondary sexual characteristics (Citation61, Citation81,Citation82).
A substantial body of literature thus exists to demonstrate the significant role of the environment in the morphological development of the peoples of the Far North. The primary anthropologic features of the indigenous population is the result of a centuries-long adaptation to the harsh conditions of the North.
Human adaptation to the extreme conditions of the North is accomplished through stress and a complex restructuring of the body's homeostasis (Citation43, Citation49,Citation83–Citation85). This involves changes in thermoregulation, in order to adapt to cold temperatures. Many researchers noted a high tolerance for cold temperatures in the indigenous groups of the Arctic and Subarctic regions – Nenets, Chukchi, Inuit and Yakuts (Citation9, Citation20,Citation21, Citation41,Citation86). Functional manifestations of adaptation to cold in the indigenous populations of the North are geared towards increasing thermoproduction and decreasing heat loss (Citation20, Citation21,Citation41). Increased thermoproduction in northern peoples occurs due to increased fat stores, increase in free fatty acids in the blood and cell membranes (Citation85, Citation87) as well as activation of lipid peroxidation processes (Citation87–Citation89). Studies have shown that the northern indigenous peoples have greater peripheral circulation and a higher rate of blood circulation in cold, compared to settlers and residents of mid-latitudes (Citation53, Citation90,Citation91). Those authors considered these characteristics to be part of the process of adaptation to cold, at the core of which is impaired vasoconstriction.
Thermoregulation processes of residents of the Far North are closely associated with energy processes, as energy expenditures are greater at higher latitudes compared with middle latitudes (Citation41, Citation90,Citation91). There have been many studies comparing metabolism in indigenous groups to settler groups (Citation20, Citation21,Citation52, Citation53,Citation90–Citation93). A majority of these studies, carried out among unrelated northern ethnic groups, found a higher energy expenditure and a greater basal metabolic rate among indigenous individuals in low temperatures (Citation53, Citation91,Citation92, Citation94). An increased basal metabolic rate was also found in the Inuit (Citation53) as well as in Yakuts, Evens and Chukchi (Citation91, Citation94). In addition, Nenets, Saami, Yakuts, Evens, Chukchi and Inuit were found to have a higher oxygen consumption compared with residents of middle latitudes (Citation20, Citation21,Citation94). The higher basal metabolic rate was more pronounced in winter than in summer. Seasonal variations in basal metabolic rate were due not only to climate but also to diet. In summer, the proportion of calories consumed from protein decreases significantly for indigenous individuals compared to the winter period (Citation94). Chukchi, Yakuts and Inuit subsisting entirely on a Western diet tended to have a lower basal metabolic rate (Citation93, Citation94), whereas Europeans subsisting on a typical northern diet were found to have an increased basal metabolic rate (Citation94).
Based on the available data on thermoregulation and basal metabolism, one can conclude that the populations of the Far North have a higher basal metabolic rate and higher energy expenditure, manifestations of their adaptation to the extreme northern climate.
The low temperature in the Far North has the greatest impact on the respiratory organs, as they have the most direct contact with the environment (Citation95). The indigenous population has lower respiratory reserves than settlers to the region. Many studies have found that forced vital capacity, reserve volume, forced expiratory volume, peak flow rate and bronchial patency are lower than in the settler population (Citation95–Citation98).
Many studies examining the structure and function of the respiratory organs of the indigenous northern populations have shown that their morphology enhances gas exchange in extreme conditions. This was found in the significantly well-developed chest (Citation20, Citation21), hypertrophy of the smooth muscle of the airways (Citation99), increased alveolar surface area and increased volume of lung microvasculature (Citation41, Citation43,Citation99–Citation102). The increased ventilation and perfusion under conditions of increased oxygen requirements were accompanied by increased smooth muscle tone in the base of the lungs, decreased patency of the bronchial tubes and increased function of the middle portion of the lungs. With this, alveolar ventilation of the lungs is not uniform, leading to regional alveolar hypoxia. As a result of these compensatory mechanisms, vascular resistance and systolic pressure of the pulmonary arteries increase, increasing the work of the right heart. These morphofunctional changes specific to high latitudes are referred to as “Northern arterial hypertension of the pulmonary circulation” or “Northern pulmonary hypertension” (Citation43, Citation101,Citation103). Avtsyn and others, based on their own observations over 10 years in the field, concluded that “Northern pulmonary hypertension” is widespread among residents of all regions of the North, regardless of ethnicity (Citation41, Citation103). They emphasized the high prevalence of pulmonary hypertension among the indigenous populations (Yakuts, Chukchi and Evens) (Citation41, Citation103). They also found that the frequency of elevated systolic pulmonary artery pressure in the indigenous population is somewhere between 25 and 80%, while it is between 15 and 56% for the settler population. The high incidence of this condition in the Arctic was confirmed by the research of Bligh and Chauca, who observed pulmonary hypertension in both humans and animals (Citation104). Sovershaeva also found this condition in a significant proportion of the indigenous population of Arkhangelsk Oblast (Citation105). A comparative analysis of the patency of the tracheo-bronchial tree, carried out on the indigenous and settler populations, showed a lower patency of the tertiary bronchi in the indigenous population, evidence of more stress on lobar and main bronchi, and an indirect indicator of congestion of the pulmonary circulation (Citation95).
Most studies on the cardiovascular system of the indigenous populations of the Far North look at issues related to arterial pressures in the various ethnic groups. Despite the numerous papers which have been published on this topic, there is no unified opinion characterizing the vascular reactions in Northern indigenous peoples. Many researchers have written about hypotension compared to Europeans in most Arctic populations: Inuit (Citation106, Citation107), Chukchi and Koryaks (Citation108, Citation109). According to these authors, the average arterial pressure in men varied between 105/70 and 115/75, and in women it was between 98/67 and 108/69 mmHg. They also noted that arterial pressure remained low, even among elderly participants. Turchinsky found that, among the indigenous Nganasan residents of Taymyr, arterial pressures were within normal ranges (123/69–125/75 mmHg) (Citation110). Similar results were obtained by Petrov and others, who noted that the average arterial pressure in indigenous residents in polar regions of Yakutia was not different from average arterial pressures in populations at middle latitudes (Citation111). Other studies showed that pulse, cardiac output, electrocardiogram amplitude and intervals were also within or better than normal ranges for northern indigenous peoples (Citation106, Citation110).
The presence of hypo- or normotensive conditions in different northern populations was extensively investigated by Argunov, who studied the structure of vessels of children and young people and found a significantly thinner intima in the aorta and coronary arteries in the indigenous population. These characteristics of vessel walls were considered by Argunov to be both genetically determined and a result of diet and lifestyle (Citation112).
The hypotension in northern indigenous populations characterized by many researchers was also observed in children. Arterial pressure studies were performed on children in Yamalo-Nenetsky and Nenetsky Autonomous Okrug (Citation51, Citation73). Nenets, Khanty, Selkup and Komi children were found to have significantly lower arterial pressures than settler children in nearly all age groups. Indigenous children exhibited hypotension far more often than hypertension (Citation51). Through these studies, indigenous children were also found to have a larger thoracic aorta diameter than settler children. Chasnyk and others carried out a study of angiotensin-converting enzyme polymorphisms in order to study a possible genetic aetiology to explain lower arterial pressure in the indigenous populations (Citation51). Nenets children were studied, and the control group was composed of children from St. Petersburg. The study showed a near-complete absence of the DD genotype in Nenets children, which is associated with hypertension (5% in Nenets children compared with 27% of European children). As a result, the authors were able to propose a possible genetic origin of the lower blood pressure in northern indigenous populations.
Most northern indigenous populations exhibit a characteristic haemodynamics, formed through the process of adapting to the harsh Arctic conditions. It can be said with great confidence that this has a genetic basis.
The physiologic adaptations of the northern indigenous peoples also have a nutritional component, due to the unique features of the indigenous diet. Scientists studying the Arctic population found a high level of protein and fat and a low level of carbohydrates in their diet (Citation20, Citation21,Citation45, Citation52,Citation86, Citation113). They emphasized the fact that no adverse effects from consuming excess protein and fat were observed during their studies (Citation20, Citation45,Citation93, Citation94,Citation114). As early as 1914, A. Krogh and M. Krogh studied the metabolic processes of Greenlandic Inuit and found adequate digestion and utilization of protein with low intake of carbohydrates (Citation114). Rodahl and Issekutz found that the Alaskan Inuit have increased urinary excretion of nitrogen, which could be considered an enzymatic adaptation aimed at deamination of excess amino acids (Citation93, Citation94). Based on her own studies, as well as the work of others on metabolism of indigenous populations, Alekseeva concluded that there are specific biological mechanisms for utilization of excess protein and fats in Arctic indigenous groups (Citation20). It is thought that the intensive digestion and utilization of proteins and fats are genetically determined (Citation33) and are the result of nutritional adaptations of indigenous populations (Citation115).
Nutritional adaptations undoubtedly influence homeostasis parameters of the indigenous populations of the North (Citation94). Studies on biochemical indicators conducted among the Saami, Nenets, Yakuts, Chukchi, Even and Inuit revealed a tendency towards elevated total serum protein levels (Citation20, Citation21,Citation45, Citation94). Mean total serum protein levels in the indigenous populations were higher than in ethnic groups living at lower latitudes (Citation20, Citation21,Citation94). An increase in certain amino acids was also observed – proline, tyrosine, phenylalanine, isoleucine and methionine (Citation116). The globulin fraction in the indigenous populations was also higher than in the European population (Citation20, Citation21,Citation94, Citation116). These characteristics of protein metabolism in the indigenous population, according to Alekseeva (Citation20, Citation21) and Petrova and others (Citation45), have adaptive implications and are evidence of their bodies’ increased protective properties.
Veselukhin also found in the serum of Yakuts, Chukchi and Evens increased levels of non-protein nitrogen (29.7 g/L, 23.96 g/L and 32.34 g/L, respectively), significantly higher than in the settler population (Citation94). Veselukhin considered these findings normal, given the increased animal protein consumption in the study population.
Many researchers consider a distinguishing feature of lipid metabolism in northern indigenous populations to be the increased activity of lipolytic enzymes breaking up exogenous fats (Citation20, Citation21,Citation45, Citation85,Citation87). Currently, it is known that the neuroendocrine system is activated in response to extreme climatic-geographic factors, stimulating lipolysis, which leads to an increase in triglycerides, free fatty acids and cholesterol in the blood and cell membranes (Citation45, Citation85,Citation87, Citation116). The effects of exposure to cold increases energy expenditures and basal metabolic rate. In addition, the lipid peroxidation process is activated – increasing cellular respiration, enzymatic activity and the quantity of reactive oxygen species (Citation87–Citation89, Citation116,Citation117). It has been established that the rate of lipid peroxidation is higher in both the indigenous and settler populations of the North than in residents of the middle latitudes (Citation89). In addition, the indigenous population of the Far North exhibited higher antioxidant activity in blood lipids, as well as a lower level of secondary products of lipid peroxidation, than in the settler population (Citation89, Citation117). Therefore, the relatively high levels of endogenous antioxidants in the indigenous populations compared with the settler population arose from adaptive processes and is indicative of their greater reserves, which evolved over the course of generations (Citation45, Citation89,Citation117).
Haemoglobin levels influence the degree of lipid peroxidation to a certain extent. Most of the groups studied in the Arctic exhibited lower haemoglobin levels than those at lower altitudes (Citation94, Citation116). It is this low level of haemoglobin which amplifies hypoxia, characteristic of people living at northern latitudes, which is another reason for metabolic processes which lead to greater free radical oxidation (Citation116).
The strength of the antioxidant system reserves which prevent free radical oxidation depends on the vitamin levels in the organism. The literature contains many studies describing vitamin deficiencies in residents of the Far North (Citation22, Citation85,Citation91, Citation108,Citation116–Citation121), including ascorbic acid (11–70%), vitamin E (18–59%) and vitamin A (9–51.5%) (Citation22, Citation116,Citation117, Citation121). Seasonal vitamin D deficiencies have also been found, due to lack of exposure to sunlight in winter in children and teenagers residing in the Far North (Citation9, Citation122).
Of particular importance in the North is ensuring adequate intake of fat-soluble vitamins. This is because vitamins E and A are components of the antioxidant system, preventing excessive activation of lipid peroxidation processes and accumulation of reactive oxygen species (Citation117, Citation123,Citation124). Boyko and others showed a pronounced deficiency in vitamin A (23% of men and 43% of women) and vitamin E (68% of men and 50% of women) in reindeer herders from indigenous minority groups (Citation117). This group was also found to have low levels of secondary products of lipid peroxidation. Comparison of data allowed the authors to propose that the low levels of vitamin E in persons with a traditional lifestyle are caused by activation processes of free radical oxidation. Sitnikova examined 108 relatively healthy Dolgans and Evenks living in the Anabarsky region of Yakutia and found deficiencies in beta carotene, vitamin A and vitamin E in the serum of most participants, which was more pronounced during winter (Citation120). In view of the deficiencies in fat-soluble vitamins in indigenous populations, these authors emphasized the necessity for measures to maintain optimal antioxidant levels in the Far North (Citation117, Citation120).
This literature review allowed us to conclude that the various ethnic groups residing the Far North share common morphophysiological characteristics, which were formed over many centuries of evolution. The role of specific environmental factors in this evolution is undisputable. Daily life in the North poses serious challenges to the human body. We can therefore conclude that a survival advantage is conferred upon those whose morphophysiological features are able to meet the demands of the extreme environment.
1.3. Ethnic and regional disease patterns
Adaptation to the conditions of the Far North involves significant stress and complex restructuring of the body's homeostatic systems (Citation22, Citation42,Citation43, Citation49,Citation83–Citation85). Processes aimed at supporting homeostasis under harsh environmental conditions are frequently so deep-rooted that they accompany structural injury and functional disturbances which create a certain pre-morbid setting for the development of chronic disease (Citation41, Citation42,Citation99, Citation108). Besides this, the effects of extreme environmental factors in the Far North are accompanied by great psychosocial pressures which surpass a person's adaptive capabilities (Citation6), Citation24 (Citation39, Citation42). Disruption of the adaptive mechanisms of the body and the destabilization of the workings of the central nervous system have the potential to cause chronic disease in a population, including indigenous northern peoples (Citation6, Citation24, Citation39, Citation42, Citation125, Citation126)
Several authors studying Arctic health have shown that non-specific pathology in the indigenous population has an asymptomatic latent period (Citation49, Citation127–Citation130). It should also be noted that comparison of these studies was not always possible since many of the studies were not conducted using standardized methods and unified evaluation criteria (Citation110, Citation131).
Researchers have been particularly interested in the prevalence of circulatory disorders in northern indigenous populations. Most experts in recent years have held the same opinion that ischaemic heart disease and hypertensive disease are rarely found in Arctic indigenous populations. This phenomenon was thought to have a genetic basis, and to be closely associated with the traditional lifestyle and diet (Citation91,Citation106, Citation107,Citation108, Citation110,Citation132, Citation133,Citation134, Citation135,Citation136, Citation137,Citation138, Citation139,Citation140) .
