
Abstract
Objectives
To determine and compare the incidence of cancer among the 8 Arctic States and their northern regions, with special focus on 3 cross-national indigenous groups – Inuit, Athabaskan Indians and Sami.
Methods
Data were extracted from national and regional statistical agencies and cancer registries, with direct age-standardization of rates to the world standard population. For comparison, the “world average” rates as reported in the GLOBOCAN database were used.
Findings
Age-standardized incidence rates by cancer sites were computed for the 8 Arctic States and 20 of their northern regions, averaged over the decade 2000–2009. Cancer of the lung and colon/rectum in both sexes are the commonest in most populations. We combined the Inuit from Alaska, Northwest Territories, Nunavut and Greenland into a “Circumpolar Inuit” group and tracked cancer trends over four 5-year periods from 1989 to 2008. There has been marked increase in lung, colorectal and female breast cancers, while cervical cancer has declined. Compared to the GLOBOCAN world average, Inuit are at extreme high risk for lung and colorectal cancer, and also certain rare cancers such as nasopharyngeal cancer. Athabaskans (from Alaska and Northwest Territories) share some similarities with the Inuit but they are at higher risk for prostate and breast cancer relative to the world average. Among the Sami, published data from 3 cohorts in Norway, Sweden and Finland show generally lower risk of cancer than non-Sami.
Conclusions
Cancer among certain indigenous people in the Arctic is an increasing public health concern, especially lung and colorectal cancer.
The 8 member states of the Arctic Council (Canada, Denmark, Finland, Iceland, Norway, Sweden, Russian Federation and the United States, hereafter referred to as the Arctic States) comprise some of the world's economically most developed countries. Yet, within these countries, substantial health disparities persist, between northern and southern regions, and within the North, between indigenous and non-indigenous peoples, although the extent of the disparities varies across countries (Citation1–Citation3).
We report on an epidemiological review of cancer in the Arctic States and their northern regions. Cancers such as lung and breast can be viewed as an indicator of the rapid social, economic and environmental changes that Arctic populations, especially indigenous peoples, are experiencing. A circumpolar comparative framework is particularly useful as countries and regions that share many commonalities can learn best practices from one another in cancer prevention and control.
Previous reviews have focused on specific regions such as Greenland (Citation4), Alaska (Citation5), northern Canada (Citation6), and specific populations such as the Inuit (Citation7, Citation8). The current review compares all northern regions within the Arctic (for which data are available), with special focus on 3 indigenous populations whose traditional homelands span across present day national boundaries – Inuit, Athabaskans and Sami. We also offer a global perspective by putting the circumpolar populations in the context of major geopolitical regions of the world.
Methods and data sources
We obtained data on cancer incidence among the Arctic States and their northern regions from national statistical agencies, cancer registries and regional health authorities. Such data refer to the total populations with all ethnicities combined. These agencies are listed in the notes of Table . There are also international cancer databases such as NORDCAN for the Nordic countries (Citation9) and GLOBOCAN for the member states of the World Health Organization (Citation10). With the exception of Russia, the Arctic States have national cancer registries that are considered to be of sufficient quality to be included in the International Agency for Research on Cancer's statistical compendium Cancer Incidence in Five Continents, CI5 (Citation11). The St. Petersburg registry is the only Russian entry in CI5. National and regional cancer incidence data from Russia are available from the annual reports of the P.A. Hertzen Research Institute of Oncology in Moscow (Citation12). In recent years, Norwegian international assistance efforts have been directed at improving the quality of the cancer registry of an Arctic region in north-western Russia (Citation13). In this study we did not access data from this registry.
Table I. Mean age-standardized incidence rates of selected cancer sites in 8 Arctic States and their northern regions, 2000–2009
The regional and national rates were directly age-standardized to the “world standard population” of the International Agency of Research on Cancer (Citation11). This statistical procedure ensures that the widely different age structures across populations have been adjusted for and can be compared meaningfully.
For data on the 3 indigenous groups, we utilized specialized databases. Data for Alaska Natives are obtained from the Alaska Native Tumor Registry (ANTR), a state-wide population-based registry which has been in existence since 1969. It is currently maintained by the Alaska Native Tribal Health Consortium in Anchorage, Alaska. ANTR covers Alaska Native and American Indian patients living in Alaska at the time of diagnosis who meet eligibility criteria for health care benefits from the United States Indian Health Service and its contracted providers. Alaska Native people are comprised of 3 major groups – Eskimos (here termed Inuit), Indian and Aleut. Procedures for data collection and coding follow standards of the Surveillance, Epidemiology and End Results (SEER) Program of the National Cancer Institute (Citation14). Further separation of Alaska Native data into Inuit (Eskimo) and Indians was performed by JK and colleagues in ANTR.
Statistics Canada operates the Canadian Cancer Registry, which receives cancer data from all provincial and territorial cancer registries and performs internal record linkage and national death clearance annually. Data on cancer cases diagnosed among permanent residents of the 3 northern Canadian territories (who generally obtain cancer care services outside the territories) are maintained by the respective health departments of Yukon, Northwest Territories (NWT) and Nunavut. Although ethnic identifiers are not included in the national registry, differentiation of Inuit, First Nations and Métis people is possible in the territorial cancer registries of NWT (Citation15) and Nunavut (Citation16), but is incomplete in Yukon. Although regional data for Yukon are included, First Nations-specific data from Yukon were not included in this study. Inuit-specific data are also not available for the predominantly Inuit-inhabited region of Nunavik in the province of Québec.
The Danish Cancer Registry registers cases from both Denmark and Greenland. Through data linkage with the Greenland population registry, cases occurring among individuals born in Greenland and residents in Greenland at the time of diagnosis can be identified. The use of “born in Greenland” as a proxy identifier for Greenland Inuit is a long-established practice. This is not a satisfactory approach as clearly there are Danish babies being born in Greenland and Inuit babies being born in Denmark. With increased population movements, the accuracy of the “born in Greenland” as an identifier for Greenland Inuit will be reduced over time. Previously a database of cases from 1989 to 2003 was created by JF and colleagues at the Danish Epidemiology Research Centre, Statens Serum Institut in Copenhagen (Citation7). This database was updated for the present study.
None of the national population registries or statistical databases of the Nordic countries record ethnicity. Only a handful of studies have been published where Sami identity among study participants was specifically determined based on a variety of linguistic, genealogical and sociopolitical criteria. Regional Sami cohorts have been assembled in Norway (Citation17) covering the period 1970–1997, Sweden (Citation18) covering the period 1961–2003, and Finland (Citation19) covering the period 1979–1998, which was updated to 2005 in a previous review (Citation20). The Finnish Sami cohort was further updated to 2010 by LS and colleagues at the University of Helsinki and Finnish Cancer Registry.
Ethnic identity of patients is not recorded in health care statistics in post-Soviet Russia (Citation21). Only one study on cancer among several Russian indigenous peoples in the Arctic has been published in English, covering the period 1977–1988 (Citation22).
Cancer cases were classified by site in accordance with the International Classification of Diseases, 10th edition (ICD-10). Only those coded as malignant neoplasms (ICD-10 codes C00 to C96 and their equivalents in earlier editions) were included in this review, excluding benign and in situ neoplasms. Non-melanoma skin cancer (ICD-10 C44) was excluded, because of the inconsistency across registries in including/excluding it. By excluding it, the total number of cancer cases from all sites is more comparable, without being influenced by this common, rarely fatal and often under-reported cancer.
We did not conduct independent validation of diagnosis or classification, but accept them as reported by the official agencies. In terms of quality of incidence data, GLOBOCAN assigns grade D to Russia and grade A to all the other Arctic States (Citation10).