In the 1920s, Thomas, who studied the Inuit of Labrador and Greenland, did not record a single case of hypertension in persons over 60 years of age (Citation139). In the 1950s and 1960s, various researchers reported on the low levels of hypertension and the lack of significant increase in incidence with age in the Inuit of Alaska and Canada (Citation106, Citation107,Citation134, Citation135,Citation138, Citation141). Hypertension among Russian indigenous populations (Komi, Saami, Dolgan, Nganasan, Evenk, Chukchi, Koryak and Yakut) was also significantly rarer than among the settler population (Citation86, Citation91,Citation95, Citation108,Citation110, Citation136,Citation137).
In his 1980 monograph entitled Ischemic heart disease in the Far North, Turchinsky studied the Nganasan of Taymyr. Of 158 participants, ischaemic heart disease was found in 5, and he found no cases of hypertension. Turchinsky also reported that the prevalence of hypertension did not significantly increase with age, and the cases of ischaemic heart disease were all asymptomatic, and were only diagnosed through electrocardiography (Citation110). Other researchers in Taymyr such as Polikarpov found a low morbidity rate for ischaemic heart disease among both the Dolgans (2.72 per 1,000) and Nganasan (2.01 per 1,000) (Citation142).
Low rates of myocardial infarction were found among Inuit in Alaska by Maynard in the 1960s and 1970s (Citation135) and in Greenland by Dyerberg and Bang (Citation132). Feldman estimated that the rate of ischaemic heart disease among the Inuit of Alaska was one-tenth that in the US population as a whole (Citation133).
In the 1950s, various researchers found a low rate or near absence of atherosclerosis among the Inuit of Alaska and Canada (Citation143, Citation144). In Yakutia, Afanasyeva showed that atherosclerosis is seen significantly more often in the settler population than in the indigenous population. Furthermore, the clinical signs of atherosclerosis in the non-native population are seen 10 years earlier than in the native population (Citation86). A small number of patho-anatomical studies carried out primarily in Yakutia also showed a lower rate and degree of manifestation of atherosclerosis, as well as the decade delay found in the indigenous populations of the Far North compared to the settler population (Citation86, Citation112,Citation145–Citation147). Argunov compared the normal vasculature of children and young people in the indigenous and settler populations and found that the indigenous group had a significantly thinner intima of the aorta and coronary arteries. He concluded that these features of the arterial walls developed under the influence of genetics as well as dietary and lifestyle factors (Citation112).
The results of the majority of studies carried out among the northern populations showed a relatively low rate of vascular disease in the Arctic indigenous populations. In addition, a number of researchers have expressed the opinion that haemodynamic findings of those indigenous populations who have preserved their traditional ways should be differentiated from those consuming a more modern diet (Citation41, Citation110,Citation148, Citation149). This point of view is based on the results of multiple studies carried out comparing indigenous populations with a traditional diet and lifestyle to those with a modern lifestyle. These studies have shown that a change from a traditional lifestyle and diet gives rise to the so-called effects of acculturation – a change in the evolution-fortified haemodynamic parameters. According to a majority of these researchers, observed transformations include an increase in arterial pressure, an increase in serum cholesterol levels, and an increase in the number in the population suffering from hypertension and ischaemic heart disease among those individuals who have, for 1 reason or another, left the traditional lifestyle (Citation33, Citation106,Citation112, Citation131) Citation138, (Citation141,Citation146, Citation148–Citation153).
In recent decades, many researchers have observed an increase in circulatory disorders among the indigenous populations of the Far North (Citation39, Citation46,Citation110, Citation112,Citation146, Citation152,Citation154). The primary reason for this negative trend is metabolic de-adaptation as a result of change from the traditional diet (Citation39, Citation42,Citation46, Citation155,Citation156). Among those individuals who were compelled to stop adhering to a traditional diet, an increase in psychoemotional stress was also observed, as well as activation of the sympathetic nervous system and the hypothalamo-hypophyseal-adrenal axis, which points to significant changes in hormonal regulation of metabolism (Citation42, Citation156). Other effects of the sharp decrease in consumption of traditional foods are marked deficiencies in vitamin A and E, both fat-soluble vitamins. These vitamins are an important component of the antioxidant system and prevent excessive activation of lipid peroxidation processes (Citation42, Citation117,Citation120). It is depletion of antioxidant protection and excessive lipid peroxidation which are primary drivers in the development of hypertension and ischaemic heart disease in northern indigenous populations (Citation42, Citation89).
The data provide evidence that, through adaptive processes, the Arctic indigenous peoples evolved a circulatory system genotype that is optimal for Arctic conditions, and was protective against the development of atherosclerosis and associated ailments. However, studies in recent years have shown that the influence of modern civilization and urbanization, and a deviation from traditional lifestyle and dietary practices, has caused an increase in hypertension and ischaemic heart disease in the indigenous population.
Several studies of pulmonary problems in the Far North have found a high prevalence of respiratory disorders in northern populations, especially chronic obstructive pulmonary disease among the Inuit of Alaska and Canada (Citation98, Citation157–Citation159). This is attributable to exposure to low temperatures.
The significance of cold in the pathogenesis of pulmonary disease in Northerners is well accepted among Russian researchers (Citation42, Citation43,Citation160–Citation162). The high prevalence of respiratory disorders in residents of northern territories, regardless of ethnic origin, has been reported (Citation22, Citation42,Citation46, Citation127,Citation128, Citation131,Citation163–Citation166). It has been shown that the peak of respiratory pathology is during the winter months (Citation43, Citation160). Fluorographic diagnosis of pneumonia by Kartseva and Graschenkova among the indigenous population of the Evenkiysky and Yamalo-Nenetsky Federal Okrugs was 32.0 per 1,000 population, compared to 7 per 1,000 population among the settlers (Citation129). Kartseva and Graschenkova emphasized that a large proportion of pneumonia was found among indigenous hunters with a nomadic or semi-nomadic lifestyle.
The widespread prevalence of chronic, non-specific respiratory ailments among the population of the Far North is in large part due to the extreme climate. This fact helped Avtsyn to conclude that chronic respiratory disorders are endemic to most Arctic regions, with a significant impact on the overall morbidity patterns and rates in the population (Citation161).
Many researchers have found a high prevalence of digestive disorders in Arctic indigenous populations (Citation22, Citation39) Citation121, (Citation130,Citation167), which can also be attributed to the shift away from traditional diet and lifestyle (Citation33, Citation131,Citation151).
The morphological pattern of gastrointestinal disorders in the Far North has some specific characteristics. In the indigenous populations, these disorders are often localized to the oesophagus (Citation121, Citation168). In northern Yakutia (among Yakuts and Evens), chronic oesophagitis was found in 23–62% of the study population (Citation168, Citation169). In his dissertation, Tikhonov demonstrated that the prevalence of oesophagitis in the indigenous minority populations was 3 times higher than in the settler population (135 vs. 44 per 1,000 population) (Citation121).
In the Far North, there is a high prevalence of chronic gastritis in both the indigenous and the settler populations (Citation42, Citation121,Citation130, Citation169–Citation172). The predominant form of this disorder was atrophic gastritis (Citation42, Citation173). A significant proportion of indigenous individuals participating in the study in Yakutia were diagnosed with atrophic gastritis through endoscopy (Citation166, Citation173). In Krivoshapkin's study of 516 residents of Yakutia, 59% were diagnosed with atrophic gastritis (Citation173). In the northern coastal zone, this figure was 75%. Atrophic changes in the digestive tract were found at a rate 2 times than that of the settler population. Based on biopsies of the gastric mucosa of 544 participants with chronic gastritis, Loskutova found that the rate of chronic gastritis in indigenous populations was 2.2 times higher than in settlers (Citation174). Other studies showed that the majority of cases of atrophic gastritis had a more subtle clinical progression without clinical manifestations (Citation42, Citation173), and is a reason for delay in seeking medical attention, which has implications for the development of gastric cancer (Citation173).
Erosive gastritis and ulcerative disorders of the stomach and duodenum are diagnosed significantly more often in settlers than in the indigenous populations (Citation42, Citation121,Citation167, Citation175,Citation176). In Yakutia, the prevalence of ulcerative disorders is 4 times greater among the settler population than in the indigenous population. A similar situation was observed in Khanty-Mansiysky Okrug, where the morbidity rate in the settler population was 5.8 times higher than in the indigenous population (Citation176). There is no clear-cut explanation for such pronounced ethnic differences. It is thought that psychoemotional stresses due to the extreme environmental conditions likely play a role (Citation42).
Infectious and parasitic diseases are another important source of pathology in the Far North (Citation22, Citation46,Citation131, Citation171). The close relationship of the indigenous populations with the environment leads to a high prevalence of zoonotic diseases (Citation46, Citation128,Citation131). Opisthorchiasis is endemic in Khanty-Mansiysky and Yamalo-Nenets Okrugs. Brucellosis is endemic in Magadansky Oblast, Chukotka and Taymyr (Citation46). Alveococcosis is endemic in Koryakia and Yakutia (Citation131, Citation170,Citation177). In recent years, due to the influence of anthropogenic factors as well as climate change, a significant transformation in zoonotic infectious diseases in the Far North has been underway, evidenced by major outbreaks of certain zoonoses (Citation33, Citation178). International experts predict that as a result of global warming and the melting of permafrost, there is a high probability that new disease vectors are expanding northwards, introducing new diseases (Citation179).
An increase in tuberculosis has also been observed in the Far North of Russia in recent years (Citation5, Citation6,Citation39), Citation46 (Citation131, Citation180). The current situation is complicated by the presence of significant tuberculosis reservoirs in areas traditionally inhabited by indigenous populations (Citation131, Citation180). The high rate of tuberculosis among the indigenous minority populations is associated with the low socio-economic status of those populations (Citation5, Citation6,Citation128, Citation131,Citation180).
According to the American Association for the Study of Liver Diseases, Arctic indigenous populations are at an increased risk for contracting hepatitis B (Citation181). Studies conducted in various regions of Yakutia found that the prevalence of hepatitis B is significantly higher among Yakuts and Evenks than in the settler population (Citation182–Citation184). One of the primary reasons for this increased risk and higher morbidity rate is considered to be depressed immunoreactivity, as manifested in a low T-cell count in the majority of infected persons (Citation42, Citation183). Chronic viral hepatitis is one of the main risk factors for the development of hepatocellular carcinoma. The observed increase in hepatocellular carcinoma in recent years is due to the high rate of chronic viral hepatitis and viral hepatic cirrhosis in the population of the Far North (Citation7, Citation185–Citation187).
Malignancies have long been of interest to scholars of Arctic medicine. There is a high incidence of gastrointestinal and bladder cancers in the indigenous populations of Labrador (Citation188). An analysis of 840 cases of cancer between 1950 and 1975 in the Greenland Inuit found predominantly cancer of the oesophagus, cervix, salivary glands and nasopharynx (Citation189, Citation190). These authors also observed that a significant number of malignancies tend to be diagnosed at an advanced stage.
In northern Russia, cancer in the indigenous populations is significantly higher than in the settler populations (Citation33, Citation46,Citation168, Citation173,Citation191). However, the most pronounced differences were found in the cancer mortality rates – as much as 4 times higher in the indigenous population of Chukotka than in the settler population, 3 times higher in Khanty-Mansiysky Okrug and 2 times higher among Evenks (Citation33). The high mortality rate is associated with late diagnosis, due to a lack of oncologic services in predominantly indigenous areas.
Oesophageal and gastric cancers are endemic in most regions of the Far North (Citation46, Citation131,Citation168, Citation187,Citation192). A significantly higher incidence of oesophageal cancer was found in the indigenous populations compared to the settler populations in Yakutia (Citation168, Citation173,Citation187, Citation191), Taymyr (Citation33, Citation131) and Chukotka (Citation33, Citation46). Gastric cancer was the most common cause of oncologic morbidity and mortality in the indigenous population in Koryak Autonomous Okrug, Tyumenskaya Oblast, Chukotka and Yakutia (Citation33, Citation46,Citation131, Citation173,Citation187, Citation193). In recent decades, the rate of lung cancer has been growing. This has been the most prevalent form of cancer in Koryaks, Chukchi and Yakuts (Citation33, Citation46,Citation131). Liver and cervical cancers have also become a priority in several northern regions (Citation33, Citation186,Citation194).
Thus, the literature describes a broad geographic distribution of malignancies in the Arctic regions, predominantly in the indigenous populations, who experience higher morbidity and mortality from cancer than those in the settler population.
Many researchers believe that stress plays a strong role in the many pathologies common in the indigenous populations of the Far North (Citation4, Citation6,Citation24, Citation33,Citation39, Citation46). Indigenous populations who have adapted to extreme environmental conditions are not as well suited to the effects of man-made social and environmental factors (Citation24, Citation46). The social and economic reforms of the decades since the dissolution of the Soviet Union have led to a crisis in the traditional livelihood of indigenous minority populations, with increasing unemployment, poverty and poor living conditions affecting both their physical and mental health (Citation5, Citation6,Citation24, Citation36,Citation39).
The increase in alcoholism, depression and suicide in the indigenous populations of the Far North offers evidence of the deterioration of their psychological health (Citation5, Citation24,Citation25, Citation36,Citation38, Citation39,Citation195, Citation196). That indigenous peoples are genetically predisposed to alcoholism due to a deficiency in the enzymes that metabolize alcohol – alcohol dehydrogenase and aldehyde dehydrogenase (Citation11, Citation17,Citation197–Citation199) – is widely accepted in Russia. However, in North America, various authors (Citation200–Citation202) provided evidence that the high prevalence of alcoholism in a population is not a result of a genetic deficiency or excess of those enzymes. In his 2008 monograph, Protecting health in the Far North: Using Yakutia as an example, Tyrylgin concluded that the problem of alcoholism in the northern indigenous populations cannot be based on their genetics but rather is the result of excessive psychological stress (Citation6). Suicide is an extreme response to stress and the feeling of being in an inescapable situation. The fact that suicides happen at increasing rates in rural areas populated by indigenous peoples speaks for the extreme degree of social and psychological stress in these populations (Citation24, Citation25,Citation36, Citation38,Citation195).
The health profile of the majority of indigenous Arctic populations, regardless of ethnic or regional origin, has many common features, which attest to the influence of similar environmental conditions on health. Genetics also play a role, as natural selection has taken place over the course of centuries and millenia. Many researchers in the past were of the opinion that among Arctic natives, many of the “diseases of civilization” were rarely found. In recent years, a significant increase in circulatory and digestive disorders has been observed. This trend is closely associated with the fact that the indigenous populations are no longer living in their natural environment, and have for the most part departed from the traditional way of life and diet, while experiencing new social and environmental stress.
Chapter 2. Methods and materials
This study was carried out at the Yakutsk Medical Research Centre, which is under the Siberian Division of the Russian Academy of Sciences. It was part of a public contract from the government of Yakutia entitled “Evaluating the health of the indigenous minorities of the Sakha Republic (Yakutia) and optimizing medical assistance using innovative technologies and telemedicine in indigenous settlements” (registration number 636). It was also part of a scientific initiative entitled “Neuroimmune and endocrine mechanisms of disturbances to physical and reproductive health in children and teenagers of the Sakha Republic (Yakutia)” (registration number 004).