Results
Regional variation in cancer incidence
We were able to collect cancer incidence data from all 8 Arctic States and 20 of their northernmost regions for the decade 2000–2009 (Table ). The various data sources for the countries and regions are provided in the notes to the table. Among northern regions, the highest age-standardized incidence rates are observed in Nunavut, Greenland and Alaska. Note these data refer to national and regional statistics which are not specific to indigenous people. Moreover, Nunavut and Greenland have the highest proportion of indigenous people (Inuit) in their population, accounting for more than 85%. Other regions with high proportion of indigenous people are the NWT (50%), Yukon (25%) and Alaska (20%) (Citation2). The proportion is lower in the northern regions of Eurasia. In general, the disparities in cancer incidence between the northern regions and their national counterparts are least among the Nordic countries, but considerable between Greenland and Denmark, and between Nunavut and Canada.
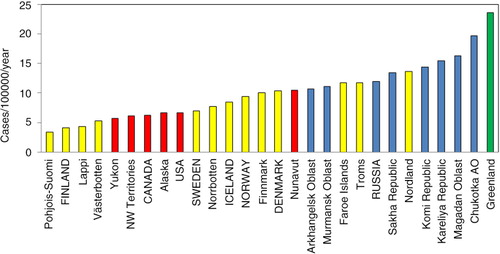
Among the different cancer sites, cancer of the lung and colon/rectum in both sexes and breast in women are the commonest in most populations. For lung cancer, Nunavut and Greenland lead all regions and countries in both men and women. Russia and its regions have high rates among men, but the opposite is true for women (). Greenland reports the highest incidence of cervical cancer, followed by several Russian regions (). Higher rates for breast cancer are found in North America and the Nordic countries, while Greenland, Nunavut and Russian regions are at the low end of the range.
Fig. 1. Age-standardized incidence rates of lung cancer among men and women in the Arctic States and their northern regions, 2000–2009. Note: AO=autonomous okrug.
All 8 Arctic States (in capital letters) and most of their northern regions are included in the chart – blue refer to Russia and its northern regions, yellow to the Nordic countries and their northern regions, red to Canada and USA and their northern regions, and green to Greenland.
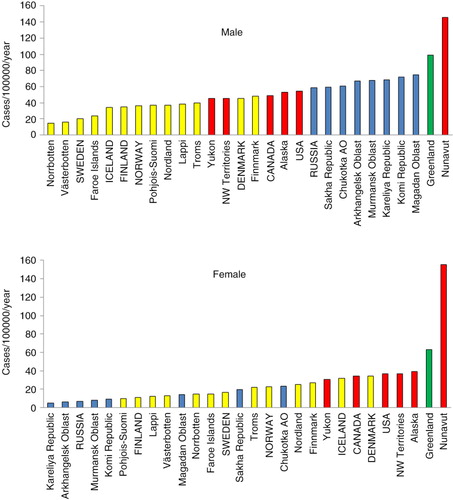
Fig. 2. Age-standardized incidence rates of cervical cancer among women in the Arctic States and their northern regions, 2000–2009.
Note: AO = autonomous okrug.
All 8 Arctic States and most of their northern regions are included in the chart – blue refer to Russia and its northern regions, yellow to the Nordic countries and their northern regions, red to Canada and USA and their northern regions, and green to Greenland.
Inuit in Alaska, Canada and Greenland
Globally there are approximately 165,000 Inuit, distributed in the United States (primarily Alaska), Canada (mainly the northern territories of Nunavut and NWT) and Denmark/Greenland. There are also fewer than 2,000 Inuit in Russia, primarily in its easternmost region of Chukotka (Citation2).
We combined the Inuit cases and populations in Alaska, NWT, Nunavut and Greenland to create a “Circumpolar Inuit” group. We obtained data from the ANTR, the territorial cancer registries of NWT and Nunavut, and the Danish Cancer Registry. Incidence data are grouped into 4 5-year periods from 1989 to 2008 (Table ). Although substantial number of Inuit also live in other American states (the “lower 48”), southern Canadian provinces and metropolitan Denmark, information on cancer occurrence in these groups is not available.
Table II. Age-standardized incidence rates among Circumpolar Inuit by cancer site, sex and time period
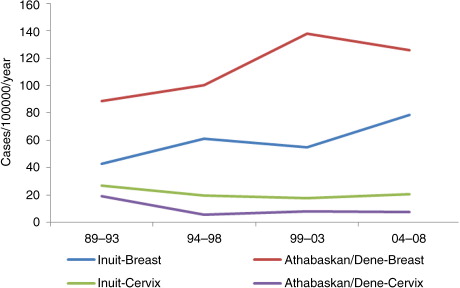
There has been an overall increase of cancer (all sites combined) over the 4 5-year periods from 1989 to 2008. The increase is particularly marked for lung (), colorectal () and female breast cancers (Table ). The overall risk of cancer among Inuit men and women has now “caught up” with those of non-Inuit in the United States, Canada and Denmark.
Fig. 3. Time trend in lung cancer incidence among circumpolar Inuit and Athabaskan/Dene, 1989–2008.
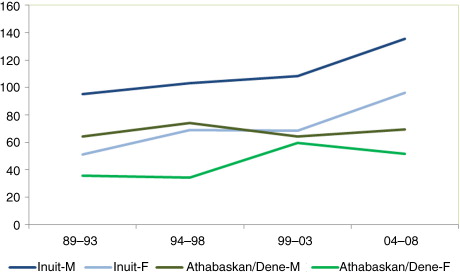
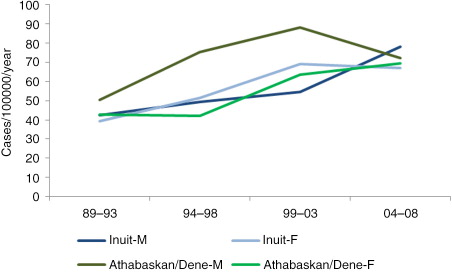
Fig. 4. Time trend in colorectal cancer incidence among circumpolar Inuit and Athabaskan/Dene, 1989–2008.
For Inuit women, breast cancer is on the rise, whereas a decline can be observed for cervical cancer ().
Fig. 5. Time trend in breast and cervical cancer incidence among circumpolar Inuit and Athabaskan/Dene women, 1989–2008.
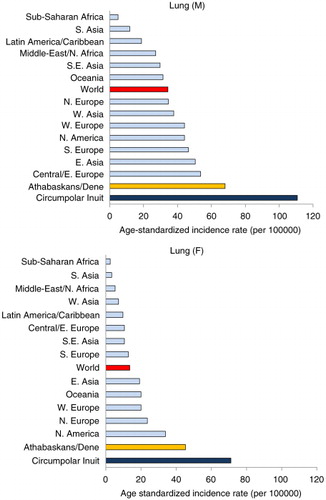
To compare the risk of different cancer sites with non-Inuit, we chose the world average age-standardized rate reported by GLOBOCAN (Citation10). Inuit are at low risk for prostate cancer, a common cancer among men. Inuit continue to be at extreme high risk for certain rare cancers such as nasopharyngeal cancer (NPC) among both men and women (). From a global perspective, Inuit today also have the world's highest incidence rate of lung cancer ().
Fig. 6. Risk of cancer by site among circumpolar Inuit relative to the GLOBOCAN world average.
Note: Bars above the 1.0 line indicates excess risk among Inuit, whereas bars below the 1.0 line indicates reduced risk. Horizontal axis is in logarithmic scale.
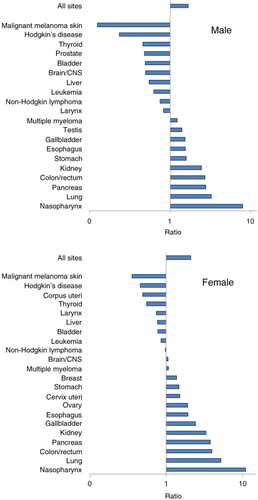
Fig. 7. Lung cancer incidence: Circumpolar Inuit and Athabaskans/Dene compared to global regions.
Athabaskans in Alaska and NWT
The Athabaskans (also spelled Athapaskans or Athabascans) are North American Indians who inhabit large swathes of the northern boreal forests of the continent. In certain regions the people self-identify as Dene. We created a group called “Athabaskan/Dene” to include members of this group who inhabit parts of Alaska and the NWT of Canada for the 4 5-year periods between 1989 and 2008 (Table ), as reported by the ANTR and the NWT Cancer Registry. While Athabaskan communities are also present in Yukon and several Canadian provinces, health data are not available by ethnicity in these jurisdictions.