2.1. Overview of the study on children
The register of indigenous minority settlements in Yakutia, as defined by law of the Sakha Republic (Yakutia; 22.03.2006 330-3#673-III), includes more than 70 settlements. Since 2005, we have travelled to 19 settlements (27%) in order to examine the child population. The study population was selected from the following regions ().
Fig. 2.1. Map of study regions and settlements.

The number of children examined and the settlements where they came from are shown in Table . They total 2,991 children. A total of 1,565 children with their ethnic origin going back 3 generations were included in the database (Table ).
Table 2.1. Settlements and regions of participants in study on children
Table 2.2. Ethnic origin of participants in study on children
The children were measured according to standardized methods using a vertical metre stick with a fold-up stool. Weight was measured on a Fairbanks medical scale. Blood pressure was measured using the Korotkoff method (Citation203). These measurements were compared to a database belonging to a laboratory at the Yakutsk Medical Research Center responsible for monitoring the health of the child population.
Sensitivity to the taste of cooking salt was determined based on a modified K. Henkin method (Citation204). For this, a total of 452 children were given 12 solutions of NaCl in distilled water with concentrations between 0.0025 and 5.12%.
The Tanner method was used for evaluating stage of sexual development, with modifications by Skorodok (Citation205, Citation206). Levels of growth hormone and gonadotropic and sex hormones were evaluated in 189 children (123 boys, 66 girls) taken from a group of essentially healthy children (stage I–II of health), living in northern or Arctic regions of Yakutia (Ust-Yansky and Nizhnekolymsky regions). Of the children studied, 87 were of Yakut ethnicity, and 102 belonged to indigenous minority groups (Yukaghir, Chukchi, Even and Evenk). A thyroid panel was performed on 259 of the children (122 boys and 137 girls), who exhibited no thyroid enlargement. Cortisol levels were measured in 82 children. These tests were performed at the biochemical laboratory within the department of molecular genetics of the Yakutsk Research Center for Complex Medical Problems (headed by Dr N.R. Maksimova). Immunofluorescent assays were performed by the Viktor-2 IFA analyser using the Accu-Bing test system (USA). The following pituitary hormones were measured: thyroid-stimulating hormone (TSH), follicle-stimulating hormone (FSH), luteinizing hormone (LH) and growth hormone. In addition, free T3 and free T4, testosterone, dehydroepiandrosterone sulphate, oestradiol and progesterone were measured.
Genetic analysis was performed taking ethnic origin into consideration. In accordance with current practices, ethnic origin was determined through self-identification. These studies were approved by the ethics committee of the Yakutsk Research Center for Complex Medical Problems. The following criteria were put forth for inclusion into genetic studies: an authenticated signed participation agreement, female or male, 3–17 years of age at the beginning of the study, confirmation of birth and residence in the same region, confirmation of residence of parents in the same region and a preference for parents and children older than 5 years of age to also participate in the study. A total of 321 children participated. Allele-specific polymerized chain reaction (Citation207) was used to identify mutations in the CYP 21 –nt656g gene (“intron 2g”) and V281L (“exon 7”). Testing was performed at Mount Sinai Hospital, New York, New York, United States.
Among the team of physicians travelling to settlements were a paediatrician, a radiologist, a neurologist, an endocrinologist, a cardiologist, an otolaryngologist, a child gynaecologist, a urologist, a surgeon, an allergist and an ophthalmologist.
2.2. Overview of the study on adults
The sample was drawn from 12 settlements in 5 regions; all are officially in the register of indigenous minority settlements of Yakutia. Information was collected during 2008–2009. Also included in the sample were individuals from other ethnicities who had been permanently residing in settlements of northern indigenous groups. Between 67 and 94% of the adult population of these communities were screened.
A complete physical examination was performed on 1,324 participants. The majority were from the northern indigenous minority population – 1,001 (75.6%), including Evenks (573, 43.3%), Evens (127, 9.6%), Dolgans (232, 17.5%), Yukaghir (67, 5.1%) and Kamchadals (2, 0.2%) (Table ).
Table 2.3. Ethnic origin and place of residence of participants in study on adults
Participants’ age and sex are shown in Table . The majority of participants were women (69.6%), with significantly fewer men (30.4%). Age of study participants was between 15 and 86 years of age. The average age was 44.5 years. The majority was of working age (77.3%). The employment status of participants is shown in Table .
Table 2.4. Distribution of participants in study on adults by sex and age group
Table 2.5. Employment status of participants in study on adults
The population's health was evaluated based on screenings conducted by the following specialists: a cardiologist, a pulmonologist, a neurologist, a gastroenterologist, an otolaryngologist, an urologist, a gynaecologist, a radiologist and an endoscopist. During the screening process, diagnoses were verified through an expert group. The procedure for this included an analysis of complaints, data from the physical examination as well as data from any laboratory or other studies. Medical documentation was also examined. The physical exam included documentation of appearance, percussion, auscultation and palpation. All participants underwent electrocardiography and sonography of the abdominal cavity. When indicated, fibre-optic oesophagogastroduodenoscopy was performed with subsequent cytologic and histologic studies. Sonography of the pelvic organs, thyroid gland and breasts was also performed.
In order to screen for lipid metabolism disturbances, serum lipid studies were performed on 272 participants, from 20 to 73 years of age. The following tests were performed: total serum cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides and the atherogenic index. Calculation of the atherogenic index was carried out using the following equation: Total cholesterol (TC) - HDL cholesterol/HDL cholesterol (Citation208). The following criteria were used in making the diagnosis of dyslipidaemia: hypercholesterolaemia (TC≥5.0 mmol/L), elevated LDL (≥3.0 mmol/L), low HDL (≤1.0 mmol/L) and hypertriglyceridaemia (≥1.7 mmol/L). The degree of abnormality of the atherogenic to anti-atherogenic lipid fraction ratio (atherogenic shift) was evaluated using the atherogenic index: an atherogenic index of greater than or equal to 4 units was considered elevated. All studies were carried out using standardized methods.
Participants were asked to fill out questionnaires in order to elicit more information about their lifestyle. Four groups of questions covered living conditions, material situation, family and lifestyle. In all, 1,073 participants completed the questionnaire, ranging in age from 16 to 86. The average age was 45.9. The number and ethnic composition of the surveyed participants can be found in Table .
Table 2.6. Ethnic origin and place of residence of participants who completed questionnaire in study on adults
A database was created based on the results of the screening, containing information from the survey and data from the physical examination, laboratory and other studies, and diagnoses. In accordance with the study goals, participants were broken into general groups and sub-groups. Databases were created using Statistica for Windows 6.0. Microsoft Excel 2003 was used to calculate ratios and means, errors, confidence intervals and Pearson correlation coefficients.
Chapter 3. The state of health of the child population
3.1. Demographic and health indicators
A comparative analysis of data on morbidity in children and teenagers in Yakutia showed that the morbidity rates of most clinical illnesses in children and teenagers were higher in Yakutia than in the Russian Federation as a whole (Citation209).
Table compares the crude birth rate and infant mortality rate between Yakutia as a whole and its indigenous minority regions, as reported in official statistics. The differences between the 2 groups are small. Within Yakutia, there is regional variation. The infant mortality rate in 2006 ranged from a low of 6.3 per 1,000 in the city of Yakutsk to several times higher in indigenous minority regions such as Allaikhovsky (41 per 1,000), Anabarsky (37 per 1,000), Nizhnekolymsky (55 per 1,000) and Ust-Maysky 38 per 1,000).
Table 3.1. Selected health indicators in Yakutia, 2002–2006
The leading causes of death in children aged 1–14 years and 15–17 years were injury, including poisoning, followed by congenital malformations.
In 2006, the rate of officially registered disease cases among children aged 17 and younger was significantly higher in indigenous minority regions than in Yakutia as a whole. The highest rates were observed in the Arctic and Subarctic regions of Allaikhovsky, Nizhnekolymsky, Oymykonsky and Srednekolymsky. For children aged 14 and younger, the top 2 regions for child morbidity were Ust-Maysky and Oymykonsky regions.
A comparative analysis of data on the rate of morbidities registered in children living in northern indigenous minority regions shows that, for the majority of clinical illnesses, the rate is higher than in the Russian Federation as a whole. Such data on morbidity, however, are based on the existing official statistics, which are dependent on the population seeking medical attention. Therefore, the utility of these data is limited (Citation210). For a more detailed analysis of medical and demographic processes in the northern indigenous minority populations, the Ministry of Health of the Russian Federation is considering including in their statistical tallies a column for ethnicity. This would undoubtedly help in obtaining objective information about the state of health of northern indigenous minorities.
3.2. Data from clinic patients
We performed a retrospective analysis of the results of examinations performed on 2,385 teenagers seen at the Pediatric Center of Republican Hospital 1 in 2005–2007. Participants ranged in age from 15 to 17 years. Participants were divided in groups based on residence in 1 of 4 medical-geographic zones: the Arctic zone (10%), Vilyusk zone (16%), Central zone (69%) and Southern zone (5%). Of the total participants, 759 (32%) resided in urban areas, and 1,626 (68%) resided in rural areas.
The most common illnesses found were nervous system disorders (24%), respiratory disorders (16%) and circulatory disorders (14%) ().
Fig. 3.1. Distribution of disorders in teenagers presenting to the Pediatric Center of Republican Hospital 1.
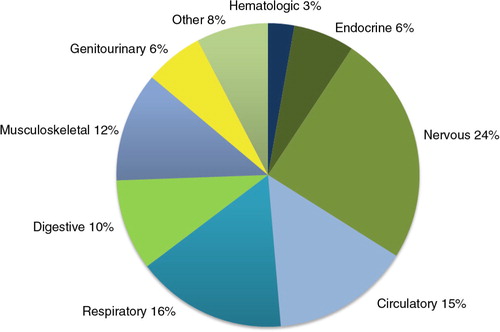
Of the nervous system disorders diagnosed, the most prevalent were encephalopathies (33%), autonomic nervous system disturbances (30%), hypoxic brain injury (17%) and epilepsy (11%). Of the respiratory disorders, 78% were in the upper respiratory tract. Of these, the most common were tonsillitis (35%); chronic rhinitis, nasopharyngitis or pharyngitis (16%); and vasomotor and allergic rhinitis (10%). The majority of circulatory disorders (56%) involved the heart, including non-rheumatic valvular defects (15%), arrhythmias (10%) and acute or chronic rheumatic disease of the heart (3%).
The distribution of the main types of illness varied significantly between the sexes. Pathologies of the nervous system, circulatory system and musculoskeletal system, as well as trauma and poisoning and other external causes, were seen significantly more often in boys than in girls. However, girls had more endocrine and urogenital disorders.
Despite differences in lifestyle and socio-economic conditions between urban and rural areas, the distribution of illnesses was very similar between teenagers living in rural and urban areas. Disorders of the genitourinary system were observed significantly more often in teenagers residing in urban areas (7.6% compared with 5.2%). On the contrary, disorders of the skin and subcutaneous tissue were observed significantly more often in teenagers residing in rural areas (4.1% compared with 1.8%), as were neoplasms (0.9% compared with 0.1%). Teenage girls living in urban areas reported disorders of the reproductive organs twice as often as did teenage girls living in rural areas (9.4% compared with 4.7%). We also found that teenagers living in rural areas had infections of the skin and subcutaneous tissue, dermatitis and eczema significantly more often than those living in urban areas (2.5% compared with 0.7%). Neoplasms were diagnosed almost exclusively in rural teenagers.
3.3. Results of screening examinations
In this section, we will present the results of the screening examinations conducted on the child population of indigenous minority settlements in northern Yakutia. The child populations of 8 regions were examined: Abyysky, Anabarsky, Allaikhovsky, Zhigansky, Ust-Yansky, Momsky,Srednekolymsky and Nizhnekolymsky. The number of participants from each region was given in Chapter 2.
We determined the prevalence of health problems in children from the different ethnic groups living in indigenous minority settlements. A detailed table is available in the appendix (Appendix Table 1).
The overall prevalence of disease in children living in indigenous minority settlements in northern Yakutia was 117 cases per 100 children examined. Among Yakut and Russian children, the rate was 131 cases per 100 children; among children from indigenous minority groups of the North, it was 108 cases per 100 children. The most prevalent diseases among children were diseases of the eye and adnexa (24 per 100 children), disorders of the respiratory system (18 per 100 children), disorders of the endocrine system and metabolism (14 per 100 children) and disorders of the genitourinary system (9 per 100 children). Among Yakut children, the most prevalent disorders were disorders of the eye and adnexa (25 per 100 children), respiratory disorders (24 per 100 children) and disorders of the endocrine system (15 per 100 children). Among Russian children, the most prevalent disorders were disorders of the eye (60 per 100 children), respiratory disorders (17 per 100 children) and disorders of the genitourinary tract (12 per 100 children). Among children from indigenous minority groups, the common disorders were that of the endocrine system (14 per 100 children), eye (21 per 100 children) and respiratory tract (15 per 100 children).
Disorders of the eye consisted predominantly of myopias of varying degrees and secondary retinal angiopathy. Disorders of the respiratory system mainly constituted disorders of the upper respiratory tract, chronic tonsillitis, adenoiditis and rhinitis. Of endocrine disorders, hypothyroidism, weight deficit, exogenous constitutive obesity and delay in puberty in teenagers were seen most often. Genitourinary disorders were predominantly urinary tract infections of non-specific aetiology, varying degrees of chronic pyelonephritis and urethritis. Many cases of disorders of the reproductive organs were also reported in children: in girls, dysmenorrhea, oligomenorrhoea and amenorrhoea; and, in boys, varicocele, hydrocele and cryptorchidism.
Our findings provide information that can be used by medical teams planning visits to remote areas to provide health care to children. Most effective would be a team including specialists in paediatrics, radiology, otolaryngology, endocrinology, neurology, nephrology, gynaecology, urology, ophthalmology and gastroenterology.
The prevalence of disease in a particular region depends on the region's current level of access to health care. For example, in the village of Saydyy, in the Momsky region, due to a lack of otolaryngology services, over several years the prevalence of ear disorders in children rose to 25 per 100 children, with all affected children having chronic otitis media.
3.4. Physical development of the child
Anthropometric studies were carried out in order to evaluate the physical development of children from indigenous minority groups of northern Yakutia. The average height and weight of Yakut boys and girls were compared to the averages for Russian, Even, Evenk, Yukaghir and Chukchi children (Table , 3.3 , 3.4 and 3.5 ).
Table 3.2. Height-for-age in Yakut, Russian, Even, Evenk, Chukchi and Yukagir boys
Table 3.3. Height-for-age in Yakut, Russian, Even, Evenk, Chukchi and Yukagir girls
Table 3.4. Weight-for-age in Yakut, Russian, Even, Evenk, Chukchi and Yukagir boys
Table 3.5. Weight-for-age in Yakut, Russian, Even, Evenk, Chukchi and Yukagir girls
As shown in Table and 3.3 , by the teenage years, the average height for Russian children exceed that of Yakuts and the other ethnic groups.
Similarly for weight, by the teenage years, Russian boys and girls are heavier than Yakuts and children of other ethnic groups (see Table and 3.5 ).