Table III. Age-standardized incidence rates among Athabaskans/Dene by cancer site, sex and time period
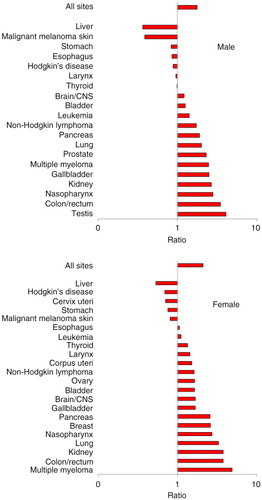
The cancer pattern among the Athabaskans sharessome similarities with the Inuit but also differs in significant respects (). While lung cancer incidence is still high in global terms, the Athabaskan/Dene incidence is substantially lower than that of the Inuit (). The incidence of colorectal cancer is higher than that of the Inuit (), although there is a decreasing trend in the most recent 5-year period among men. Unlike the Inuit (), the Athabaskan/Dene are at higher risk for prostate cancer relative to the world average (). Among women, the breast cancer incidence is substantially higher than that of Inuit (), and 3 times higher than the world average (). There is a downward trend in the cervical cancer rate ().
Fig. 8. Risk of cancer by site among Athabaskans/Dene relative to the GLOBOCAN world average. Note: Bars above the 1.0 line indicates excess risk among Athabaskans/Dene, whereas bars below the 1.0 line indicates reduced risk. Horizontal axis is in logarithmic scale.
Sami in the Nordic Countries
The traditional homeland of the Sami – Sápmi – covers the northern parts of Norway, Sweden, Finland and the Kola Peninsula of Russia. There is no accurate estimate of the total Sami population, which ranges from 60,000 to 110,000 (Citation2). As the Sami data are based on 3 different research cohorts from 3 countries, we present the data separately by cohort in Table . Also, we can only compute relative risks comparing Sami with non-Sami in the same cohort, and not population-based rates. Hence there are no Sami rates for comparison with the Inuit, Athabaskan/Dene and GLOBOCAN regions.
Table IV. Risk of cancer by site among Sami in Norway, Sweden and Finland relative to non-Sami in the same regions
With the exception of stomach and ovarian cancer in Sweden, the risk of cancer among both male and female Sami is not different from or significantly lower than non-Sami living in the same regions.
Discussion
Cancer is becoming a significant public health problem in the Arctic, especially among some indigenous populations. From a global perspective, the circumpolar Inuit and Athabaskan/Dene have rates for several cancer sites that exceed all other regions in the world. An increasing trend is also evident, and represents a change from a few decades ago when the risk of cancer was generally below that of non-indigenous populations in the same region.
There are methodological limitations that pertain to the primary data sources which are beyond the control of the authors. Most but not all Arctic States have national and regional cancer registries that use internationally standardized methods of data collection and reporting. Unfortunately the availability of ethnic-specific (especially with regard to indigenous populations) is the exception rather than the rule, We were able to obtain data on 3 indigenous groups – the Inuit, the Athabaskan/Dene and the Sami, and even among these groups, not all geographical regions can be represented. Furthermore, the size of indigenous population is small in most Artic regions, although combining the same ethnic groups living in similar habitats across national borders overcomes small sample size to a certain extent.
Of the 3 indigenous groups studied, the Sami in the Nordic countries is the exception in that its cancer pattern differs only slightly from non-Sami in the same regions. Because northern Scandinavia was heavily exposed to nuclear fallout from Soviet nuclear tests in the Kola Peninsula during the 1950s and 1960s and the Chernobyl accident in 1986, concern was expressed regarding the risk of cancer among the Sami populations of Norway, Sweden and Finland, in view of the increased levels of caesium 137 in lichen, reindeer meat, and in whole-body content among reindeer herders. Studies to date showed no detectable excess of either leukaemia or thyroid cancer, which are radiation-sensitive. Indeed, the incidence of prostate, lung, breast, and colorectal cancer is lower than in the rest of the population (Citation17–Citation20).
The absence of significant disparity in cancer incidence between Sami and non-Sami in the Nordic countries is similar to the patterns observed for other health indicators, including mortality measures, social determinants and health behaviours (Citation23, Citation24).
Among the Inuit, the extreme high risk of several cancer sites – namely nasopharyngeal cancer (NPC) – continues to be observed. NPC has long been recognized as prevalent among the Inuit, which has been dubbed as a “traditional” cancer, unlike the “modern” ones such as lung and breast (Citation25). The risk of NPC is comparable to those observed among East Asian populations. The Athabaskan/Dene are also at high risk for NPC, although to a lesser extent than the Inuit, a pattern that differs from that observed among American Indians outside Alaska (Citation26).
While the risk of NPC among the circumpolar Inuit and Athabaskan/Dene is extremely high relative to other populations, it is still very rare. From a public health perspective the most important cancers are lung, colorectal and breast cancer.
The differential risk in lung cancer largely reflects smoking prevalence, which is extremely high among the indigenous people of Alaska, northern Canada and Greenland. For example, 39% of Alaska Natives are current smokers, compared to only 18% for the state as a whole (Citation27). In northern Canada, almost 63% of Inuit adults are daily smokers, compared to 16% among all Canadians (Citation28). Among the Dene in the NWT, 60% of adults are current smokers (Citation29). shows the prevalence of smoking in several regional indigenous populations in the Arctic obtained by the Survey of Living Conditions in the Arctic.
Fig. 9. Proportion of non-smokers among the adult population in selected Arctic indigenous populations. Note: Based on data in Results Table 288 of the Survey of Living Conditions in the Arctic www.arcticlivingconditions.org [cited 2014 Dec 20].
![Fig. 9. Proportion of non-smokers among the adult population in selected Arctic indigenous populations. Note: Based on data in Results Table 288 of the Survey of Living Conditions in the Arctic www.arcticlivingconditions.org [cited 2014 Dec 20].](/cms/asset/a16166ce-a532-4d7a-ba3e-5f65fad41beb/zich_a_11821011_f0009_ob.jpg)
The high incidence of lung cancer among men in Russia and its northern regions contrasts with the very low incidence among women. According to the 2009 Global Adult Tobacco Survey, about 55% of Russian men were daily smokers, compared to only 16% among Russian women (Citation30).
In addition to smoking, other cancer risk factors include heavy alcohol use, low dietary intake of fruits and vegetables, obesity and physical inactivity. Changes in the population prevalence of these health determinants have occurred among Arctic populations as they experienced relatively rapid social, cultural, economic and political change (Citation2). It should be recognized that given the long lag time for cancer to develop, even if smoking and other risk factors are dramatically reduced today, it would be decades before any impact on cancer rates would be observed.
For breast cancer, genetic susceptibility may be an important risk factor, as a BRCA1 founder mutation has been found in the Greenlandic population, though not studied elsewhere in the Arctic (Citation31). Another consideration is environmental contaminants such as persistent organic pollutants (POPs) including perfluorinated compounds which may increase the risk of breast cancer possibly in conjunction with certain genetic polymorphisms involved in carcinogen activation (Citation31). POPs such as polychlorinated biphenyls and organochlorine pesticides are found at very high levels in the Arctic population (Citation32).
The low risk of prostate cancer among Inuit contrasted with high risk among the Athabaskan/Dene has been previously observed in Alaska (Citation33); however, the reasons are obscure. It is unlikely the result of differential screening rates. In neither group is population-wide screening with prostate-specific antigen practiced.
Cervical cancer results from infection with the human papilloma virus (HPV), which is sexually transmitted. Greenland has among the world's highest incidence rate of gonorrhoea and chlamydia infection (Citation34), and thus the high risk of cervical cancer is not unexpected. However, Nunavut has comparable rates of sexually transmitted diseases, and yet it has a much lower burden of cervical cancer. One likely explanation is the effectiveness of Pap smear screening. Prior to 2000 Nunavut was the jurisdiction with the lowest screening participation rate in Canada. However, by 2005, the proportion of women in the 3 northern territories aged 18–69 who had at least one Pap test during the preceding 3 years exceeded the Canadian national average (Citation35). The implementation of HPV vaccination programmes can be expected to have long term impact on cervical cancer incidence.