This comparison of the anthropometric characteristics of Russian and Yakut children to northern indigenous minority children confirmed the existence of ethnicity-specific differences in height and weight. There is a need for developing regional standards for indigenous and settler children, but such efforts are hampered by small numbers. More extensive surveys are needed.
3.5. Blood pressure and taste sensitivity to salt
We compared age-specific blood pressure data of Russian children, Yakut children and children from northern indigenous minority groups. The results are displayed in and .
Fig. 3.2. Mean systolic blood pressure of Russian, Yakut and indigenous minority children in selected age groups.
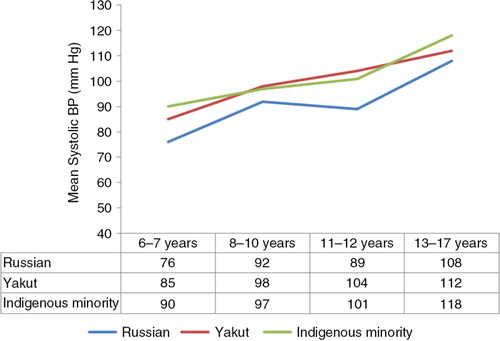
Fig. 3.3. Mean diastolic blood pressure of Russian, Yakut and indigenous minority children in selected age groups.
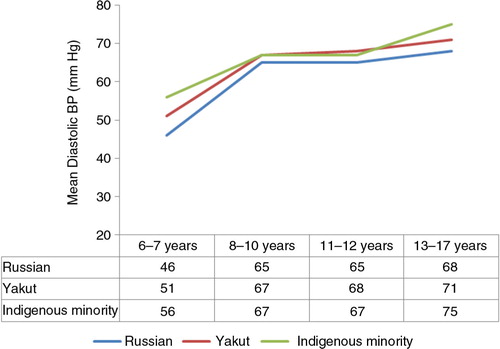
Overall, it can be seen that Russian children tend to have lower systolic and diastolic blood pressure than Yakut and indigenous minority children.
The mean threshold for taste sensitivity to cooking salt in Russians was 0.369±0.364, in Yakuts 0.627±0.547, in Evens 0.654±0.918, in Evenks 0.627±0.439, in Yukaghir 0.480±0.518, in Chukchi 0.267±0.092 and in Dolgan 1.291±1.301.
We found that Russian children had a significantly lower taste sensitivity threshold to cooking salt than Yakut, Even, Evenk and Dolgan children. Dolgan children had a significantly higher taste sensitivity threshold than Russian, Yakut, Even and Yukaghir children.
We investigated the correlation among age, height, weight, systolic and diastolic blood pressure and taste sensitivity threshold. As expected, age, anthropometric values and blood pressure are all highly intercorrlelated. We found a low correlation between height and taste sensitivity to cooking salt (r=0.15), systolic arterial pressure and taste sensitivity to cooking salt (r=0.20) and diastolic arterial pressure and taste sensitivity to cooking salt (r=0.22).
3.6. Sexual development and hormonal status
We investigated ethnic differences in endocrine function by determining hormone levels at different stages of sexual development in children of northern indigenous minority groups and those of Yakut ethnicity.
There was a significant difference in FSH and LH levels between Yakut girls and indigenous minority girls from the 10- to 14-year-old age group. The average FSH level in Yakut girls was 11.13 mIU/mL, compared to 7.39 mIU/mL in indigenous minority girls. The average LH level in Yakut girls was 14.47 mIU/mL, and it was 6.95 mIU/mL in indigenous minority girls. In Yakut girls, both FSH and LH levels were higher than in indigenous minority girls. In comparing hormone levels with the development of secondary sexual characteristics, we confirmed that Yakut girls surpassed indigenous minority girls in reproductive development. Levels of other anterior pituitary hormones (TSH and growth hormone), thyroid hormones (free T4 and free T3) and sex hormones (progesterone and oestradiol) were all within normal range, and no differences among ethnicities were found. Among boys aged 10–14 years, there were differences in FSH and progesterone levels. FSH and progesterone levels were higher in Yakut boys than in indigenous minority boys in this age group. The average FSH level in Yakut boys was 8.01 mIU/mL, and in indigenous minority boys it was 5.53 mIU/mL. In Yakut boys, the average progesterone level was 1.28 ng/mL, and in indigenous minority boys it was 0.60 ng/mL. Among Yakut and indigenous minority boys aged 14–18 years, hormone levels were within the normal range for this age group.
An analysis of average levels of pituitary hormones (TSH, FSH, LH and growth hormone), thyroid hormones (free T4 and free T3) and sex hormones (testosterone, oestradiol and progesterone) in Yakut and indigenous minority boys living in identical climate and geographical conditions showed no ethnicity-associated differences in hormone levels.
In carrying out a correlational analysis of physical and sexual development and hormone levels among indigenous girls, a significant correlation was found between testosterone level and age, height, weight, quantity of pubic hair and degree of breast development; between level of diepiandrosterone and height, weight, amount of axillary hair, amount of pubic hair and degree of breast development; and between progesterone and weight (Table ). Among boys, there was a significant correlation between testosterone level and age, height, weight, quantity of pubic hair, volume of right and left testicle and degree of sexual development on the Tanner scale. There was a negative correlation between levels of growth hormone, TSH and thyroid hormones and physical and sexual development indicators (Table ). Our results were in accordance with what is known about hormone levels and physical and sexual development from the literature.
Table 3.6. Association between physical and sexual development and hormone levels in indigenous girls
Table 3.7. Association between physical and sexual development and hormone levels in indigenous boys
According to the literature, the first sign of puberty is the appearance of LH spikes during sleep. In boys, a significant increase in LH and FSH levels signifies the second stage of sexual development. Girls in the pre-pubertal stage, as well as throughout puberty, have higher FSH levels than boys, whose FSH levels are nearly identical throughout the sexual maturation period. An appreciable increase in testosterone in boys begins between the third and fourth stages, and by the fourth stage the testosterone level increases sharply, reaching the sexually mature level. Oestrogen levels in girls begin to be higher than boys’ in the pre-puberty years. Increases in oestrogen levels are seen in boys by the second stage of sexual development. Increases in testosterone levels in girls begin in the fourth stage, according to the literature (Citation211). Until the third stage, testosterone levels in girls are low.
Indigenous populations living in their historical homeland are better at maintaining homeostasis, evidenced by intensive pituitary activity regulating the processes of sexual development. Our study showed that children from the indigenous population of Yakutia had elevated levels of gonadotropic hormones (FSH and LH). It is thought that, in indigenous children with a traditional lifestyle, adrenal cortical activity is low. In the pre-pubertal and pubertal ages, we found low levels of cortisol in girls and boys living in indigenous minority settlements where a traditional lifestyle is maintained (see Table ).
Table 3.8. Levels of thyroid hormones and cortisol in indigenous children in Yakutia
Between Yakut and indigenous minority children living in the same climate and geographic conditions, no ethnicity-related differences were found in levels of pituitary hormones (TSH, FSH, LH and growth hormone), thyroid hormones (free T3 and free T4) or sex hormones (testosterone, oestradiol and progesterone). These hormone studies confirmed that indigenous children and teenagers have adaptive mechanisms for regulating hormones in response to the extreme conditions of the Far North.
3.7. Genetic heterogeneity in non-classical 21-hydroxylase deficiency
Between 2004 and 2007, clinical and genetic studies were performed on 318 children between 3 and 17 years of age living in Pokhodsk, Chersky, Kolymsk, Andryushkino, Iengra, Neryungri, Zhigansk, Olenek and Yakutsk.
Table shows the frequency of 2 mutations responsible for classical and non-classical forms of congenital adrenal hyperplasia in children, by ethnicity.
Table 3.9. Frequency of mutations, by ethnicity
Among Evens, the mutation frequency for the classical form of congenital adrenal hyperplasia was 2.4:100. In the general population, the mutation frequency is 0.2:100. This mutation was absent in the other ethnic groups. The mutation frequency for the non-classical form of congenital adrenal hyperplasia was found most often in Yukaghir (5:100), Chukchi (4.9:100) and Evens (4.2:100). The mutation frequency in the overall population of the Far North was 2.3:100. Therefore, the mutation frequency for non-classical congenital adrenal hyperplasia is in accordance with earlier obtained data. Among the Yupik, the mutation frequency was 1.7:100 (Citation212).
We found that the mutation frequency is correlated with the size of the population of a given ethnic group (r=−0.74). In the Yukaghir, with a population of 476, the mutation frequency was 0.057. In the Chukchi, with a population of 428, the mutation rate was 0.048. In the Evens, with a population of 1,793, the mutation rate was 0.048.
With this, we found that the smaller the ethnic group, the higher the mutation frequency. Our research confirmed a higher prevalence of the non-classical form of 21-hydroxylase deficiency in children from northern indigenous minority groups compared with the Yupik living in southwestern Alaska, where the mutation frequency in the CYP21 gene was 1:60 for heterozygotes (1.7:100).
Chapter 4. The state of health of the adult population
4.1. Major population trends during socio-economic transition
Since the beginning of the 1990s, the Russian Federation has experienced depopulation and a deterioration in health status brought about by significant political and socio-economic changes. The most significant negative trends observed since this transition are a decrease in the birth rate and an increase in the mortality rate. Yakutia has also experienced similar negative shifts in demographic and health status indicators since the beginning of the 1990s. Between 1990 and 2003, the birth rate in Yakutia decreased from 19.6 to 15.0 per 1,000 population. Over this period, the mortality rate increased from 6.8 to 10.2 per 1,000 population. As a result, the rate of natural increase fell from 12.8 per 1,000 population in 1990 to 4.8 per 1,000 population in 2003. From the Federal Government Statistics Office of Yakutia, we were able to look at specific indicators for the indigenous minority populations of northern Russia in 1990, 1995 and 1999–2003. This included population size, crude birth rate, crude mortality rate and rate of natural increase.
Twenty regions of Yakutia have been designated indigenous minority areas. According to the statistics bureau, in 2003, 56,400 persons (6% of the population of Yakutia) were living in indigenous minority regions, including 21,500 in rural areas (38% of the population of these regions).
Between 1990 and 2003, the overall population of these regions decreased from 72,400 to 56,400. The rate of population decline between 1990 and 2003 was 22%. The population in indigenous minority regions as a proportion of the republic as a whole decreased from 6.5% in 1990 to 5.9% in 2003 (Table ).
Table 4.1. Total population (in thousands) in indigenous minority regions
Such a significant decrease in the population of indigenous minority regions and in Yakutia as a whole over this period is due primarily to a significant increase in emigration since the beginning of the 1990s. Before the 1990s, immigration to Yakutia was more common. Between 1990 and 2003, the regions experiencing the most emigration were in the north, including indigenous minority regions such as Ust-Yansky, Oymyakonsky, Bulunsky, Nizhnekolymsky and Verkhnekolymsky. A significant emigration of the settler population from northern regions was undoubtedly associated with the significant increase in the cost of living in the North, the closing of many businesses and the cancellation of benefits that existed previously for living in the Far North, among other reasons.
While the total population of indigenous minority regions decreased, during this period we also observed that the number of members of indigenous minority groups living in the rural areas of these regions increased by 3.7% (from 20,718 to 21,486). The population growth rate for Evens was 12%; for Dolgans was 22%; and for Yukaghir was 18% (Table ).
Table 4.2. Population of indigenous minorities living in rural areas
During the period between 1990 and 2003, the birth rate in the indigenous minority settlements fell from 23.2 to 14.1 per 1,000 population (by 39%). The rate of decline of the birth rate between 1990 and 2003 was 1.7 times higher than the average for Yakutia as a whole (24%). The mortality rate during that period increased from 8.1 to 10.6 per 1,000 population (by 31%). An especially high mortality rate over that entire period was consistently observed in the following indigenous minority regions: Allaikhovsky, Nizhnekolymsky, Ust-Maysky and Eveno-Bytantayskiy. As a result of the above trends in birth rate and death rate, the rate of natural increase declined from 15.1 per 1,000 population in 1990 to 3.5 per 1,000 population in 2003 (Table ).
Table 4.3. Birth, mortality and natural increase rate in Yakutia and indigenous minority regions
Table shows the age–sex distribution of the indigenous minority population. In 2004, the female population was greater than the male population, accounting for 51.8% of the total population. This trend was observed across all of the ethnic groups. For every 100 men, there were 104 women in Evenks; 113 in Evens; 111 in Dolgans; and 105 in Yukaghir. This trend was more pronounced in the above-working-age population. In this age category, the proportion of Evenk men was 34.2%; Evens, 31.1%; Dolgans, 34.3%; and Yukaghir, 27.6%. It should be noted that during this period, the proportion of women was also greater in the population of Yakutia as a whole, including Russians and Yakuts (Citation6).
Table 4.4. Distribution of the rural population of indigenous minorities by sex and age, as of January 1, 2004
The rural population of indigenous minority regions also has a disproportionately high proportion of children (34% vs. 26% in Yakutia as a whole in 2004). Among Evenks, this figure was 34%; among Evens, 35%; and among Yukaghir, 35%; and it was highest among the Dolgans, with 40%. The elderly population was, by contrast, a small proportion of the population, only 0.4% of the total population of indigenous minorities. In Evenks, they comprised 8.6%; Evens, 9.0%; Dolgans, 6.0%; and Yukaghir, 5.0%. This points to the relatively low number of people living to old age. As a whole, the overall demographic picture of the relatively high proportion of children and the low proportion of older adults in the indigenous minority population is consistent with the literature (Citation6, Citation26,Citation33).
4.2. Major health care indicators
During the difficult years of social and economic reform, a key issue for the Russian public health sector was improving its efficiency. Reform of the health care system in the Russian Federation consisted of decreasing the number of hospital beds, and centralization and reorganization of health care facilities and clinics. In Yakutia, between 1990 and 2005, the total number of health care facilities decreased by 20%, while the number of hospital beds decreased by 31%. Medical and obstetrics centres decreased by 25%. Over the same period, the number of doctors in all specialties increased by 2.6%, and the number of nurses decreased by 2.0% (Citation6). In this section, we examine health care for the population of indigenous minority areas, as reported to Yakutia's Federal Government Statistics Office in 1990, 1995 and 1999–2003.
Between 1990 and 2003, the number of health care institutions in the indigenous minority regions decreased from 51 to 48 (by 6%). The number of hospital beds decreased from 1,009 in 1990 to 852 in 2003 (by 16%). However, due to the decline in the population, the rate of hospital beds grew from 139 to 151 per 10,000 population (by 9%) (Table ).
Table 4.5. Number and rate of hospital beds in indigenous minority regions
Changes in the number of ambulatory clinics and medical and obstetrical centres are shown in Table , with the former showing an increase and the latter a decrease. The decrease in the number of medical and obstetrics centres was due to the creation of ambulatory clinics from former medical and obstetrics centres in 6 out of 8 regions. This reflects the centralization process carried out as a part of the restructuring of the health care system.
Table 4.6. Number of ambulatory clinics and medical and obstetrical centres in indigenous minority regions
During this period, significant changes also were observed in health care personnel. In indigenous minority regions, the number of physicians of all specialties decreased by 27% between 1990 and 2003, compared to a 0.6% decrease in Yakutia as a whole. A similar trend was observed with nurses (Table ). In 2003, the number of physicians per 10,000 population in indigenous minority regions was half that of Yakutia as a whole (24 compared with 49 per 10,000 population). The number of nurses increased by 10%, but the proportion of the honey sisters in Yakutia is 85%.
Table 4.7. Number and rate of physicians and nurses in indigenous minority settlements
The period of reform in Russia exacerbated existing disparities for the indigenous minority regions. There is a serious problem in the provision of health services to a population living in an extreme climate and poor socio-economic conditions.
4.3. A profile of disease prevalence
In this section, we compare the results of comprehensive medical examinations in 6 ethnic groups (Evenks, Evens, Dolgans, Yukaghir, Yakuts and all others), living in 5 regions of Yakutia (Anabarsky, Verkhnekolymsky, Zhigansky, Oleneksky and Ust-Maysky). Information on the number and ethnic composition of participants was given in Chapter 2. Representatives from the settler population (Russians, Ukrainians, etc.) who were residing permanently in indigenous minority regions were included in the study. This group comprised 3.5% of the population and was categorized as “others.”
Detailed breakdown of disease prevalence by categories and ethnic group is provided in Appendix Table 2 and by region in Appendix Table 3. The overall disease prevalence in the study population was 279.6 per 100 participants, or an average of 2 conditions per participant. The highest disease prevalence was among the Yukaghir (315 cases per 100 participants) and Evens (311 cases per 100 participants). The lowest disease prevalence was in the Dolgans (223 cases per 100 participants) and the settler population (226 cases per 100 participants).
The 5 most prevalent categories of diseases were diseases of the digestive (70 per 100), genitourinary (49 per 100), circulatory (48 per 100), respiratory (37 per 100) and musculoskeletal (29 per 100) systems. These 5 diseases played an important role in the health of participants in all of the ethnic groups being studied.
The Evenk and Yakut populations had similar disease patterns, among whom diseases of the circulatory system were the second most common type of disorder, whereas in the other groups it was genitourinary disorders.
Among digestive disorders, the most prevalent were chronic gastritis (53 per 100), chronic pancreatitis (48 per 100) and chronic cholecystitis (44 per 100). The prevalence of chronic gastritis was particularly high in the Yukaghir population (79 per 100). The Dolgans and the settler population had the lowest prevalence of digestive disorders.
The most common genitourinary disease, across all ethnic groups, was chronic pyelonephritis. This disorder was seen at a rate 2 times higher in Evens and Yukaghir (65 and 58 per 100, respectively) than in Evenks (33 per 100), Dolgans (34 per 100), Yakuts (38 per 100) and others (38 per 100). The Even, Yukaghir and other groups showed a higher prevalence of cystic kidney disease.
Among circulatory disorders, the most prevalent were arterial hypertension, ischaemic heart disease and cerebrovascular disorders. The highest prevalence of arterial hypertension was seen in Yakuts (42 per 100) and Evenks (41 per 100), and it was lowest among the Dolgans (25 per 100). Yakuts and Evenks had significantly higher rates of ischaemic heart disease compared with all groups except for the “other” (i.e. settler) group. Five of the ethnic groups (Evenks, Evens, Yukaghir, Yakut and settler) had similar rates of cerebrovascular disease, between 19 and 20 per 100. Dolgans had a much lower prevalence of cerebrovascular disease (9 per 100).
Chronic bronchitis was the most common respiratory disorder in the study population. The highest prevalence was found in the Yukaghir (42 per 100) and Evenks (36 per 100). The “other” group had a significantly lower prevalence of chronic bronchitis (15 per 100).
Evenks and Yakuts had similar prevalence of musculoskeletal disorders. Evens and Yukaghir had a higher prevalence of arthropathies than the others. The “other” group had the lowest prevalence of dorsopathies, and arthropathies were completely absent.
Overall, we found similarities in the pattern and prevalence of disease between the Evens and Yukaghir and also between the Evenks and Yakuts. We propose that such similarities could be due to the genetic similarities between these groups, based on the analyses of mitochondrial DNA and Y chromosomes by Fedorova (Citation213).
In terms of regional variation, we found that in Zhigansky, Oleneksky and Ust-Maysky regions, the most prevalent disorders were circulatory and musculoskeletal disorders. In Verkhnekolymsky region, digestive and genitourinary disorders predominated. Anabarsky region can be characterized by a lower overall disease prevalence compared to the other regions. It is likely that geographical and environmental conditions play a role in the regional patterns observed.
4.4. Lipid metabolism
The high prevalence of digestive and circulatory disorders found in the indigenous minority settlements would alert one to a possibly high prevalence of lipid disorders in this population. We investigated the lipid profile consisting of TC, HDL, LDL, very-low-density lipoprotein (VLDL), triglycerides and the atherogenic index. The atherogenic index (Citation207) was calculated by the formula (TC - HDL)/(HDL). The following criteria were used in making the diagnosis of dyslipidaemia: hypercholesterolaemia (total cholesterol ≥ 5.0 mmol/L), elevated LDL (≥3.0 mmol/L) and low HDL (≤1.0 mmol/L) or hypertriglyceridaemia (≥1.7 mmol/L). An atherogenic index of greater than or equal to 4 units was considered elevated.
A total of 272 participants between the ages of 20 and 73 years were studied. The average age was 43.6±9.9 years. More women (62%) than men (38%) were studied. Participants were divided by ethnicity: Evenks (51%), Evens (10%), Dolgans (13%), Yukaghir (11%), Yakuts (13%) and others (3%).
Table compares the average serum lipid concentrations among the ethnic groups separately for men and women.
Table 4.8. Mean serum lipid levels and index of atherogenicity, by ethnic group and sex (±standard deviation)
These results are consistent with findings from studies of other Arctic populations, which have shown elevated total cholesterol (Citation20, Citation21,Citation94, Citation138,Citation144). Average LDL cholesterol was above normal in all ethnic groups. Average LDL cholesterol was highest in the “other” group and lowest in the Dolgan group. Average HDL cholesterol was also within normal limits, but in the Dolgan population, especially men, a more pronounced shift towards an anti-atherogenic level was observed. Statistically significant differences were found when comparing HDL cholesterol in Dolgan men to that of men from the “other” group. No appreciable difference was observed between the study groups when comparing triglyceride levels. Evenks had the highest serum triglycerides level, and Dolgans the lowest. The tendency for the “other” group to exhibit more atherogenic lipid levels and for the Dolgan group to have anti-atherogenic levels is reaffirmed in these groups’ index of atherogenicity. The index of atherogenicity in the “other” group was the highest, and it was lowest in the Dolgan group. These differences were more pronounced among men.
In the under-50 age group, there were no significant differences in average lipid levels. Ethnicity-related differences were observed when comparing indicators in the over-50 age group. The differences were predominantly in the atherogenic-to-anti-atherogenic lipid fraction ratio. In the Dolgan population, the average level of anti-atherogenic lipids was significantly higher than in the “other” and Even populations, and the atherogenic index was significantly lower than in the “other,” Even and Yakut populations. These results are a reflection and confirmation of the previously discussed trends regarding the tendency in the Dolgan population towards higher anti-atherogenic lipid levels and lower atherogenic lipid levels.
The prevalence of lipid metabolism abnormalities in different ethnic groups is shown in Table . There was at least 1 abnormal lipid metabolism indicator in 100% of the “other” group, 96% of Evens, 86% of Evenks, 86% of Yakuts, 80% of Yukaghir and 71% of Dolgans. Hypercholesterolaemia was found in 59–77% of participants, with no statistically significant difference between ethnic groups. We found that elevated LDL cholesterol was found in all 7 participants (100%) from the “other” group. The Dolgans had a significantly lower rate of elevated LDL cholesterol (44%). In addition, the Dolgan population exhibited a significantly lower prevalence of hypoalphacholesterolaemia. The highest rates of hypoalphacholesterolaemia were in the Even (417%) and Evenk (37%) groups. The settler population had the highest rate of above-normal atherogenic index (43%).
Table 4.9. Prevalence of lipid metabolism abnormalities, by ethnicity
4.5. Social and health-related characteristics
This section presents the results of social surveys carried out in indigenous minority settlements. A total of 1,073 individuals participated in the survey. Of these, 258 were residing in Anabarsky region, 190 in Verkhnekolymsky region, 189 in Zhigansky region, 250 in Oleneksky region and 186 in Ust-Maysky region. The majority of those surveyed were of indigenous minority origin (76%) including Evenks (45%), Evens (10%), Dolgans (15%) and Yukaghir (6%). Of the respondents, 30% were men and 70% were women.
Respondents varied in age between 16 and 86 years. The average age of the male respondents was 46.2±1.5 years, and the average age of the female respondents was 45.8±1.5 years. The average age of all respondents was 45.9±1.5 years.
Appendix Table 4 summarizes several socio-economic indicators in the different regions. The proportion of pensioners in Zhigansky region (30%) was significantly higher than in the other regions. Ust-Maysky and Anabarsky regions had the greatest proportion of working individuals (66%). There was no significant difference between regions in the proportion of respondents belonging to the other employment categories.
Approximately half of the surveyed population (51%) possessed professional (higher or special secondary) education. The proportion was highest in Oleneksky region (59%) and lowest in Verkhnekolymsky region (43%). The proportion of respondents with no education was 2%, and this varied between 1.2 and 2.4% among the regions.
Significant differences between regions were found when comparing marital status. Regions with the highest proportion of married respondents were: Anabarsky (74%) and Ust-Maysky (67%). This figure was much lower in Verkhnekolymsky (61%), Zhigansky (62%) and Oleneksky (54%) regions.
There are significant gender differences in the unmarried population. The proportion of unmarried women was significantly higher than unmarried men in all regions (39% compared to 29%). This is in part attributable to the greater number of widowed women compared to men. Widowed women outnumbered men in the Ust-Maysky region by 4.3 times, in the Zhigansky region by 4.2 times, in the Verkhnekolymsky region by 3.7 times, in the Oleneksky region by 3.6 times and in the Anabarsky region by 2.8 times. With the exception of the Ust-Maysky region, the proportion of men who had never been married exceeded the proportion of women who had never been married. This difference was most pronounced in the Verkhnekolymsky region (30% compared to 14%).
In terms of family size, distinct differences in number of family members were seen by region (). In the Arctic zone (Anabarsky, Zhigansky and Oleneksky regions), there were more families with 6 or more members. In Ust-Maysky region, located in the mixed zone with a mixed ethnic composition and both agricultural and manufacturing industries, 5-member families predominated. The Verkhnekolymsky region, also located in the mixed zone, had predominantly smaller families with 2 members. This is the result of a high level of poverty and broken families among the respondents.
Fig. 4.1. Distribution of respondents by family size and region.
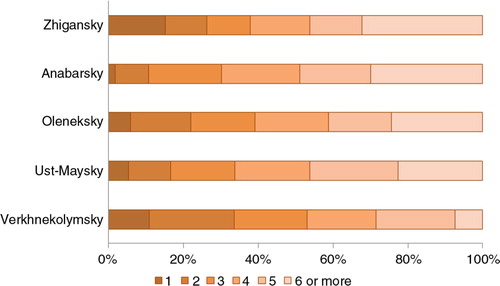
The number of children in homes is correlated with the total size of the family, and the same regional pattern is observed. The proportion of respondents with 3 or more children was around 50% in the 3 Arctic zones of Anabarsky, Zhigansky and Oleneksky. In the mixed zone, the proportion of respondents with 3 or more children was lower (37% in Verkhnekolymsky and 41% in Ust-Maysky). The regions with the greatest number of childless respondents were Verkhnekolymsky (23%) and Zhigansky (22%).
Of the 338 women of reproductive age surveyed, a mere 41% reported planning to have children in the future. Further analysis revealed that women without children were more than 2 times more likely than women with children to plan on having children in the future (66% compared to 36%). A woman's reproductive plans was not associated with education. Among women with professional education, 39% reported planning on having children in the future, while 45% of women with only general education reported planning on having children.
We investigated the possible barriers to having children. The most important factor for women in Zhigansky, Oleneksky and Ust-Maysky regions was poor health. This was the second most important factor for women in Anabarsky and Verkhnekolymsky regions. In these 2 regions, material and housing problems were the main barrier to having children. One of the most important factors preventing women from having children in Zhigansky and Ust-Maysky regions was the lack of an official marriage, which reflected the local marriage customs in those regions.
Housing conditions among respondents are summarized in Table . Overall, 42% of respondents were living in a house and 53% in an apartment. The majority of respondents were living in an apartment. An analysis of respondents’ accommodation by date built showed a decay in housing resources in indigenous minority settlements. A mere 31% of respondents were living in accommodations built after 1995. In this regard, the most favourable trends were seen in Anabarsky region, where 47% of respondents were living in homes built after 1995.
Table 4.10. Distribution of respondents by housing conditions and region
The survey showed a low number of homes with indoor amenities in the study regions. Central heating was present in 68% of the homes. The regions with the fewest respondents with central heating were Ust-Maysky (19%) and Zhigansky (45%). Running water, sewage lines and hot water were found in only 39% of respondents’ homes in Verkhnekolymsky and 14% of homes in Zhigansky region. A complete absence of indoor plumbing and hot water was found among participants living in Anabarsky, Oleneksky and Ust-Maysky regions.
This lack of indoor amenities was reflected in respondents’ own evaluation of their living conditions (). A mere 15% of respondents rated their living conditions as “good.” The greatest proportion of individuals rating their living conditions as “good” were in Anabarsky region (23%). Anabarsky region also had the lowest proportion of respondents who described their living conditions as “unsatisfactory” (23%). Due to the conditions in the villages of Kyuptsy, Ezhantsy and Petropavlovsk of Ust-Maysky region, the number of respondents rating their living conditions as “unsatisfactory” was the highest among all regions, at 43%. Among the primary reasons for respondents’ dissatisfaction with living conditions were deterioration of their residential space and lack of amenities. However, the relative importance of these factors varied by region ().
Fig. 4.2. Respondents’ evaluation of living conditions by region.
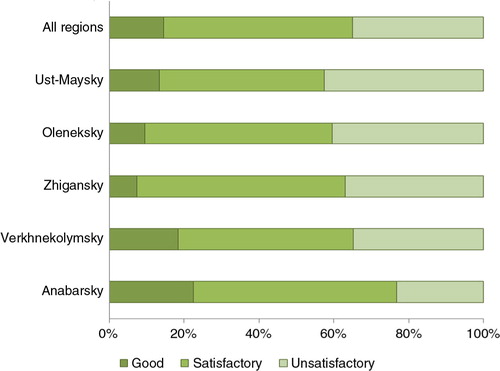
Fig. 4.3. Distribution of respondents by reason for dissatisfaction with housing, by region.
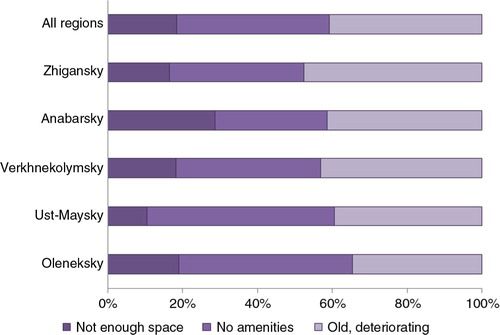
In comparing responses to questions about their material situation, no significant difference was found between regions. For nearly a quarter of all respondents in all regions, there was only enough money to buy food. For nearly one-third of respondents, there was enough to buy food and essential goods. For 4–12% of respondents, there was not enough money even for food ().