This study focuses only on the surveillance component of cancer control. In the face of increasing cancer risk among circumpolar populations, a variety of effective preventive strategies can be used to reduce the public health impact of cancer. This could involve primary prevention targeting health risk behaviours (smoking, diet, physical activity, etc.), certain vaccinations (against HPV and hepatitis B infection) and early detection through screening (mammography and Pap smear). Continuing epidemiological surveillance of cancer in Arctic regions will also serve the purpose of monitoring the progress and impact of interventions.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Acknowledgements
This project was endorsed by the Arctic Council in the October 2013 meeting of Senior Arctic Officials in Whitehorse, Yukon, Canada. The authors acknowledged the assistance of Dr. Kami Kandola, former Chief Public Health Officer of the Northwest Territories, and Dr. Maureen Baikie, Chief Public Health Officer of Nunavut, in extracting data from their respective territorial cancer registries. The opinions expressed in this article represent those of the authors only and not those of the Arctic Council or any of the health and statistical agencies which have contributed data to the project.
Related Research Data
References
- Chatwood S, Bjerregaard P, Young TK. Global health – a circumpolar perspective. Am J Public Health. 2012; 102: 1246–9.
- Young TK, Bjerregaard P. Health transition in arctic populations. 2008; Toronto: University of Toronto Press.
- Young TK, Rawat R, Dallmann W, Chatwood S, Bjerregaard P. Circumpolar Health Atlas. 2012; Toronto: University of Toronto Press.
- Friborg J, Koch A, Wohlfarht J, Storm HH, Melbye M. Cancer in Greenlandic Inuit 1973–1997: a cohort study. Int J Cancer. 2003; 107: 1017–22.
- Lanier AP, Kelly JJ, Maxwell J, McEvoy T, Homan C. Cancer in Alaska Natives 1969–2003. Alaska Med. 2006; 48: 30–59.
- Carrière GM, Tjepkema M, Pennock J, Goedhuis N. Cancer patterns in Inuit Nunangat: 1998–2007. Int J Circumpolar Health. 2012; 71: 18581.
- Friborg JT, Melbye M. Cancer patterns in Inuit populations. Lancet Oncol. 2008; 9: 892–900.
- Circumpolar Inuit Cancer Review Working Group Kelly J, Lanier A, Santos M, Healey S, Louchini R, etal. Cancer among the circumpolar Inuit, 1989–2003. II. Patterns and trends. Int J Circumpolar Health. 2008; 67: 408–20.
- Engholm G, Ferlay J, Christensen N, Bray F, Gjerstorff ML, Klint A, etal. NORDCAN-a Nordic tool for cancer information, planning, quality control and research. Acta Oncol. 2010; 49: 725–36.
- International Agency for Research on Cancer. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. [cited 2014 Dec 20]. Available from: http://globocan.iarc.fr .
- Forman D, Bray F, Brewster DH, Gombe Mbalawa C, Kohler B, Piñeros M, etal. Cancer incidence in five continents, Vol. X (electronic version). 2013; Lyon: IARC. [cited 2014 Dec 20]. Available from: http://ci5.iarc.fr .
- Malignant Neoplasms in Russia (Incidence and Mortality). Moscow: P.A. Hertzen Research Institute of Oncology. Annual [In Russian]. [cited 2014 Dec 19]. Available from: www.oncology.ru/service/statistics/ .
- Vaktskjold A, Lebedintseva JA, Korotov DS, Tkatsjov AV, Podjakova TS, Lund E. Cancer incidence in Arkhangelskaja Oblast in northwestern Russia. The Arkhangelsk Cancer Registry. BMC Cancer. 2005; 5: 82.
- Kelly JJ, Schade TL, Starkey BM, White S, Ashokkumar R, Lanier AP. Cancer in Alaska Native People, 1969–2008: 40-year report. 2012; Anchorage, AK: Alaska Native Tribal Health Consortium.