Fig. 4.4. Respondents’ evaluation of their material situation, by region.
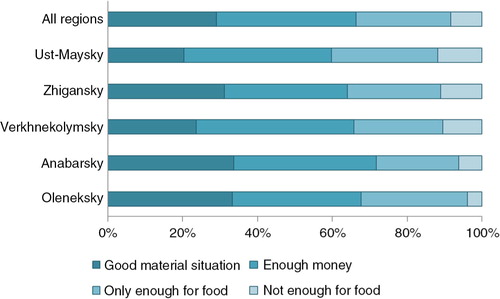
Due to the more favourable climate, environmental and socio-economic conditions in the mixed zone, the proportion of respondents with subsistence farms was significantly higher than in the Arctic zone. In the indigenous agricultural communities of Anabarsky, Zhigansky and Oleneksky regions, there was virtually no domestic farming or animal husbandry. With regard to animal husbandry, only domestic reindeer were kept by respondents in the Arctic region (Anabarsky, 21%; Zhigansky, 10%; and Oleneksky, 7%).
Among respondents, 89% characterized their way of life as settled, while 11% considered themselves as nomadic or semi-nomadic (hunters, reindeer herders and tent workers). The proportion of nomads and semi-nomads was highest in the Anabarsky and Verkhnekolymsky regions (17 and 16%, respectively). Among ethnic groups, Dolgans (45%) and Evenks (32%) had the highest reported proportion of nomads and semi-nomads.
The results of this survey allowed us to identify problems related to the marriage structure, living conditions and material situation of the surveyed population. The analysis of the marriage structure revealed a high proportion of single people, including those who were widowed and the never-married. Living conditions of the surveyed population can be characterized by deteriorating accommodations and an extremely low level of indoor amenities. The majority of the population of indigenous agricultural communities have significant material difficulties.
Discussion
An analysis of the main medical and demographic indicators of northern indigenous minority regions of Yakutia from 1990, 1995 and 1999–2003 revealed a number of negative trends in the demographic development of these regions during the period of social and economic reform: population decline, a decrease in the birth rate, an increase in the mortality rate and a decrease in natural population increase. The age–sex structure of the indigenous peoples can be currently characterized by a high proportion of children and a low proportion of individuals above working age. This is evidence of the fact that a significant proportion of the population does not live to old age. The period of reforms in Russia also had a negative impact on health care in these regions. Our analysis showed that these reforms resulted in a decrease in the number of health care institutions, medical and obstetrics centres, hospital beds and health care professionals (physicians and nurses) in these regions.
The persistence of acute socio-economic, medical and demographic problems in predominantly indigenous areas is manifested in chronic population stress, which is the main pathophysiological mechanism affecting their psychological and physical health. Based on our results, we can say that the health of the adult study population is not satisfactory. The average survey participant had 2–3 health conditions. The most common disorders were of the digestive, genitourinary, circulatory, respiratory and musculoskeletal systems.
The surveys carried out in predominantly indigenous minority regions brought a number of problems to light. These were related primarily to the marriage structure, living conditions and material situation of the surveyed population. The analysis of the marriage structure showed a large proportion of single people, including widowed and never-married individuals. Living conditions could be characterized by deteriorating housing and an extremely low level of indoor amenities. The majority of the population of indigenous agricultural communities, by their own acknowledgement, reported having significant material difficulties. Overall, we found similarities in the pattern and prevalence of disease between the Evens and Yukaghir and also between the Evenks and Yakuts. We propose that such similarities could be due to the genetic similarities between these groups.
Based on the results of our comparative analysis of the study regions, we found that the most prevalent disorders in Zhigansky, Oleneksky and Ust-Maysky regions were of the circulatory and musculoskeletal systems. The most prevalent disorders in Verkhnekolymsky region were of the digestive and genitourinary systems. Anabarsky region had the lowest disease prevalence of all study regions. The patterns discussed here are connected to the specifics of the environment – the geographic location, climate, territorial and other characteristics of the study regions.
Our analysis of lipid metabolism indicators in the adult population showed that in all ethnic groups, all indicators except total cholesterol and LDL cholesterol were within normal limits. In our opinion, the fact that total cholesterol was outside normal limits in most of the study population speaks to the necessity of creating regional standards based on the results of studies of a representative sample of northern indigenous populations. Ethnicity-specific differences were observed when comparing indicators in the over-50 age group. The differences were predominantly in the atherogenic-to-non-atherogenic lipid fraction ratios. With the exception of the Dolgan population, dyslipidaemia in the different ethnic groups was atherogenic. The Dolgan population was distinct in the predominantly anti-atherogenic fractions in the majority of the population.
Our comparative analysis of official disease statistics showed that for the majority of clinical disorders, the morbidity in children in indigenous minority regions was higher than in Yakutia and the Russian Federation as a whole. Because these official statistics are dependent on presentation to health care facilities, this is invariably understated. For a more detailed analysis of medical and demographic processes in the northern indigenous minority populations, a column for ethnicity should be included in statistical tallies. This will help in collecting more objective information about the health status of ethnic minorities.
The results of our analysis of morbidity in teenagers, based on data collected from the paediatric centre, allowed us to conclude that among the teenage study population, the most prevalent disorders were diseases of the nervous, respiratory and circulatory systems. However, the disease patterns in teenagers differed based on region of residence. Endocrine disorders were seen most often in children living in Arctic and central zones of Yakutia. The health of teenagers is significantly affected by the specifics of his or her environment, and different approaches to diagnosis are required for different regions.
Through the course of their adaptation to the harsh climate of the Far North, the indigenous populations likely acquired certain unique anthropometric features. Our comparison of height, weight and arterial pressures of indigenous minority children and Yakut children revealed differences in height and weight between the 2 groups. This points to the need for regional height and weight standards for children.
It is widely accepted that there are ethnicity-associated differences in endocrine function. Our analysis of pituitary hormones (TSH, FSH, LH and growth hormone), thyroid hormones (free T3 and free T4) and sex hormones (testosterone, oestradiol and progesterone) in Yakut and indigenous minority children exposed to the same environmental conditions did not reveal any differences between the 2 groups. We found that children from the indigenous groups had high levels of gonadotropic hormones (FSH and LH). We also found low levels of cortisol in girls and boys living in indigenous minority settlements in the pre-pubertal and pubertal ages. Our study of hormone levels showed that children and teenagers from the indigenous populations of Yakutia have developed adaptive mechanisms for hormone regulation to cope with the extreme conditions of the North.
Isolation of the population is one of the most important factors contributing to the prevalence of non-lethal genetic disorders in Yakutia. We found that the frequency of the V281L mutation in our study population was 2.4:100, with a higher mutation frequency in Chukchi (5.1:100) and Yukaghir (5:100). A moderate association was found between the mutation frequency and number of individuals in the ethnic group.
Appendix Table 1. Rates of illness (per 100 children examined) by diagnostic category and ethnicity among children from indigenous minority settlements of northern Yakutia
The government order under which this project was conducted was a social project. The Yakutsk Research Center for Complex Medical Problems managed to bring qualified medical assistance to 28 communities, for which they were very grateful.
Appendix Table 2. Prevalence (per 100 examined) of diseases by category and ethnic group
A small network of village first-aid stations exist to aid in the provision of health care to these sparsely populated regions. These stations are staffed by an internist or paediatrician or often just a medical assistant or nurse. As a result, the population is often compelled to travel to the regional centre for many types of medical care. Indeed, half of all trips out of the indigenous minority settlements are for seeking some sort of medical care. One of the most pressing problems for public health in the Far North is how to protect the health of a population living in such remote, harsh conditions, with poor transportation infrastructure.
Appendix Table 3. Prevalence (per 100 examined) of diseases by category and region
In recent years, the idea of using mobile medical clinics in these areas of low population density has been discussed more and more. In Yamalo-Nenets Okrug, for example, there have been mobile medical units equipped for winter, water and off-road conditions. The Adaptation Medical Engineering Center has become involved in development of such mobile clinics. They have developed and launched 3 types of mobile medical clinics: asphalt based; together with the Vektor manufacturing company, van based; and, together with the Shumerlinsky factory, clinics for desert-like conditions.
Appendix Table 4. Distribution of respondents by selected socio-economic indicators and region
For Yakutia, the most effective option would be a mobile clinic comprising all of the functions of a traditional clinic. The legal aspect of this endeavour is extremely important: (a) strengthening the relationship of the mobile clinic with the responsible institution, (b) ensuring staffing in accordance with the number of patients expected and (c) establishing a rotation for staff.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
References
- Schepin OP, Tishuk EA. [Medico-demographic problems in the Russian Federation]. Vestn Ross Akad Med Nauk. 2005;9:3–6. [in Russian].
- Natural movement of the Russian population: a statistical bulletin. 2005; Moscow. 25.
- Birth and mortality rates in the Russian Federation: a statistical bulletin. 2005; Moscow.
- Solomatina TV, Kapilevich LV. Organization of medical assistance to residents of remote regions of northern Siberia. Public Health Russ Fed. 2002; 5: 26–8.
- Makarova UE. [Problems with the medico-demographic situation and health care delivery in indigenous minority settlements in northern Sakha Republic (Yakutia)]. Yakutsky Med Zhurnal. 2008; 2: 33–7. [in Russian].
- Tyrylgin MA. Protecting health in the Far North: using Yakutia as an example. 2008; Novosibirsk: Nauka.
- Tikhonov DG. The indigenous population of the Arctic. Past, present and future. Yakutsk Med J. 2006; 4: 36–40.
- Chikin SY, Cheknev BM. Protecting the health of the Northern populations. 1974; Moscow: Meditsina. 231.
- Bisyarina VP, Rapoport ZZ, Maltsyev PV, Minyaylo EK. Child health in the North. 1978; Moscow: Meditsina. 152.
- Yagya NS, Petrov PA, Yagya VS. Protecting a person's health in the North. 1984; Moscow: Meditsina.
- Gorokhov SN. Ethnodemographic processes in the indigenous minority populations of Yakutia. Seventy years of the USSR Academy of Sciences in the Yakut Republic and indigenous minority populations. 1995; Yakutsk 72–8.
- Uvarova TE, Burtseva TE, Dranaeva GG, Samsonova MI, Tomsky MI. An analysis of government reporting on medical-demographic indicators and the state of health of the indigenous minority populations of the Sakha Republic (Yakutia). Health of children of the North. 2008; Yakutsk42–7.
- Burtseva TE, Uvarova TE, Makharova NV, Tomsky MI. [Dynamics of demographic and medical processes in the indigenous minority peoples of northern Sakha Republic (Yakutia)]. Dalnevost Med Zhurnal. 2008; 2 112–15. [in Russian].
- Ethnic composition of the Yakut SSR. Results of the all-union census of 1989: a compilation of statistics. 1990; Yakutsk
- Ethnic composition, languages, citizenship of the population of the Sakha Republic (Yakutia). Results of the all-Russia 2002 census: a statistical collection. 2005; Yakutsk
- Statistics: a look to the next 100 years. 375 years of Yakutia in Russia. 2008; Yakutsk: Ofset. 576.
- The indigenous peoples of Northern Sakha Republic (Yakutia): an informational booklet. 1994; Yakutsk
- Patkanov SK. On the growth of the indigenous population of Siberia. 1911; St. Petersburg. 210.
- Lantis M, Anderson R. [Demographic, social and environmental factors in polar regions]. Tetradi obschestva zdravookhraneniya. 1964; 18: 12–15. [in Russian].
- Alekseeva TI. The geographic environment and human biology. 1977; Moscow: Mysl.
- Alekseeva TI. Adaptive processes in the human population. 1986; Moscow: Moscow State University Press. 215.
- Potapov AI, Istomin AV, Shushkova TS, Ustyushin BV, Yudina TV, Maymulov VG, etal. [Challenges to preserving population health in extreme northern conditions]. Vestn Ross Akad Med Nauk. 2005; 3: 19–23. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract] [in Russian].
- Dranaeva GG, Burtseva TE. Primary demographic trends in the child population of indigenous minority groups. Children's health in the North. 2008; Yakutsk 24–6.
- Vinokurova LI. Aboriginal ethnicities of the Sakha Republic (Yakutia) in modern society. Ethnosocial development in the Sakha Republic (Yakutia): potential, trends, prospects. 2000; Novosibirsk: Nauka. 163–88.
- Borisov MN. Small-numbered ethnic groups of the North: yesterday, today and tomorrow. 1995; Rybinsk 155.
- Puzyrev VP. [The gene pool in Northern populations. Genetic processes in populations and population health]. Vestn Ross Akad Med Nauk. 1993; 8: 25–31. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract] [in Russian].
- On a register for Northern indigenous minority settlements. 1993; Moscow
- Ignatyeva VB. The population of the Sakha Republic (Yakutia): dynamics of modern demographic processes. Ethnosocial development in the Sakha Republic (Yakutia): potential, trends, prospects. 2000; Novosibirsk: Nauka. 163–88.
- Danilova AL, Sukhomyasova AL, Nikolaeva IA, Gurinova EE, Maksimova NR. Genetic and demographic features of the indigenous population of Yakutia. Children's health in the North. 2008; Yakutsk 70–2.
- Chasnyk VG, Kaminsky M, Yakovleva SY, Burtseva TE. Medico-demographic principles and general approaches to modeling the prevalence of genetic disease in the child population of the Sakha Republic (Yakutia). Health of children in the North. 2008; Yakutsk 50–3.
- Yakovleva SY, Burtseva TE, Tomsky MI, Danilova GI, Chasnyk VG, Nikolaeva LA, etal. [Congenital adrenal dysfunction in the children of Yakutia]. Yakutsky Med Zhurnal. 2008; 2: 4–6. [in Russian].
- The demographic situation in the Sakha Republic (Yakutia). 2006; Yakutia: Statistics Bureau.
- Vasilyev NV, Pisareva LF, Podoplekin VD. Prevalence of oncologic disease in the indigenous minority populations of Siberia and the Far East. 1992; Tomsk: Tomsk University Press. 115.
- Kraus RF. Violent death in Alaska. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 283–4.
- Pakhomov YE. The health of Northern indigenous minorities. Indigenous minorities in Northern Yakutia: status and problems, a collection of scientific works. 1983; Yakutsk 88–9.
- Shadrin FE. On the health of the indigenous minorities in Yakutia. Current issues regarding the health of the population of the Sakha Republic (Yakutia). 1994; Yakutsk 51–2. 2nd ed.
- Shadrin FE. On the health of indigenous minority populations of Yakutia. Seventy years of the USSR Academy of Sciences in the Yakut Republic and indigenous minorities of the North. 1995; Yakutsk 59–60.
- Wakefield D. Alcoholism: how serious? Protecting the genetic pool of Northern populations. 1995; Yakutsk 93–4.
- Protopopova RN, Krivoshapkin VG. Dependence of the health of the northern indigenous minorities on lifestyle and the environment. Nauka i Obrazovanie. 2003; 1: 46–9. [in Russian].