- Northwest Territories Department of Health and Social Services. Cancer in the northwest territories, 1990–2000: a descriptive report. 2003; Yellowknife: Government of the Northwest Territories.
- Nunavut Department of Health. Cancer in Nunavut 1999–2011. 2013; Iqaluit: Government of Nunavut.
- Haldorsen T, Tynes T. Cancer in the Sami population of North Norway, 1970–1997. Eur J Cancer Prev. 2005; 14: 63–8.
- Hassler S, Sjölander P, Grönberg H, Johansson R, Damber L. Cancer in the Sami population of Sweden in relation to lifestyle and genetic factors. Eur J Epidemiol. 2008; 23: 273–80.
- Soininen L, Järvinen S, Pukkala E. Cancer incidence among Sami in Northern Finland, 1979–1998. Int J Cancer. 2002; 100: 342–6.
- Hassler S, Soininen L, Sjölander P, Pukkala E. Cancer among the Sami – a review on the Norwegian, Swedish and Finnish Sami populations. Int J Circumpolar Health. 2008; 67: 421–32.
- Dudarev AA, Chupakhin VS, Odland JØ. Cancer incidence and mortality in Chukotka, 1997–2010. Int J Circumpolar Health. 2013; 72: 20470. [PubMed Abstract].
- Zaridze DG, Marochko A, Basieva T, Duffy SW. Cancer incidence in the native peoples of Far Eastern Siberia. Int J Cancer. 1993; 54: 889–94.
- Sjölander P. What is known about the health and living conditions of the indigenous people of northern Scandinavia, the Sami?. Global Health Action. 2011; 4: 8457.
- Soininen L, Pukkala E. Mortality of the Sami in northern Finland 1979–2005. Int J Circumpolar Health. 2008; 67: 43–55.
- Hildes JA, Schaefer O. The changing pattern of neoplastic disease in the western and central Canadian Arctic (1950–1980). Can Med Assoc J. 1984; 130: 25–33.
- Kelly JJ, Lanier AP, Alberts S, Wiggins CL. Differences in cancer incidence among Indians in Alaska and New Mexico and U.S. Whites, 1993–2002. Cancer Epidemiol Biomarkers Prev. 2006; 15: 1515–9.
- Alaska Department of Health and Social Services. Health Risks in Alaska among Adults: Alaska Behavioral Risk Factor Survey 2009 Annual Report. 2011; Anchorage, AK: DHSS, Division of Public Health.
- Wallace S. Inuit health: selected findings from the 2012 aboriginal peoples survey. 2014; Ottawa: Statistics Canada. Cat.No.89-653-X.
- Dene Nation. First Nations Regional Health Survey Report, 2008–2010. 2012; Yellowknife: Dene Nation.
- World Health Organization. Global Adult Tobacco Survey: Russian Federation. 2009. [cited 2014 Dec 20]. Available from: http://www.who.int/tobacco/surveillance/en_tfi_gats_russian_countryreport.pdf .
- Fredslund SO, Bonefeld-Jørgensen EC. Breast cancer in the Arctic – changes over the past decades. Int J Circumpolar Health. 2012; 71: 19155.
- Donaldson SG, Van Oostdam J, Tikhonov C, Feeley M, Armstrong B, Ayotte P, etal. Environmental contaminants and human health in the Canadian Arctic. Sci Total Environ. 2010; 408: 5165–234.
- Snyder OB, Kelly JJ, Lanier AP. Prostate cancer in Alaska Native men, 1969–2003. Int J Circumpolar Health. 2006; 65: 8–17.
- Gesink Law D, Rink E, Mulvad G, Koch A. Sexual health and sexually transmitted infections in the North American Arctic. Emerg Infect Dis. 2008; 14: 4–9.
- Statistics Canada. CANSIM Table 105-4042. Pap smear, females aged 18 60 69, Canada, provinces, and territories. Pap smear, females aged 18 60 69, Canada, provinces, and territories. [cited 2014 Dec 21]. Available from: http://www5.statcan.gc.ca/cansim/a05?lang=eng&id=01054042 .