- Potapov AI. [Social and health issues related to protecting the population's health and the environment in Siberia and the Far East]. Byul CO AMN SSSR. 1987; 6: 9–14. [in Russian].
- Avtsyn AP, Zhavoronkov AA, Marachev AG, Milovanov AP. Pathology of residents of the North. 1985; Moscow: Meditsina.
- Khasnulin VI. Introduction to Arctic medicine. 1998; Novosibirsk: Nauka. 337.
- Milovanov AP. Adaptations of the pulmonary vascular system in the North. 1981; Novosibirsk: Nauka. 172.
- Lopatina EB, Chubukov LA, Shvareva YN. Climate and environmental differentiation of USSR regions by living conditions. Man and climate. 1972; Moscow: Mysl. 101–9.
- Petrova PG, Kulberg AY, Volozhin AI, Zakharova FA. Population health and the environment in the Sakha Republic (Yakutia): a methodological manual. 1995; Moscow: Ministry of Health of the Russian Federation.
- Chernykha AD. Social, hygienic and environmental factors impacting the health of the population of the northeastern USSR. 1989; Magadan 206.
- Altukhov YP, Korochkin LI, Rychkov YG. [Inherited biochemical variations in the process of evolution and individual development]. Genetika + . 1996; 32: 1450–75. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract] [in Russian].
- Stinson A. Growth variation: biological and cultural factors. Human biology: an evolutionary and biocultural perspective. 2000; New York: Wiley. 424–64.
- Kaznacheev VP. Current aspects of adaptation. 1980; Novosibirsk: Nauka. 190.
- Burtseva TE, Sinelnikova EV, Avrusin SL. Ethnic and enivronmental basis for the development of the health of the child population. Children's health in the North. 2008; Yakutsk 64–5.
- Chasnyk VG, Sinelnikova EV, Burtseva TE, Avrusin SL, Tomsky MI, Nikolaeva LA, etal. Ethnic- and regional basis for normal child development in the Far North. 2008; 197.
- Veselukhin RV. [Physiological characteristics of the adaptive type of the indigenous populations of the Arctic and continental zones of northeastern Asia]. Vopr Antropol. 1977; 56: 26–9. [in Russian].
- Brown GM. Vascular physiology of the Eskimo. Rev Can Biol. 1957; 16: 279–92. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract].
- Deryabin VE, Purundzhan AL. Geography-specific features of body composition in the USSR population. 1990; Moscow: State University Press. 192.
- Degtyareva TG. Physical health indicators in the male population of the Sakha Republic (Yakutia). Issues related to human health and pathology in the North: facts, problems and prospects. 2002; Yakutsk 21–2.
- Guryeva AB. Anthropometric features of the women of Sakha Republic (Yakutia). Issues related to human health and pathology in the North: facts, problems and prospects. 2002; Yakutsk 306–7.
- Ducros A. Adiposite et densite corporelle d'une population arctique (eskimo ammasalimiut). Anthropologie. 1971; 75: 48–59. [in French].
- Margolis GS, Bender TR, Gardison GG. Growth in the Inuit over centuries. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 50.
- Bannikova RV, Udalova LS. Physical development of northern indigenous minority children in Nenets Federal Okrug. Acclimitazation and endemic pathology in the North. 1970; Arkhangelsk 54–5.
- Chiryatyeva TV. Collection of norms for physical development of pre-school aged children in Tyumenskaya Oblast. 1990; Tyumen 92.
- Platonova NA, Stepanova AD. Morphofunctional characteristics of children in the Sakha Republic (Yakutia). Yakutsky Med Zhurnal. 2007; 3: 15–17. [in Russian].
- Savvina NV, Khandy MV. Standards for individual evaluation of physical development of schoolchildren in the Sakha Republic (Yakutia): a methodological text. 2001; Yakutsk
- Sergina EP, Petrova PG, Nikolaev VG, Basharin KG. Anthropometric features of long-term male residents of the Sakha Republic (Yakutia). Sibirsky Meditsinsky Zhurnal. 2007; 22: 83–5. [in Russian].
- Skoblina NA. Physical development and health in children of the Subarctic under current social and economic conditions. 1998; Moscow
- The state of health of teenagers: scientific and practical tasks and methods for implementation. Symposium of the Summary Collegium of the Russian Ministry of Health. 2002; Moscow 55.
- Skorodok LM, Savchenko ON. Sexual development disturbances in boys. 1984; Moscow: Medicine Publishing. 238.
- Starkova NT. Clinical endocrinology. 1991; Moscow: Meditsina. 512 .
- Khandy MV, Zakharova AM, Gavrilova RS. Physical development of newborns in the Far North. Current issues in clinical medicine in the Far North. 1981; Yakutsk 30–1.
- Savchenkov VY, Venger TF. The healthy child: a handbook for students and pediatricians. 1998; Krasnoyarsk 109.
- Burtseva TE, Egorova AG, Uvarova TE, Nikolaeva LA. Effects of the environment on children in industrial areas of Northern Yakutia. Ecology and human health in the North. 2007; Yakutsk 126–8.
- Dutova SV, Khramova EE, Dolgikh VV. Physical development of children in Tofalariya. Children's health in the North. 2008; Yakutsk 78–9.
- Trolukova AN. Physical and sexual development of Yakut girls. 2006; Moscow
- Burtseva TE. Methodologic and medical principles of using information networks for providing medical care to the child population of the Far North. 2005; St. Petersburg
- Burtseva TE, Egorova AG. Physical development of schoolage children in the village of Urun-Khaya, Anabarsky Region, Yakutia. Children's health in the North. 2008; Yakutsk 67–8.
- Kozlov AI, Vershubskaya GG. Medical anthropology of the indigenous population of northern Russia. 1999; Moscow: International Independent University of Environmental and Political Sciences Press. 288.
- Krivoshapkin VG, Alekseev VP, Petrova PG. Regional standards for human health in the North (in tables and figures). 2001; Yakutsk: Izd-vo Departmenta NiSPO. 146.
- Zakharov SI, Trofimova MS. The health of newborn Evenks in the Aldansky region. Indigenous minorities in Northern Yakutia: status and problems, a collection of scientific works. 1983; Yakutsk 94–5.
- Markova SV, Khandy MV, Petrova PG. Impact of environmental factors on children's health in the diamond mining region. Issues related to human health and pathology in the North: facts, problems and prospects. 2002; Yakutsk 46–8.
- Prakhin EI, Gritsinskaya VL. Association of physical, biological, psycholgocial development indicators in the overall health of children from northern Siberia. Pediatriya. 1997; 6: 67–9. [in Russian].
- Solovyeva MI, Uchakina RV, Kozlov VK. Physical and sexual development of schoolgirls in Yakutia. Far East Med J. 1998; 2: 49–53.
- Savvina NV, Khandy MV. Growth and development of modern schoolchildren in the Sakha Republic (Yakutia). Prevention of non-communicable disease as a part of a plan to preserve health. 2000; Yakutsk 74–5.
- Vinokurov YM. A comparative analysis of the physical development of schoolchildren in Yakutia. Medical and geographic problems in Yakutia. 1977; Yakutsk 104–5.
- Avtsyn AP. Adaptation and disadaptation from a pathologist's viewpoint. Klin Med. 1974; 5: 3–15. [in Russian].
- Deryapa NR, Ryabinin IF. Human adaptation to polar regions. 1977; Moscow: Meditsina. 294.
- Panin LE. The energetics of adaptation. 1978; Moscow: Meditsina. 191.
- Afanasyeva VD. An examination of the clinical duration of atherosclerosis and hypertensive diseases in the Far North. 1972; Moscow: Medicine Publishing. 99.
- Marachev AG, Sorokovoy VI, Kornev AV, Bobkov GA. [The bioenergetics of erythrocytes in residents of the North]. Fiziologiya cheloveka. 1982; 8: 407–15. [in Russian].
- Kaznacheev VP, Kulikov VY, Kolosova NG, Buraeva LB. Biophysical adaptation mechanisms to the Far North. Vestn Akad Med Nauk + . 1979; 6: 3–11. [in Russian].
- Nikitin YP, Shakalis DA, Khasnulin VI. Peroxidation of lipids and anti-oxidative activity of lipids in the settler and indigenous populations of Chukotka and ischemic heart disease. Physiological and clinical aspects of adaptations to the circulatory and respiratory systems in the Far North: a collection of articles. 1981; Novosibirsk: Nauka. 16–19.
- Bobrov NI, Lomov OP, Tikhomirov VP. Physical and health-related aspects of human acclimatization to the North. 1979; Moscow: Meditsina. 199.
- Kandror IS. Essay on the physiology and health of residents of the Far North. 1968; Moscow: Meditsina. 280.
- Panin LE. [Diet of settler, aboriginal and indigenous populations of the Asian North]. Byul CO AMN SSSR. 1981; 2: 76–89. [in Russian].
- Rodahl K, Issekutz B. Vaughn L. Nutritional effects on human performance in the cold. Nutritional requirements for survival in the cold and at altitude. 1965; Ft. Wainwright, AK: Arctic Aeromedical Lab. 7–47.
- Veselukhin RV. Basal metabolism and blood chemistry of the indigenous peoples of polar subregions and Chukotka. Physiology and pathology of human adaptive mechanisms. 1977; Novosibirsk: Sibirsky filial AMN SSSR. 5–20.
- Borisova NV, Petrova PG, Markova SV. Ecological and physiological basis of the formation of functional reserves in the population of the Sakha Republic (Yakutia). Sibirsky Meditsinsky Zhurnal. 2007; 22: 58–1. [in Russian].
- Nazarko VA, Smirnov YI, Kushnir AV, Sokolyansky AV. Certain physical and physiologic indicators in northern youth. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 93–4.
- Taskaev YN, Kaganovich DI, Shishkin GS, Petrunicheva KN, Dobrinsky AA, Geyderbrekht II. Functionality of the human respiratory system in the low temperatures of Siberia and the Far North. IV International Symposium on Subpolar Medicine. 1978; Nobosibirsk 25–6.
- Schaefer O, Timmermans TV, Hildes JA. Respiratory function impairment and cardiopulmonary consequences in long time residents of the Canadian Arctic. IV International Symposium on Circumpolar Health. 1978; Novosibirsk 31.
- Marachev AG, Matveev LN. Morphofunctional manifestations of respiratory tract adaptations in residents of the North. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 98–9.
- Marachev AG. Morphofunctional principles of adaptation and pathology of the lungs, heart and blood in human beings in the Far North. 1980; Moscow
- Milovanov AP. Regional adaptations of pulmonary microvasculature in the Northeast. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 101–2.
- Velichkovsky BT. [On the pathogenic areas being examined in the study of the impact of the environment on human health]. Vestn Ross Akad Med Nauk. 2003; 3: 3–8. [in Russian].
- Avtsyn AP, Marachev AG. [Adaptation and disadaptation manifestations in residents of the Far North]. Fiziologiya Cheloveka. 1975; 1: 587–600. [in Russian].
- Bligh J, Chauca D. Effects of hypoxia, cold exposure and fever on pulmonary artery pressure, and their significance for Arctic residents. Circumpolar Health: Fifth International Symposium. 1981; Copenhagen 606–7.
- Sovershaeva SL. Northern pulmonary hypertension in residents of Arkhangelsk Oblast. Pulmonary hypertension. 1982; Moscow: Frunze. 47–9.
- Hildes JA, Schaefer O. Health of Iglooliik Eskimos and changes with urbanization. J Hum Evol. 1973; 2: 241–6.
- Rennie DW, Prampero P, Fitts RW, Sinclair L, Wilson D, Hogan P. Cardiopulmonary fitness of Alaska Eskimos. II International Symposium on Circumpolar Health. 1971; Oulu
- Danishevsky GM. Human pathology and disease prevention in the North. 1968; Moscow: Meditsina. 412.
- Gyrgolkau LA, Nikitin YP, Scherbakova LV. Levels of arterial pressure and incidence of arterial hypertnesion in the indigenous residents of Chukotka. Cardiovascular pathology in the Arctic: fundamental and applied aspects. 2008; Yakutsk 13–15.
- Turchinsky VI. Ischemic heart disease in the Far North. 1980; Novosibirsk: Nauka. 304.
- Petrov RA, Alekseev VP, Solomatin AP. Cardiovascular pathology in Yakutia. 1982; 153 [in Russian].
- Argunov VA. Precursors and early stages of atherosclerosis in the aorta and coronary arteries in children and young people of the indigenous and non-indigenous populations of Yakutia and the significance for progression of atherosclerosis. 1996; Novosibirsk: Nauka.
- Khamnagadaev II, Polikarpov LS, Gankin MI. Diet of the rural indigenous populations of the North. Terapevtichesky Arkhiv. 2003; 1: 34–7.
- Krogh A, Krogh M. A study of the diet and metabolism of Eskimos undertaken in 1908 on an expedition to Greenland. Meddelelser om Grønland. 1914; 51: 36.
- Panin LE. [Homeostasis and diet in the subpolar regions]. Byul CO AMN SSSR. 1987; 6: 60–5. [in Russian].
- Mironova GE, Krivoshapkina ZN, Olesova LD, Yakovleva AI, Nikolaev VM, Okhlopkova ED, etal. Biochemical aspects of human pathology in the North. Molecular and cellular aspects of human pathology in the North. 2007; Yakutsk 5–7.
- Boyko ER, Potolitsyna NN, Boyko SG, Larina VE, Zelenov VA. [Supplying the Northern populations with fat-soluble vitamins]. Vopr Pitaniya. 2008; 77: 64–7. [in Russian].
- Boyko ER. Physiological and biochemical principles of the vital functions of humans in the North. 2005; Ekaterinburg
- Efremov VV. [Food rationing problems in the Far North of the Soviet Union]. Problemy Severa. 1970; 14: 186–97. [in Russian].
- Sitnikova GG. [Provision of fat-soluble vitamins to the indigenous population of the Far North. Current issues in northern clinical medicine: a collection of scientific works. 1994; Yakutsk: Yakutsk State University Press. 117–1.
- Tikhonov DG. Disorders of the esophagus, stomach and duodenum in the Sakha Republic (Yakutia). 1993; Moscow
- Krivoshapkina DM, Khandy MV. Calcium and vitamin D deficiencies in children. Ecology and human health in the North. 2007; Yakutsk 155–7.
- Machlin LJ. Handbook of vitamins. 1991; New York: M. Dekker. 595. 2nd ed.
- Meagher EA, Barry OP, Lawson JA, Rokach J, FitzGerald GA. Effects of vitamin E on lipid peroxidation in healthy persons. JAMA. 2001; 285: 1178–82.
- Danishevsky GM. Human acclimatization to the North (with an essay on endemic pathology and health). 1955; Moscow
- Zakharova FA. Immunologic reactivity in the indigenous peoples of Yakutia. Issues related to human health and pathology in the North: facts, problems and prospects. 2002; Yakutsk 30–1.
- Avtsyn AP. Introduction to geographical pathology. 1972; Medicine Publishing. 328.
- Borodin YI, Nikitin YP, Belov GF, Shutskaya EI. Indicators of morbidity and metabolism in residents of the North and Novosibirsk. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 264–5.
- Kartseva TM, Graschenkova OV. Chronic non-specific disorders of the lungs and upper respiratory tract. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 105–6.
- Krivoshapkin VG. Climate and geographical features of the prevalence of gastric cancer in the population of the northern Asian USSR. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 270–1.
- Sedov KR. Preserving and improving the situation of the northern indigenous minorities. Vestn Ross Akad Med Nauk. 1993; 8: 5–9. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract] [in Russian].
- Dyerberg J, Bang HO. The role of Eskimo food in the prevention of coronary heart disease. IV International Symposium on Circumpolar Health. 1978; Novosibirsk 61–2.
- Feldman SA, Ho KJ, Lewis LA, Mikkelson B, Taylor CB. Lipid and cholesterol metabolism in Alaskan Arctic Eskimos. Arch Pathol. 1972; 94: 42–58. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract].
- Mann G, Scott E, Hursh L, Heller C, Youmans J, Consolazio F, etal. The health and nutritional status of Alaskan Eskimos. A survey of the interdepartmental committee on Nutrition for National Defense. Am J Clin Nutr. 1962; 11: 31–76.
- Maynard JE. A study of cardiovascular disease risk factors among Alaskan Eskimo men. II International Symposium on Circumpolar Health. 1971; Oulu 30.
- Menshikov YF. Experience studying morbidity in Kolsky peninsula. Zdravookhranenie Rossiyskoy Federatsii. 1965; 5: 21–3. in Russian.
- Prikatova MK. The state of the cardiovascular system in the indigenous populations of the Far North. Work and human health in the Far North. 1965; Norilsk
- Scott EM, Griffith IV, Hoskins DD, Whaley RD. Serum-cholesterol levels and blood-pressure of Alaskan Eskimo men. Lancet. 1958; 2: 667–8.
- Thomas WA. Health of carnivorous race, study of Eskimos. JAMA. 1927; 88: 1559.
- Rodahl K. Observations on blood pressure in Eskimos. Norsk Polarinstitutt Skrifter. 1954; 102: 53.
- Rodahl K. Preliminary survey of dietary intakes and blood levels of cholesterol and the occurrence of cardiovascular diseases in the Eskimo. Norsk Polarinstitutt Skrifter. 1954; 102: 31.
- Polikarpov LS. Environmental aspects of cardiology in the Far North. X All-Union Symposium Biological Problems of the North. 1983; Magadan 98.
- Schaefer O. Medical observations and problems in the Canadian arctic: part I. Can Med Assoc J. 1959; 81: 248–53. [PubMed Abstract] [PubMed CentralFull Text] [PubMed Abstract] [PubMed CentralFull Text] [PubMed Abstract] [PubMed CentralFull Text].
- Wilber CG, Levine VE. Fat metabolism in Alaskan eskimos. Exp Med Surg. 1950; 8: 422–5. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract].
- Alekseev VP. Prevalence of atherosclerosis in the city of Yakutsk. 1968
- Argunov VA. Pathological anatomy and morphogenesis of atherosclerosis of the aorta and coronary arteries in residents of Yakutia. 2006; Novosibirsk: Nauka. 184.
- Ischenko MV. Information on endemic pathologies of Yakutia. Endemic pathologies. 1964; Moscow 73–5.
- Prikatova MK. Acclimatization of aboriginals of the Far North to the city of Krasnoyarsk. Human adaptation to Northern conditions. 1976; Krasnoyarsk 53–4.
- Sundberg S, Buchberger J, Siltanen P, Andersen KL. Resting arterial blood pressure in adult Lapps. II International Symposium on Circumpolar Health. 1971; Oulu 54.
- Bang HO, Dyerberg J. Plasma lipids and lipoproteins in Greenlandic west coast Eskimos. Acta Med Scand. 1972; 192: 85–94.
- Malchevsky YM, Malchevskaya MD. Social and economic development of the indigenous northern peoples. 1990; Novosibirsk: Nauka.
- Petrov RA, Ryvkin IA. Ischemic heart disease and arterial hypertension in Yakutsk. Kardiologiia. 1977; 3: 63–70. in Russian.
- Schaefer O, Timermans TV, Eaton RDP, Matthew A. Comparison of general and nutritional health in two Eskimo populations at different stages of acculturation. IV International Symposium on Circumpolar Health. 1978; Novosibirsk 5–6.
- Ivanov KI. The clinical epidemiological situation of cardiovascular disorders in the Sakha Republic (Yakutia). Yakutsky Med Zhurnal. 2007; 4: 4–10. in Russian.
- Sofronova SI, Voevoda MI. The association between overweight and arterial hypertension in indigenous minority populations of Yakutia. Cardiovascular pathology in the Arctic region: fundamentals and applied aspects. 2008; Yakutsk 31–2.
- Panin LE. Biochemical mechanisms of stress. 1983; Novosibirsk: Nauka. 233.
- Fleshman JK, Wilson JF, Cohen JJ. Bronchiectasis in Alaska Native children. Arch Environ Health. 1968; 17: 517–23.
- HIldes JA, Schaefer O. Chronic lung disease and cardiovascular consequences in Iglooliigmiut. III International Symposium on Circumpolar Health. 1976; Toronto 327–31.
- Schaefer O. Right bundle branch block and pseudo-infarction EGG patterns in Eskimo men. II International Symposium on Circumpolar Health. 1971; Oulu 31.
- Argunova AN, Makarov VM, Vinokurov SN. Risk factors impacting the development and duration of subclinical pneumonia in Yakutia. Ecology and human health in the North. 2007; Yakutsk 64–6.
- Avtsyn AP, Barsova RI, Botvinnik LK, Zhavoronkov AA, Kenig EE, Marachev AG, etal. Chronic progressive respiratory disorders as an endemic pathology in some northeastern regions of the USSR. Vestn Akad Med Nauk + . 1971; 10: 3–13. in Russian.
- Lutsenko MT, Tseluyko SS, Krasavina NP. Morphological changes to the respiratory organs as a result of low temperatures. IV International Symposium on Subpolar Health. 1978; Novosibirsk 99–100.
- Makarov VM. The epidemiology of chronic obstructive pulmonary disease and secondary medical prophylaxis. 1994; Yakutsk
- Yagya NS. [Morbidity from chronic respiratory disorders in the North]. Zdravookhr RSFSR. 1974; 6: 25–8. in Russian.
- Timofeev LF, Krivoshapkin VG, Platonov FA, Egorova AG, Tyrylgin MA, Prokopyeva MV. Regionalization of the northern Russian Federation: medical and biological criteria for lifestyle discomfort in the population. Yakutsk Med J. 2005; 1: 10–15.
- Yagya NS. Morbidity in the Far North. Zdravookhr RSFSR. 1976; 2: 25–9.
- Androsov VT. On the prevalence of clinical-pathogenetic variants of chronic gastritis among the population of Yakutia. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 271.
- Krivoshapkin VG, Arzhakova GS. State of the mucosa of the lower esophagus in northern indigenous peoples of Yakutia. Bioclimatic and medico-geographical issues: a collection of scientific works. 1977; Novosibirsk: Nauka. 84–6.
- Bessonov PP, Bessonova NG, Kurilovich SA, Reshetnikov OV. Prevalence of dyspeptic disorder in the rural indigenous peoples of Yakutia. Molecular and cellular aspects of human pathology in the North. 2007; Yakutsk 90–1.
- Deryapa NR, Solomatin AP. Current issues in medico-geographical pathologies in Yakutia. Bioclimatic and medico-geographical issues: a collection of scientific works. 1977; Novosibirsk: Nauka. 52–4.
- Petrov PA, Ygya NS. Morbidity in the indigenous and settler population of the Far North (with the city of Yakutsk as an example). IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 25–6.
- Timofeev GA. Medical and environmental research in the Sakha Republic (Yakutia). Achievements and prospects for medical science in the Sakha Republic (Yakutia). 2002; Yakutsk 23–30.
- Krivoshapkin VG. Premalignancies in the stomach in the Far North of the USSR. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 120–1.
- Loskutova KS, Trufanov AS, Argunov VA, Inokentyeva AS, Gorokhova NN, Kolesnikova TN, etal. Morphological characteristics of chronic gastritis and features of gastric cancer in Yakutia. Molecular and cellular aspects of human pathology in the North. 2007; Yakutsk 78–9.
- Starostin VG. Ulcerative disorders in the Sakha Republic (Yakutia). Republican Scientific-Practical Conference of the Medical Institute of Yakutsk State University. 1996; Yakutsk 45.
- Yaroslavsky VE, Bychkov VG. A comparative analysis of the indigenous and settler populations of Kanty-Mansiysky National Okrug. IV International Symposium on Circumpolar Health. 1978; Novosibirsk 282–3.
- Alperovich BI. Alveolar echinococcosis. 1967; Yakutsk 223.
- Chernyavsky VF, Nikiforov OI, Repin VE, Kershengolts BM, Sofronova ON. Epizoological-epidemiological potential of zoonotic infections in Yakutia and its dynamics under modern conditions. Yakutsky Med Zhurnal. 2009; 1: 58–61. in Russian.
- The impact of global climate change on the health of the population of the Russian Arctic: a report by international experts from the UN. 2007; UNESCO and UNDP.
- Anisimov IV. The epidemiology of tuberculosis among the northern populations: materials from the scientific and practical conference of the Medical institute of Yakutsk State University. Scientific and Practical Conference of the Medical Institute of Yakutsk State University. 1996; Yakutsk
- [Chronic hepatitis B: practical recommendations from the American Association for the Study of Liver Diseases]. Ros Zhurn Gastroenterol Gepatol Kolproktol. 2008; 4–25. in Russian.
- Semenov SI, Savvin RG, Chakhova ND, Pavlov NN, Indeeva LD, Chemezova RI, etal. Studies on markers of viral Hepatitis B, C and D in the Sakha Republic (Yakutia). Issues related to human health and pathology in the North: facts, problems and propects. 2002; Yakutsk 235–7.
- Sleptsov AP. Viral hepatitis in Yakutia. Siberian Med J. 2007; 22: 52–4.
- Zotova AV, Alekseeva MN, Mikhaylov MI. Prevalence of viral Hepatitis B among reindeer herders in southern Yakutia. Ecology and human health in the North. 2007; Yakutsk 202–3.
- Alekseeva MN. Viral hepatitis in the Sakha Republic (Yakutia). 2002; St. Petersburg
- Bugaeva TT, Alekseeva MN, Ivanov IM, Sleptsova SS, Karataev PD. [Chronic viral hepatitis as a primary risk factor for hepatocellular carcinoma in Yakutia]. Sibirsky Meditsinsky Zhurnal. 2007; 22: 47–9. in Russian.
- Ivanov PM. Esophageal and gastric cancer as an endemic pathology in the North. 1999; Yakutsk: Bichik. 192.
- Thomas GV, Williams JH. Cancer morbidity among indigenous residents of Laborador: a 25-year study. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 269.
- Grin A, Kroman N. Chronic disease and mortality in the Arctic Inuit population over 25 years. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 26–7.
- Hart Hansen JP, Nygaard N. Malignant neoplasms in the Inuit of Greenland. IVth International Symposium on Circumpolar Health. 1978; Novosibirsk 31.
- Krivoshapkin VG. Chronic gastritis as a precancerous disorder in the North. 1974; Yakutsk
- Makeeva RP, Samsonov VA, Silvestrov VS. State of the glands of the body of the stomach in esophageal cancer patients in Karelia SSR (based on biopsied tissue). IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 129–30.
- Dolgintsev VI, Veber OA, Filatov PI, Fazlutidinov RI. A comprehensive study of the epidemiology of malignant neoplasms in Western Siberia. IV International Symposium on Subpolar Medicine. 1978; Novosibirsk 285–6.
- Makarova NN, Ivanov PM. Cervical cancer as a pressing issue in the North. Issues related to human health and pathology in the North: facts, problems and prospects. 2002; Yakutsk 244–6.
- Ivanov IA. [What do we know about suicides? Death in pairs]. Yakutsky Med Zhurnal. 2007; 3: 54–7. in Russian.
- Pakhomov YE, Turnin KK. Alcohol consumption of indigenous minorities in Northern Yakutia. Indigenous minorities in Northern Yakutia: status and problems, a collection of scientific works. 1983; Yakutsk 92–3.
- Kershengolts BM. Alcoholization and narcotization – important threats to the genetic pool of the Northern populations, and prevention methods. Protecting the genetic pool of the Northern peoples. 1995; Yakutsk 60–9.
- Kershengolts BM, Turnin KK. Alcohol metabolism in Northern indigenous minority populations. Indigenous minorities in Northern Yakutia: status and problems, a collection of scientific works. 1983; Yakutsk 93–4.
- Turnin KK. Ethnic-related features of alcoholism. Seventy years of the USSR Academy of Sciences in the Yakut Republic and indigenous minority populations. 1995; Yakutsk
- Agarwal DP, Goedde HW. Palmer TN. The role of alcohol metabolizing enzymes in alcohol sensitivity, alcohol drinking habits, and incidence of alcoholism in oriental. The molecular pathology of alcoholism. 1991; Oxford: Oxford University Press. 211–39.
- Bennion LJ, Li TK. Alcohol metabolism in American Indians and whites. Lack of racial differences in metabolic rate and liver alcohol dehydrogenase. N Engl J Med. 1976; 294: 9–13.
- Cook C, Gurling HMD. Palmer TN. Genetic factors in alcoholism. The molecular pathology of alcoholism. 1991; Oxford: Oxford University Press. 182–210.
- Mazurin AV, Vorontsov IM. An introduction to children's illnesses. 2000; Sotis: St. Petersburg
- Henkin RI, Gill JR, Bartter FC. Studies on taste thresholds in normal man and in patients with adrenal cortical insufficiency: the role of adrenal cortical steroids and of serum sodium concentration. J Clin Invest. 1963; 42: 727–35.
- Shabalov NP. Diagnosis and treatment of endocrine disorders in children and teenagers. 2003; Moscow: MEDpress-inform. 544.
- Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child. 1976; 51: 170–9.
- Wilson RC, Mercado AB, Cheng KC, New MI. Steroid 21-hydroxylase deficiency: genotype may not predict phenotype. J Clin Endocrinol Metab. 1995; 80: 2322–9. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract].
- Klimov AN. Kositsky . Atherosclerosis. Preventive cardiology: a handbook. 1987; Moscow: Meditsina. 239–316.
- Savvina NV. Preserving and strengthening the health of school children. 2006; Moscow
- Medik VA, Yuryev VK. Part II: healthcare provision. 2003; Moscow: Meditsina. 456.
- Dedov II, Semicheva TV, Peterkova VA. Sexual development in children: norms and pathologies. 2002; Moscow 231.
- Pang SY, Wallace MA, Hofman L, Thuline HC, Dorche C, Lyon IC, etal. Worldwide experience in newborn screening for classical congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Pediatrics. 1988; 81: 866–74. [PubMed Abstract] [PubMed Abstract] [PubMed Abstract].
- Fedorova SA. A genetic portrait of the peoples of the Sakha Republic (Yakutia): an analysis of mitochondrial DNA and Y-chromosome lines. 2008; Yakutsk: Publishing House of the Yakutsk Research Center, Siberian Division of the Russian Academy of Sciences. 235.
